A staged approach to managing dry eye disease can positively impact a patient’s quality of life.
Nikola, whose name has been changed for privacy, walked into my practice with a warm smile. It was about her fifteenth consult in four years. I checked in on how she was and how her job was going. She quickly opened up and I realised Nikola’s forced smile was just her being polite. As she started to talk, it only took moments for her to completely break down.
Nikola said she was going through a really bad patch with her dry eye symptoms. Since her last consultation, only a few months before, they had really begun to affect her quality of life.
She said she had complied with everything her dry eye specialist and I had recommended and prescribed for her. Having come to know her over time, I felt confident she was being absolutely honest. She described the artificial lubricants; fluorometholone (FML); serum; punctal plugs; azithromycin; cyclosporine; Optimel honey; meibomian gland expression and hot compress management.
Nikola is finally getting considerable relief from her symptoms, and she says, “I really feel like I can live again
She said nothing was really helping.
Nikola was even wearing protective wind goggles outside, as well as inside, which made her feel terribly self-conscious. She wondered whether people looked at her, and judged her when she had them on, but there was no way she could live without them.
Nikola works hard and when she’s not at the office, she loves walking, going to the beach, and getting outdoors, but she wasn’t able to enjoy any of these activities anymore. Her eyes were getting very sore with computer work and concentrating in meetings. Walks were painful on her eyes with the ambient wind. The sunny beach dried out her eyes. Even doing the grocery shopping was tricky because the freezer section was intolerable. In short, she told me that dry eye disease was impeding her ability to work, and robbing her of her quality of life. Nikola broke down again as she told me that she was so tired of the symptoms that it was becoming hard to keep going. She felt incredibly disheartened.
MOVING AHEAD WITH MANAGEMENT
I helped Nikola as much as possible. I assessed her tear film, and her meibomian glands, and I explained that her tear break up time looked a little worse than her last visit, but reassured her that, clinically, very little looked like it had changed, which meant once this hump in symptoms receded, things would improve.
We did a blephasteam and meibomian gland expression, which we knew would alleviate her symptoms to an extent; and then, because her current regimen was not managing her symptoms, I raised the option of scleral contact lens management.
I explained that for more advanced cases of dry eye, scleral lenses should be considered an option to relieve the symptoms.
The Tear Film and Ocular Surface (TFOS) Dry Eye Workshop II Report (DEWS II) recommends consideration of therapeutic contact lens options (soft bandage contact lenses or scleral contact lenses) if other conservative treatment options are inadequate, such as prescribed artificial tears, lid therapy, topical pharmacological agents, serum, and punctal plugs.1 Additionally, DEWS II says it is important that other masquerade conditions that could be causing dry eye symptoms are ruled out.1
As TFOS DEWS II shows, scleral contact lenses should be considered before prolonged use of topical corticosteroids, systemic anti-inflammatories, as well as before surgical punctal occlusion and other more invasive surgical approaches.1 Contributing to DEWS II, there are many studies such as Bavinger et al, that show scleral contact lenses are efficacious and well tolerated, and that most patients prescribed scleral contact lenses report improved visual acuity and relief of dry eye symptoms.2
Recommendations for the staged management and treatment of dry eye disease can be found in the TFOS DEWS II report available at www.tfosdewsreport.org
Nikola thought scleral contact lenses sounded interesting, but she wanted to think about it first and to ask her ophthalmologist for his thoughts – and fortunately, he agreed.
I prescribed Custom Katt Irrregular Corneal Design (ICD) miniscleral lenses for her:
KattICD
RE 6.89/16.50/4200/-5.00/-0.75 x 80 Boston XO Engraved R VA 6/6
LE 7.18/16.50/4100/-3.75/-1.00 x 91 Boston XO Engraved L VA 6/6
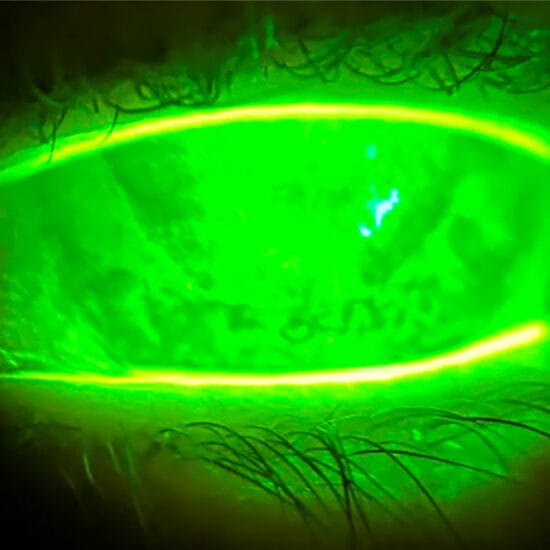
When assessing any scleral lenses, it is critical for the lens to display corneal clearance over the entire surface of the cornea of at least 100 to 150 microns. Trial lenses are placed on the eye, and assessed by creating a thin optic section or parallelepiped on the corneal surface. It helps if you move your oculars to the patient’s temporal side so that you can view the cornea through the slit lamp on a large tangent, and make the light beam come onto the cornea from the nasal side of the patient.
The white arrows in Figure 3 show the first whitish transparent layer of the contact lens, which indicate central contact lens thickness. In this lens, the lens thickness is approximately 240 microns.
The next layer, indicated by the green NaFl and the green arrows, is the post lens tear film. In this case, it looks to be at least twice as thick as the central contact lens thickness, ie. approximately 500 microns.
The grey arrows indicate the optic section of Nikola’s cornea, which as we know for an average eye, would be approximately 550 microns. This can also be used as a guide for judging your post lens thickness.
When a scleral lens is initially placed on the eye, it will sit on the spongey, squishy conjunctiva overlying the sclera. Over time, it will sink into the conjunctiva by approximately 100-200 microns.
It is essential that the lens maintains a minimum of 100 microns in the post lens tear film over the cornea. The ideal lens would initially show a post lens tear film of (200 + 100 = 300 microns). Now, note the initial contact lens thickness is approximately 240 microns. A helpful way to quickly determine if the lens is the correct sagittal height is to determine whether post lens tear film thickness is approximately equal to the apparent contact lens thickness.
On initial trial lens fitting, to save time, the lens can be quickly changed before it settles, based on where it looks as the lens is first placed on the eye. As an example, if this was the appearance of the lens in Figure 3, as it was initially placed on the eye, a new lens with 100–200 microns less in sag height should be placed on the eye; then a refraction over the contact lens would be performed over the lens to incorporate into the intended lens design; and the scleral landing zone would be carefully assessed to avoid blanching of the conjunctival and scleral vessels to determine the final optimal lens.
RELIEF AT LAST
By the time Nikola came to see me for her third follow up visit, her scleral lenses had become an essential part of her life. Today she wears them five to seven days a week, and reports, “The sclerals are very, very good and they definitely help my dry eye”. Although they do not make all her symptoms go away, Nikola says she rarely needs to wear her protective wind goggles and she feels that her eyes can handle a lot more – they no longer feel as fragile as they once did.
Nikola still follows her basic dry eye regimen of using lubricants and hot compresses, however she no longer uses FML, and she has reduced her reliance on most of the other treatments, especially, the constant use of remoisturising eye drops. Nikola is finally getting considerable relief from her symptoms, and she says, “I really feel like I can live again”.
Psychologist Milton Erickson said, “Life will bring you pain all by itself. Your responsibility is to create joy”. I believe that by helping patients like Nikola, we create and return moments of joy to their lives.
Dry eye disease can have a profound impact on a patient’s quality of life and it’s optimal management requires a methodical, staged approach. If a patient has already been prescribed artificial tears, lid therapy, topical pharmacological agents, serum, and punctal plugs without relief, it is appropriate to consider therapeutic contact lens options such as scleral contact lenses.
Margaret Lam is an optometrist in theeyecarecompany practices in greater Sydney and Sydney CBD and an Adjunct Senior Lecturer at the School of Optometry and Vision Science at UNSW. She also works as the Head of Optometry Services for George and Matilda Eyecare. Margaret practises full scope optometry, but with a passionate interest in contact lenses,retail aspects of optometry and successful patient communication and management. She has extensive experience in specialty contact lens fitting in corneal ectasia, keratoconus and orthokeratology and is a past recipient of the Neville Fulthorpe Award for Clinical Excellence. Margaret writes ‘mipatient’ on alternate months with Jessica Chi.
References:
1. Craig JP, et al., TFOS DEWS II Report Executive Summary, The Ocular Surface (2017), pg 10, Table 4. http://www.tearfilm.org/public/TFOSDEWSII-Executive.pdf
2. Bavinger JC, DeLoss K, Mian, SI. Current Opinion in Ophthalmology. 26(4):319–324, JUL 2015 DOI: 10.1097/ ICU.0000000000000171