
An Australian guideline, developed, implemented, and supported with training, is standardising initial therapy for herpes simplex keratitis. As a result, 80% of patients are now receiving the recommended antiviral medications compared to 73% prior to implementation. Steps are being put in place to sustain and broaden the reach of this comprehensive guide.
Herpes simplex keratitis (HSK) is an important infectious cause of unilateral blindness, as it causes permanent corneal scarring, in developed countries (Figure 1).1,2 One fifth of people with ocular herpes simplex virus (HSV) develop corneal stromal disease with the attendant risk of blindness.3 Worldwide, the incidence of HSK in 2012 was estimated at about 1.5 million, with 40,000 new cases of severe monocular visual impairment or blindness each year.1,2 Despite the availability of antiviral and topical corticosteroid agents, complications such as corneal scarring, vascularisation and blindness still occur.4,5
One fifth of people with ocular herpes simplex virus (HSV) develop corneal stromal disease with the attendant risk of blindness

Figure 1. Stromal herpes simplex keratitis
without ulceration.
Diverse prescribing trends for HSK at the Sydney Eye Hospital were identified in 2012–2013. Only a third of the patients with stromal HSK received topical corticosteroids in addition to anti-viral medication. Topical corticosteroids may have not been prescribed due to lack of confidence or knowledge in diagnosing HSK, insufficient senior supervision for trainees, fear of worsening the outcome of possible bacterial, fungal or acanthamoeba keratitis, and concerns regarding adequate follow up of patients.4
The diversity arose as existing evidence for HSK treatment available from other countries was not directly applicable to Australia. Therefore, the Save Sight Institute, in collaboration with the Sydney Eye Hospital, developed a local guideline to standardise initial therapy for HSK with its subsequent implementation and evaluation.6 Furthermore, a video explaining the signs of the different types of HSK has been made to assist trainees to adequately diagnose this condition.
TYPES OF HERPES SIMPLEX KERATITIS
A diagnosis of HSK is mainly made clinically after assessing the patient’s history, symptoms and signs. Investigations are performed for atypical or complicated cases or when the diagnosis is uncertain. Many terms have been used to describe the types of HSK, such as ‘immune stromal’, ‘necrotising’, ‘disciform’, and ‘endotheliitis’. These terms are not well understood and can be confusing.
A simple classification system, based on the layer of the cornea affected by the virus, was introduced in Herpes Simplex Virus Keratitis: A Treatment Guideline by the American Academy of Ophthalmology (AAO) in 2014.6 The system classifies HSK as follows:
- Epithelium: epithelial HSK (alternateterms: dendritic epithelial ulcer orgeographic epithelial ulcer),
- Stroma:
o stromal HSK with ulceration (alternate terms: immune stromal keratitis, necrotising keratitis), and
o stromal HSK without ulceration (alternate terms: non-necrotising keratitis/interstitial keratitis),
- Endothelium: endothelial HSK (alternateterms: disciform/endotheliitis).

Figure 3. Stromal herpes simplex keratitis with ulceration.
Epithelial HSK
Epithelial HSK is characterised by the presence of a punctate, linear, dendritic or geographic lesion (Figure 2).2,3,8 This lesion is caused by direct invasion and active replication of the virus.8,9 It starts as fine granular spots developing into a punctate epithelial keratopathy. Then, the epithelial cells’ nuclei become overloaded with replicating virus, destroying the basement membrane and forming a dendritic shaped ulcer within 24 hours. The ulcer has a branching linear shape with large terminal bulbs, swollen epithelial borders and intraepithelial cell infiltration. The borders stain negatively with fluorescein.8–10 The ulcer may enlarge, forming a geographic or amoeboid ulcer, particularly if topical steroids are given.8,10,11
Stromal HSK
Stromal HSK presents as a recurrent infection accounting for 20–48% of HSK cases; or as the primary manifestation of HSV ocular infection in 2% of cases.
Stromal HSK With Ulceration
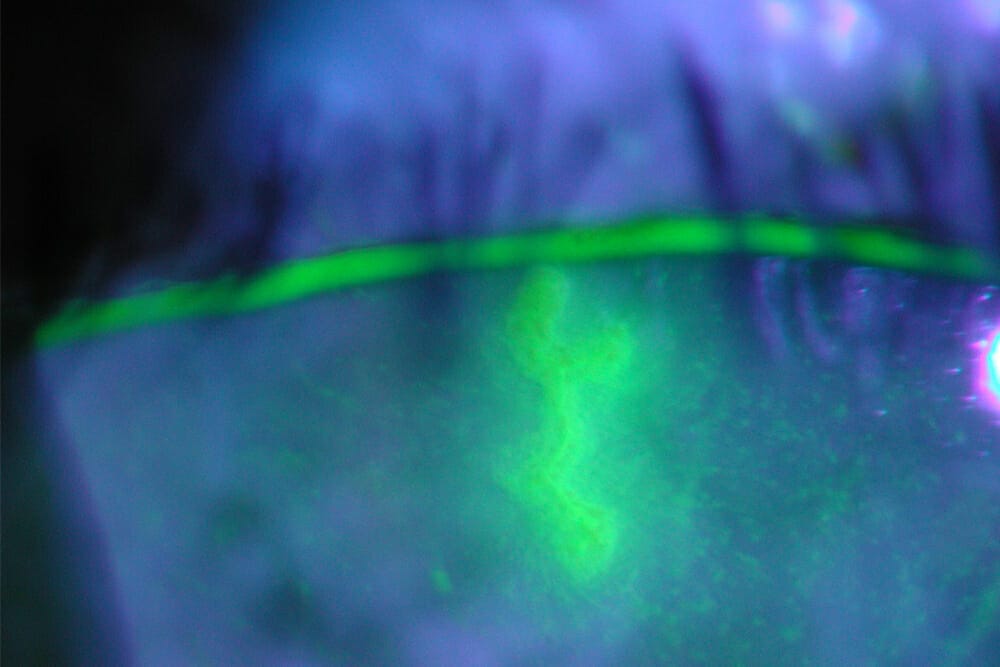
Active viral replication and the immune response cause this type of HSK.8,11 Clinical findings include necrosis and dense infiltration of the stroma with an overlying epithelial defect (Figure 3).2 Greyish white homogeneous abscesses with oedema, keratic precipitates (KPs), severe iridocyclitis, and raised intraocular pressure (IOP) may develop. The epithelium may break down over an abscess. The cornea may be left with oedema, ulceration, and neovascularisation. Cases with severe inflammatory response are often refractory to high dose anti-inflammatories and antiviral medications. This may lead to corneal thinning and perforation, especially when there is superimposed bacterial infection.8,10 This is an eye threatening emergency requiring aggressive management to prevent corneal melting and perforation.11
Stromal HSK Without Ulceration
Stromal HSK without ulceration accounts for 20% of patients with chronic or recurrent disease and is caused by immunemediated destruction of the corneal stroma without virus replication.11 It may present some days or years after an epithelial HSK episode. Generally, the clinical findings include an intact epithelium with different degrees of stromal inflammation (focal, multifocal or diffuse). Anterior uveitis may be associated. Corneal stromal inflammation may be chronic, recurrent, or recrudescent, leading to scarring, thinning, neovascularisation and lipid deposition. Stromal neovascularisation may be sectorial or diffuse and occur in several layers of the cornea (Figure 1).2,8,10
Endothelial HSK
Endothelial HSK, also known as disciform keratitis, has been thought by many clinicians as a category of stromal keratitis. It may better be considered as an inflammatory reaction of the endothelium with secondary stromal and/or epithelial oedema.7 Clinical findings include corneal stromal and epithelial oedema, in a round or oval distribution, with KPs underlying the area of oedema and iritis.2,3,8,9
Keratouveitis
Keratouveitis is a rare manifestation of primary HSV ocular infection; it most commonly occurs in recurrent disease. Herpes simplex virus reaches primarily the anterior segment of the eye through sensory innervation affecting the endothelium secondarily.8 Clinical findings include corneal epithelial and/ or stromal oedema, stromal keratitis, fine KPs, endotheliitis, and anterior chamber cells (mild to severe) and flare.8,12 Focal iritis, posterior synechiae, iris masses, haemorrhages, and hyphema may occur. The uveitis commonly presents with non-necrotising or endothelial HSK; diffuse endothelial HSK usually presents with uveitis.8

Table 1
HSK TREATMENT GUIDELINE DEVELOPMENT AND IMPLEMENTATION
The RNAO Toolkit: Implementation of Best Guidelines was used as a guide for developing, implementing, and evaluating the HSK treatment guideline.13 After identifying the knowledge gap, local corneal experts, uveitis experts and dispensing pharmacists were surveyed to form the implementation team. A consensus meeting with these specialists determined the HSK treatment guideline. The guideline contained dosing and frequency of antiviral medications and topical corticosteroids for adult and paediatric patients, and recommendations for renal dosing and pregnancy (Table 1).
After the hospital’s Drug and Therapeutics Committee guideline approval, the implementation phase was carried out. The implementation strategies included printed and online educational materials for clinicians (lanyard cards, and A4-size laminated posters for consultation rooms with an electronic version uploaded into the hospital’s intranet, Save Sight Institute website, and the Sydney Eye School website), and educational meetings such as the Australian and New Zealand Corneal Society meeting. An audit, post-guideline implementation, was conducted and results were compared to the pre-implementation retrospective case review.4 A web-based survey was created to assess clinician awareness, usage and level of knowledge of the guideline. Of patients, 80% (51/64) received the recommended antiviral compared to 73% (163/223) prior to implementation (p=0.331). Of clinicians, 73% (30/41) were aware and used the treatment guideline.6
A sustainability plan included continual education, annual audits and meetings with the consensus group. As a result of the annual meetings the guideline was revised in 2018 with new recommendations for epithelial HSK and endothelial HSK. Updated lanyard cards were provided, and A4-size posters were placed in emergency and outpatient consultation rooms.
HSK Guideline Success
A post-implementation audit and a webbased survey reported a successful and moderate adherence to the HSK treatment guideline.6 A sustainability plan is warranted to maintain a high level of adherence to the guideline. Educational lectures may be valuable to new and old trainees annually,14 and sustainability evaluations and feedback will be needed at three years post-guideline implementation.15 Future projects include the inclusion of the local treatment guideline into the Sydney Eye Hospital Ophthalmic Pharmacopoeia mobile application, and perhaps consideration of its addition to the hospital’s Electronic Medical Records software as a reminder when antiviral medications are prescribed for HSK.5
Acknowledgements
Dr Yves Kerdraon, Dr Richard Symes, Prof Peter McCluskey, A/Prof Chameen Samarawickrama, Cathy Vlouhos and Prof William Rawlinson contributed to guideline development.
Dr Maria Cabrera-Aguas, MBBS, MIPH, PhD is a Post-doc Research Associate in the Corneal Research Group at the University of Sydney-Save Sight Institute. Her thesis project focused on the development, implementation and evaluation of a treatment guideline for herpes simplex keratitis at the Sydney Eye Hospital. She is a member of the Association for Research in Vision and Ophthalmology (ARVO) Diversity Initiatives Committee. Her research interest includes corneal infections and ophthalmic public health and epidemiology.
Professor Stephanie Watson Sc(Med) (Hons I), MBBS (Hons I), PhD, FRANZCO is a clinician researcher and innovator. She is head of the Corneal Research Group at the Save Sight Institute and a Sydney Medical School Foundation Fellow. She has published over 123 articles in high-ranked peer reviewed journals and book chapters and holds international patents. Professor Watson has given over 202 presentations at national and international meetings. As Chair of the Ophthalmic Research Institute of Australia; Expert Advisor to the Stem Cells Therapy Mission; Editor for the Cochrane Eyes and Vision Group UK; and Chair elect to Association for Research in Vision and Ophthalmology (ARVO) Outreach and Advocacy committee and on the NSW Branch Committee for RANZCO she contributes to policy.
References
- Farooq A, Shukla D. Herpes Simplex Epithelial and Stromal keratitis: An epidemiologic Update. Surv Ophthalmol. 2012;57(5):448-62.
- Watson S, Cabrera-Aguas M, Khoo P. Common eye infections. Aust Prescr. 2018;41(3):67-72.
- Guess S, Stone DU, Chodosh J. Evidence-Based Treatment of Herpes Simplex Virus Keratitis: A Systematic Review. Ocul Surf. 2007;5(3):240-50.
- Cabrera-Aguas M, Robaei D, McCluskey P, Watson S. Clinical translation of recommendations from randomized trials for management of herpes simplex virus keratitis. Clin Exp Ophthalmol. 2018;46(9):1008-16.
- Cabrera-Aguas M, Robaei D, Watson SL. Outcomes of anti-viral therapy in herpes simplex keratitis. Invest Ophthalmol Vis Sci. 2018;59(9):3650-.
- Cabrera-Aguas M, Kerdraon Y, Symes RJ, McCluskey P, Samarawickrama C, Rawlinson W, et al. Development, Implementation, and Evaluation of Treatment Guidelines for Herpes Simplex Keratitis in Sydney, Australia. Cornea. February 11, 2020- Volumen Publish Ahead of Print.Issue -doi: 10.1097/ ICO.000000000000227.
- White ML, Chodosh J. Herpes Simplex Virus Keratitis: A Treatment Guideline San Francisco: Hoskins Center for Quality Eye Care, American Academy of Ophthalmology; 2014.
- Liesegang TJ. Classification of herpes simplex virus keratitis and anterior uveitis. Cornea. 1999;18(2):127-43.
- Azher TN, Yin XT, Tajfirouz D, Huang AJ, Stuart PM. Herpes simplex keratitis: challenges in diagnosis and clinical management. Clin Ophthalmol. 2017;11:185-91.
- Kaye S, Choudhary A. Herpes simplex keratitis. Prog Retin Eye Res. 2006;25(4):355-80.
- Rowe AM, St Leger AJ, Jeon S, Dhaliwal DK, Knickelbein JE, Hendricks RL. Herpes keratitis. Prog Retin Eye Res. 2013;32:88-101.
- Gritz DC, Feldman BH, Read RW. Herpes simplex uveitis: Eye Wiki. American Academy of Ophthalmology; 2014 [updated 26 June 20198 August 2017]. Available from: http://eyewiki.aao.org/Herpes_simplex_uveitis.
- Registered Nurses’ Association of Ontario. Toolkit: Implementation of Best Practice Guidelines. Toronto, ON: Registered Nurses’ Association of Ontario; 2012.
14. Grol R, Grimshaw J. From best evidence to best practice: effective implementation of change in patients’ care. Lancet. 2003;362(9391):1225-30.
- Ament SMC, de Groot JJA, Maessen JMC, Dirksen CD, van der Weijden T, Kleijnen J. Sustainability of professionals’ adherence to clinical practice guidelines in medical care: a systematic review. BMJ Open. 2015;5(12):e008073.





