Modern-day cataract patients are educated and empowered. With this in mind, it is very important to provide each patient with appropriate information about the lenses available to ideally meet their vision needs.
Multifocal implants have become increasingly popular, as patient demand for spectacle independence increases. More recently, the dual (or top-up) lens procedure, which involves implanting two intraocular lenses during the same surgery, is being used to deliver multifocal correction.
Dr Andrew Apel and Dr Brian Harrisberg share their experiences implanting the 1stQ Addon secondary sulcus supplementary lenses, including the dual lens approach.
Dr Andrew Apel
Prediction of refractive outcomes has become highly accurate as a consequence of modern intraocular lens (IOL) implantation. The vast majority of cases now fall within +/- 0.5 dioptres.1-6 This is the result of improvements in lens formulas, reduction in wound size, more predictable lens positioning, and reliably labelled IOLs.
However, there are cases where the expected refractive outcome is not achieved. In these cases, one of the options for correction is a sulcus based top-up lens.

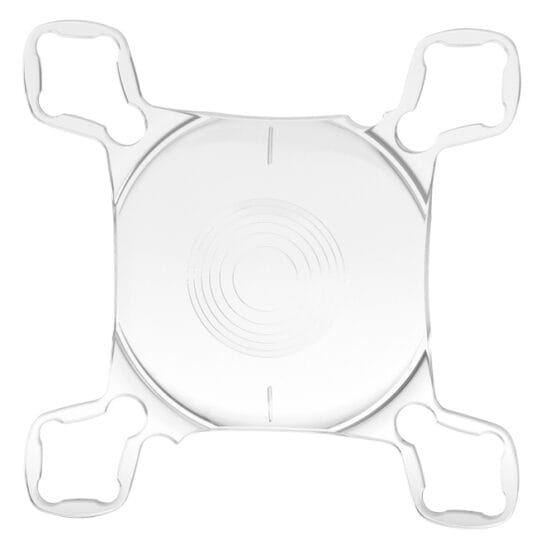
Figure 1. The 1stQ Addon Trifocal toric secondary IOL is designed to be
rotationally stable in the sulcus.
To improve spherical and astigmatic correction, a stable, non-rotating IOL of accurate power is required.
Configuration of the haptics is crucial to prevent rotation. This means that stable astigmatic correction can be achieved, as well as prevention of ciliary body chaffing, which may result in uveitis, glaucoma and hyphema.7 Additionally, as the lens can be injected through a 2.4mm wound, there is no induced astigmatic change.
Ideally, a concave posterior surface allows placement over the top of an existing convex lens, to maintain a consistent lens position, reduce decentration and aberrations. Appropriate (wide enough) interlenticular space helps to avoid interlenticular opacification and hyperopic shift, and hence ensure good and stable visual outcomes in the long-term.7
The 1stQ AddOn sulcus-based IOL family, (Medicontur Medical Engineering Ltd, Zsámbék, Hungary) has all the above features. The inventor of these lenses, Rüdiger Dworschak, designed his first sulcus lens in 1998. After collecting 10 years of experience and using it to design the latest platform, he came up with the current design in 2008. Implantations using the current patented design started in Europe in 2010. Sales of 1stQ AddOn lenses began in Australia in June 2016 with Insight Surgical (Paragon Care, Australia) becoming the distributor in 2018.
Reasons for implanting AddOn lenses include managing residual refractive error in pseudophakic patients, or refractive error post-monofocal or multifocal implant patients. There is also the option of upgrading pseudophakic patients to multifocality with the option of relatively safe reversibility at any time in the future.

Figure 2. The order summary page from the 1stQ AddOn calculator website.
Contraindications include the preoperative presence of pigmentary dispersion syndrome, especially in the presence of glaucoma or elevated intraocular pressure (IOP). Patients who have loose zonules from trauma, or pseudoexfoliation, are also not good candidates for supplementary IOLs.7
The 1stQ AddOn lenses are specifically designed to create a stable sulcus-based lens that maintains angular position and centration in the eye.8-11 The lenses are made from clear, foldable hydrophilic acrylic material. The refractive index of the material is 1.46 and the Abbe-number is 58, which is high enough to ensure good visual quality.12 The toric model has the cylinder correction on the front surface with two axis marker lines.
Other combinations of lens on this platform include a trifocal, a trifocal toric, and the Scharioth Macula Lens (SML). This latter IOL has a high-powered central addition for macular degeneration patients.13
The trifocal toric is the latest member to join Medicontur’s AddOn family, having been available worldwide since late-2018. The AddOn trifocal and trifocal toric lenses are provided with addition powers of +3.0 and +1.5D in the sulcus plane (near reading adds of 37.5cms and 74cms).
The range of powers available are -10.0 to +10.0D in 0.25D increments for the monofocal model. Monofocal torics are available in spherical equivalent (SE) powers -10.0 to +10.0D in 0.25D steps and cylinders (Cyl) 1.0 to 11.0D. Trifocal/ progressive lenses are available in powers -5.0 to +5.0D (including plano power) and trifocal toric/progressive toric lenses are available in SE powers -3.0 to +3.0 with cylinders 1.0 to 4.5D. All lens models are listed on the prostheses list.
Calculation of lens power is based on subjective refraction; and as more data is added (anterior chamber depth, axial length, keratometry and age), the predictability of the vergence based algorithm increases. Information regarding the type and power of the IOL already inside the capsular bag can be entered, but is not essential.14 The minimum recommended pseudophakic anterior chamber depth is 3.0mm (measured from the corneal epithelium), so that the risk of developing secondary glaucoma and/ or other adverse events can be minimised. A peripheral iridotomy/iridectomy is not recommended by the manufacturer.
Waiting time for supply depends on availability, and the lens power required. Most lenses can be supplied within a few weeks of being ordered. Lenses with unusual powers can take eight to 10 weeks to order if they need to be specifically manufactured for a given case.
SURGICAL PROCEDURE
The surgery itself can be performed under topical or block anaesthesia. The lens is loaded into a Medicel Accuject 2.1 push style injector with viscoelastic. A cohesive viscoelastic is recommended as this is easier to remove after the IOL has been implanted. The recommended incision size is 2.4mm. Intracameral insertion of the injector into the eye is recommended, though after some experience, wound assist can be used.

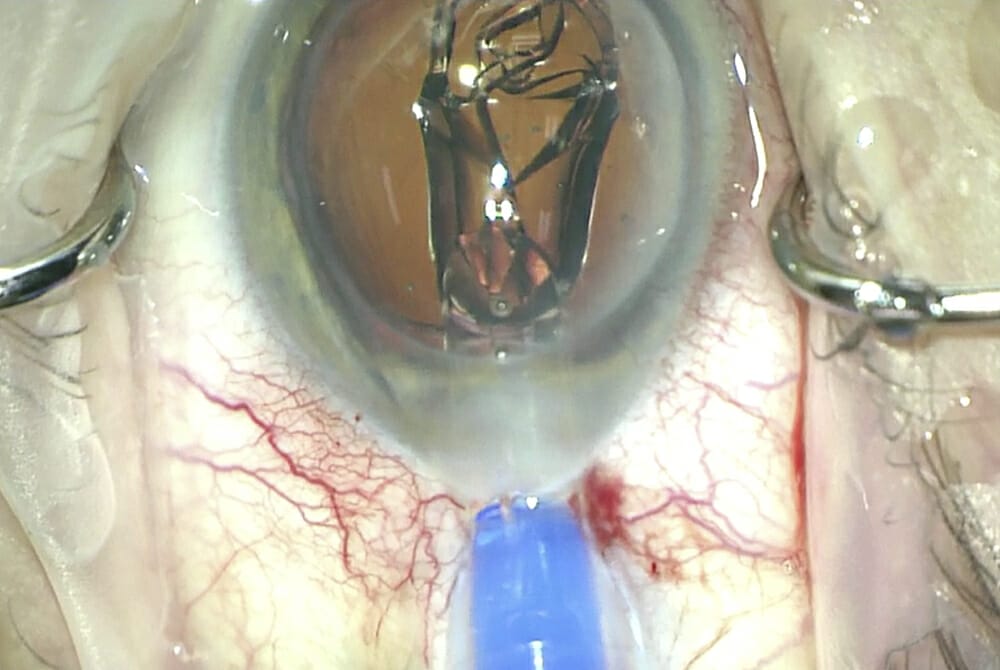
Figure 3. Implantation of a 1stQ Addon lens with the Medicel Accuject 2.1 injector.
Good pupil dilation helps prevent the lens snagging on the iris as it passes over.
Slow injection under viscoelastic is required to allow the leading haptics to unfold in a controlled way without the pressure of the optic emerging from the Medicel injector, as the leading haptics can then be guided under the iris. If the injection is performed with speed, the leading haptic may want to enter the capsular bag – this occurred in one of my cases where the capsulorhexis was larger than the optic behind the preexisting IOL. During injection, the AddOn lens should not be pushed against the primary lens to maintain zonular integrity. Nd:YAG laser capsulotomy performed after primary surgery also significantly increases the rate of anterior vitrectomy, further complicating the secondary IOL procedure: the vitreous may be forced around the optic of the existing IOL and into the anterior chamber.15,16
If the leading haptics cannot be placed into the sulcus during injection, then they can be easily placed in the sulcus from in front of the iris along with the trailing haptics. At this stage, it is important to check that all four haptics are positioned behind the iris before removing the viscoelastic, particularly in patients who have had corneal transplants, as it may be difficult to see the haptics behind the corneal scar.
Due to its design, toric versions of the lens are easier to rotate into position without all four haptics positioned in the sulcus. The lens can be dialled in either direction.
Some pearls for insertion include the use of the microscope during lens loading to avoid trapping haptics in the cartridge, good pupil dilation, slow injection and getting used to the difference between injection of a regular IOL and a supplementary lens, as less space is available in an eye with a pre-existing IOL.
Dr Andrew Apel is a leading corneal and external eye disease physician. Dr Apel completed his ophthalmology training in Brisbane, then undertook a two year Corneal and External Diseases Fellowship at the University of Toronto, Canada in 1992.
With over 25 years of experience in treating medical and surgical conditions of the anterior segment of the eye, Dr Apel has published peer reviewed journals and lectured internationally. He is Chairman of the qualification and education committee of RANZCO Queensland (QLD), Chairman of the medical advisory committee of the QLD Eye Hospital, a Director at QLD Laser Vision, Consultant Ophthalmic Surgeon at the PA Hospital, Chair of the qualification and education committee, which means he is responsible for the supervision of trainee ophthalmologists, member of the specialist advisory committee at Cura Day Surgeries and a member of the Corneal Society Special Interest Group.
Outcomes with the Dual Lens Procedure
Dr Brian Harrisberg
Cataract surgery today is considered a refractive procedure thanks to improved technological advances and surgical techniques. This facilitates spherical equivalent outcomes within ±0.50 dioptres in up to 90% of cases.1-6
I have performed cataract surgery with inthe- bag multifocal intraocular lenses (IOLs) for several years. More recently, I have offered the dual lens procedure to a select group of patients. This procedure involves the implantation of two IOLs during the same surgery, with the aim being multifocal correction. This is dependent on an accurate and safe insertion of the monofocal or monofocal toric IOL into the capsular bag. Immediately thereafter, a plano powered trifocal 1stQ AddOn IOL is placed above the original lens into the sulcus. The dual procedure offers a safe and reversible solution for patients who are unsure about receiving multifocal in-the-bag implants. Moreover, the ability to reverse the procedure can be very useful in situations where patients are prone to develop ocular disease later in life, such as macular degeneration, in which case removal of the multifocal component may be advantageous to the patient to maximise contrast sensitivity. The ease of removing a sulcus lens, and leaving the full corrective power for distance correction, is essentially a ‘get out of jail free’ card. It allows the patient to have the procedure reversed without affecting visual acuity.
Retrospective Analysis
I recently presented the results of a retrospective analysis, which compared the refractive and visual outcomes of 72 eyes (43 cataract patients) studied in three groups: in patients implanted with the trifocal inthe- bag Medicontur Liberty 677MY IOL (Medicontur Medical Engineering Ltd, Zsámbék, Hungary); in patients with the toric model of the same capsular bag lens; and in patients receiving a monofocal primary lens supplemented with the Medicontur 1stQ AddOn trifocal secondary IOL.7
The 1stQ AddOn is a platform specifically designed to fit into the sulcus (Figure 1). These are square-shaped hydrophilic lenses with four haptics, which are able to anchor the lens in various sizes and shapes of ciliary sulci. One of the advantages of the 1stQ AddOn sulcus lens is the ability to maintain rotational stability due to the fourpoint fixation design. Gundersen and Potvin reported good data with toric corrections showing axis stability within the sulcus.8

Figure 1. The 1stQ AddOn Trifocal secondary
IOL is designed specifically for sulcus implantation.
Moreover, the 1stQ AddOn lenses have a convex anterior surface and a concave posterior surface on the optic, which allows adequate spacing between the lens in the bag of at least 0.34mm.9-10 This helps to avoid development of interlenticular opacification. Adequate clearance from the iris avoids red rock syndrome and iris chafing.11-13
The 1stQ AddOn trifocal and trifocal toric lenses have six diffractive rings as apodised powers on the anterior surface. This is similar to the Medicontur Liberty trifocal lens, which has seven diffractive rings and is made from the same hydrophilic material.
The trifocal AddOn model has plano power, but it is possible to order this lens in a variety of spherical and cylinder powers as well.
The technique for a dual lens procedure follows a normal cataract operation with insertion of a single piece in-the-bag monofocal or monofocal toric IOL. The toric in-the-bag lens is positioned on axis and all viscoelastic is removed.
The wound is then enlarged to 2.4mm and viscoelastic is placed discreetly above the iris distal to the wound, as well as in the sulcus, allowing an expansion of the sulcus space. The AddOn lens is loaded under the microscope into the Medicel Accuject 2.1 top loaded injector system, allowing good clearance of all the haptics within the injector system. On injecting, the lens can pass into the anterior chamber, or the forward haptics can possibly be positioned into the sulcus from the injector.
Ideally, manipulation of the haptics is best performed away from the wound, with minimal downward pressure. It is possible to rotate one of the four haptics at a time.
Once the lens is located in the sulcus, it is best to rock it forward and backwards, and side to side to make sure that each haptic has unfolded adequately. A sign that a haptic has not unfolded correctly would be a prominence within the iris, suggesting that the haptic is pressing into the posterior iris surface. Once the lens is secured, all viscoelastic must be removed extremely thoroughly, above and in between the two lenses. Intracameral Miochol is used to secure the optic behind the iris. In the recovery room, following a dual procedure, every patient should be examined on the slit lamp for adequate placement of the lens and to ensure that none of the haptics have prolapsed into the anterior chamber.
Post-operatively, uncorrected and bestcorrected visual acuities and subjective refraction were assessed. The difference between the predicted residual refraction and actual post-operative refraction was determined as spherical equivalent, residual cylinder and axis. A patient satisfaction questionnaire was completed three months after surgery. The results of my retrospective analysis showed that outcomes between each of the groups were identical, with no loss of best-corrected or uncorrected visual acuity, hence giving confidence that this procedure is safe and accurate.
Of all patients, 90% or more achieved unaided distance visual acuity of 6/7.5 or better and all obtained N5 reading, in good lighting, in all three groups examined. Dysphotopic events were rare and easily tolerated in all three groups.
According to my personal experience, it appears that the dual lens system offers patients a viable opportunity for reversibility of multifocal implants, whereby the multifocal platform can easily be removed from the sulcus at any time. The primary lens remains within the capsular bag and the original refractive outcome would remain the same.
With informed consent a priority, all options, including distance correction, monovision options, multifocal lenses, and dual lens procedures are discussed with all of my patients. All patients are given ample chair time to understand the concept of the dual procedure.
I do believe the dual lens system offers an opportunity for some patients who are unsure if they will cope with the potential side effects of multifocal lenses. I will reserve this procedure for patients who cannot clearly make up their mind as to which system they would prefer, but do not want to miss an opportunity for spectacle independence. I would recommend the dual implantation approach to surgeons who are already experienced and highly efficient in cataract surgery. Although the 1stQ AddOn lenses are easy to implant, careful and prudent manipulation is essential to achieve the best possible surgical outcomes.
Dr Brian Harrisberg is an expert in cataract surgery, refractive surgery and diabetic eye disease with many years of experience. As one of Australia’s leading ophthalmologists he offers the latest innovations in surgery. Dr Harrisberg is a pioneer in the area of implantation of secondary sulcus pseudophakic intraocular lenses in Australia and was the first surgeon to implant a Scharioth Macula Lens (SML) for macular degeneration in Australia. Dr Harrisberg has published multiple research papers in peer-reviewed journals and regularly presents at local and international meetings.
References
- Kent C (ed.). IOL Power Formulas: 10 Questions Answered – Understanding how formulas calculate the optimum lens power can help ensure good outcomes. Review of Ophthalmology. 2018 Jan 10th, Available from: www.reviewofophthalmology.com/article/iol-power-formulas-10-questions-answered
- Melles RB, Holladay JT, Chang WJ. Accuracy of intraocular lens calculation formulas. Ophthalmology 2017 Sep 23. pii: S0161-6420(17)31428-8. doi: 10.1016/j.ophtha.2017.08.027. [Epub ahead of print]
- Fram NR, Masket S, Wang L. Comparison of intraoperative aberrometry, OCT-based IOL formula, Haigis-l, and Masket formulae for IOL power calculation after laser vision correction. Ophthalmology 2015;122:1096-101.
- Wang L, Shirayama M, Ma XJ, et al. Optimizing intraocular lens power calculations in eyes with axial lengths above 25.0 mm. J Cataract Refract Surg 2011;37:11:2018–27.
- Melles RB, Holladay JT, Chang WJ. Accuracy of intraocular lens calculation formulas. Ophthalmology 2017; Sep 23. pii: S0161-6420(17)31428-8. doi: 10.1016/j.ophtha.2017.08.027. [Epub ahead of print]
- Hill WE, Abulafia A, Wang L, Koch DD. Pursuing perfection in IOL calculations. II. Measurement foibles: Measurement errors, validation criteria, IOL constants, and lane length. J Cataract Refract Surgery 2017:43;7;869-70.
- Manzouri B, Dari M, Claoué C. Supplementary IOLs: Monofocal and Multifocal, Their Applications and Limitations. Asia Pac J Ophthalmol (Phila). 2017;6(4):358-363.
- Reiter N, Werner L, Guan J, Li J, Tsaousis KT, Mamalis N, Srinivasan S. Assessment of a new hydrophilic acrylic supplementary IOL for sulcus fixation in pseudophakic cadaver eyes. Eye (Lond). 2017 May;31(5):802-809. doi: 10.1038/eye.2016.310. Epub 2017 Jan 20.
- Gundersen KG, Potvin R. A review of results after implantation of a secondary intraocular lens to correct residual refractive error after cataract surgery. Clin Ophthalmol. 2017 Oct 3; 11: 1791-1796. doi: 10.2147/OPTH.S144675. eCollection 2017.
- Gundersen KG, Potvin R. Refractive and visual outcomes after implantation of a secondary toric sulcus intraocular lenses. Clin Ophthalmol. 2020; 14:1337-1342.
- Palomino-Bautista C, Sánchez-Jean R, Carmona Gonzales D, Romero Domínguez M, Castillo Gómez A. Spectacle independence for pseudophakic patients – Experience with a trifocal supplementary add-on intraocular lens. Clin Ophthalmol. 2020; 14:1043–1054.
- Zhao H, Mainster MA. The effect of chromatic dispersion on pseudophakic optical performance. Br J Ophthalmol. 2007;91(9):1225-1229.
- Scharioth GB. New add-on intraocular lens for patients with age-related macular degeneration. J Cataract Refract Surg. 2015 Aug;41(8):1559-1563.
- The 1stQ AddOn Onlina Calculator. Available from: www.1stq.de/en/34-addoncalculator
- Leysen I, Bartholomeeusen E, Coeckelbergh T, Tassignon MJ. Surgical outcomes of intraocular lens exchange: five-year study. J Cataract Refract Surg. 2009;35(6):1013-1018.
- Falzon K, Stewart OG. Correction of undesirable pseudophakic refractive error with the Sulcoflex intraocular lens. J Refract Surg. 2012;28(9):614-619.