
Having worked in eye care for the last 30 years, as both a nurse and optometrist, I know that dry eye disease is often poorly understood. It is often of a refractory nature to treat and many eye care practitioners find it frustrating to manage.
Unfortunately, it is our patients who are left suffering. Told they “just have to live with a chronic condition”, they are given limited options to manage it. Some are even advised that their symptoms are psychological.
Five years ago, I decided there had to be a better way.
There is no doubt that dry eye disease (DED) management can be daunting. Right now, 7.4% of Australians are estimated to suffer from this common but debilitating condition,1 and it is likely that its incidence will increase in the future as the paediatric population experiences signs and symptoms of dry eye due to increased screen time.2
The good news is that growing research and investment in therapeutics and technology over the last two decades has finally provided us with tools that can be effective in managing patients with DED. This makes creating your own dry eye clinic easier and more rewarding than you think.
having tools to diagnose and treat challenging dry eye conditions will be personally more rewarding and will lead to even more happy patients!
FIRST STEPS
Over the years several of my colleagues have ventured into the realms of treating dry eye patients, providing interesting opportunities for discussion about the best way forward.
I believe that the first step is to revisit the way you schedule your appointments and charge for your time. In the initial stages you could:
- Incorporate a few DED treatments into your routine care, charging for the individual tests and products used,
- Designate patients as either new or follow-up, allowing 20 to 60 minute appointment slots accordingly, and charging a set fee for these specific consultations, or
- Schedule specific sessions or days to dry eye patient consultations, and for testing and treatments.
I always recommend charging private fees for tests and treatments, and an above schedule fee for eligible MBS item numbers. The fee charged should both realistically cover the cost, and establish a perceived value for your time and expertise. Fee setting can be based on what the individual patient needs at the time, or as a ‘package fee’ that includes say, an initial consultation, diagnostics work-up and a treatment.
Optometry Australia has a private fee calculator to guide you on what to charge for your service, depending on time and equipment invested.
IDENTIFY YOUR DEMOGRAPHIC
Some practitioners are already aware of their existing dry eye patients, others less so. The ‘at risk’ factors to look out for include age, female sex, medications such as tricyclic antidepressants, selective serotonin re-uptake inhibitors, diuretics, beta-blockers, hormone conditions such as thyroid disease or diabetes, androgen insufficiency, auto-immune conditions, allergy and antihistamines just to name a few. That is a large percentage of your patient base!
If you suspect you have the capacity for a dry eye clinic but are not sure how large it could be, start looking for it:
- Use the Standard Patient Evaluation of Eye Dryness Questionnaire (SPEED),3 Ocular Surface Disease Index (OSDI),4 or McMonnies5 questionnaires, or simply devise your own and, over two weeks, ask every existing patient to complete it,
- Look at their tear film using NaFl (sodium fluorescein) staining with the understanding that <10 seconds indicates dry eye,
- Determine whether the patient is symptomatic and note any at-risk medications or conditions, and
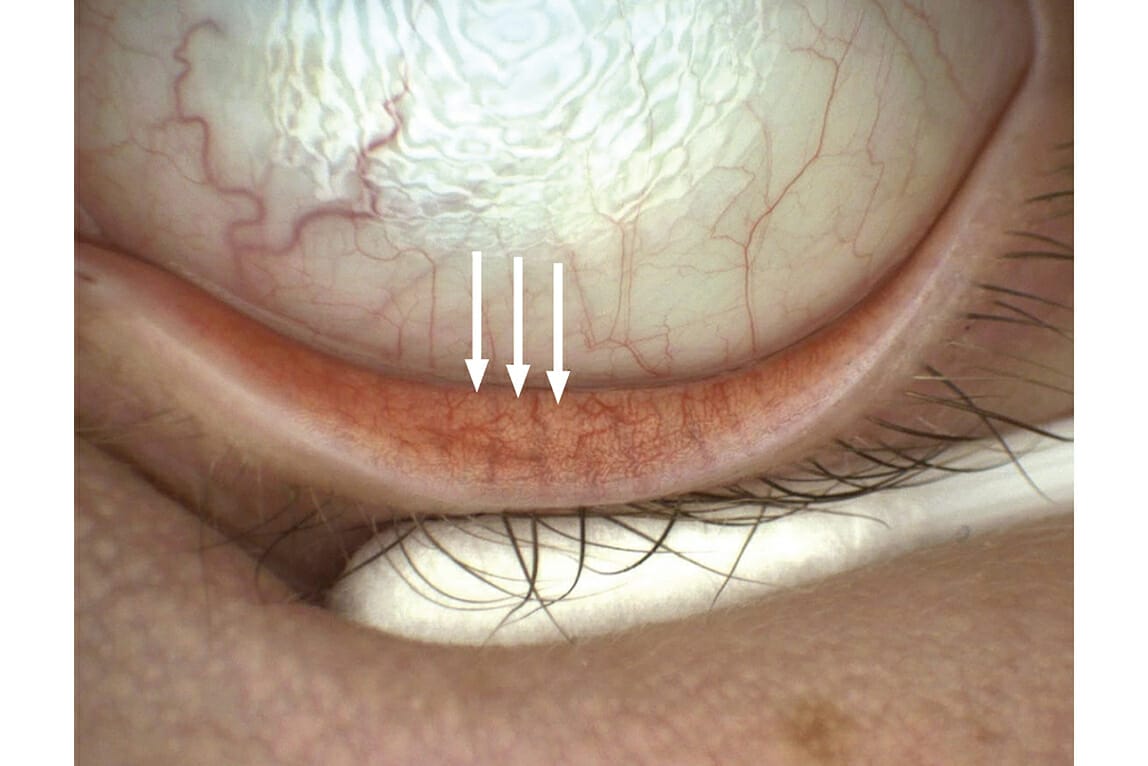
- Evert the lower lids (Figure 1) using the slit lamp and look at the meibomian glands. Are some missing? Are some short? Gently express the meibomian glands at the base of their orifices, just under the lash lines. Is the oil easily expressed; clear; yellowish; or pasty?
Once you’ve done these exercises for two weeks, work out your statistics – how many people actually commented on symptoms simply because you asked them? How many have signs of dry eye?
Manuka honey is both an anti-inflammatory and anti-bacterial agent, which can be used long-term and can be extremely advantageous in treating dry eye symptoms and improving meibum health
RESEARCH AND UP SKILL
Now that you’ve identified the opportunity to establish a dry eye clinic in your practice, it’s time to brush up on your diagnostic and treatment skills.
Although it is useful to identify the primary subtype of DED as either aqueous deficient or evaporative, to establish the first step in treatment, these are no longer considered individual pathophysiological conditions. In fact, the TFOS DEWSII6 consensus is that DED exists on a continuum, and therefore, the subtypes need to be considered, measured and addressed, often concurrently, in context of the patient’s presenting symptoms and signs.
Symptoms vary from dry, burning, stinging, itching, and sore eyes to watery and irritable eyes. Both the ocular surface and lid margins can be red, and patients can complain of eye pain – ranging from stabbing, gritty pain to a dull ache around the eyes. Patients may report increased light sensitivity and often the patient will report pain overnight or difficulty opening the eyes on waking. Many patients will complain of recurrent ‘styes’ along the eyelids and chalazia.
TREATING MILD TO MODERATE DRY EYE
The Cause
A comprehensive patient history is key to good management. Invest at least 30 minutes in your patient’s initial consultation and thorough history taking before undertaking further investigations or providing an in-room heat treatment. Investigations and treatment may be undertaken during the first consult, or at a second scheduled visit.
The Meibomian Glands
Evaporative dry eye is the most common cause of dry eye symptoms,7 making treatment of the meibomian glands the best place to start in most cases.
On average, there are about 20 to 40 meibomian glands on the upper lid and 20 to 30 on the lower lid.8 Their role is to release oil every time the eyelids meet on blinking, which prevents evaporation of the tear film.
In treating meibomian gland dysfunction, the aim is to get the oil, that is released from the glands, liquid and keep it that way.
You can view the meibomian glands using transillumination, your slit lamp or do meibography. Significant meibomian gland drop out will indicate the need for support with artificial oil based tears such as Novatears from AFT Pharmaceuticals rather than more bulk based, viscous options, and perhaps overnight lubricants such as VitaPos.
Mechanical heat of the meibomian glands is the initial mainstay treatment for meibomian gland dysfunction, so invest in dedicated eye masks such as the D.E.R.M mask from Designs for Vision (DFV), the Eye Doctor eye compress (which can be heated in the oven) from Good Optical, or Bruder masks from Optimed.
It’s worth suggesting that your patients purchase a mask for home use and bring it in to the practice for you to use on their eyes for 10 minutes prior to lid expression. This can be done in your chair and, while their lids are being warmed, the time can be used to discuss their progress. The ideal temperature is 42º. Perform gentle oil expression after with a device such as the Mastrota meibomian paddle from DFV. Placed against the palpebral conjunctival surface, it makes expression from the lid surface with your finger or a cotton bud more effective. Artificial tears have a place, but to my mind need to be supplementary rather than a ‘bandage’ solution. Manuka honey is both an antiinflammatory and anti-bacterial agent, which can be used long-term and can be extremely advantageous in treating dry eye symptoms and improving meibum health. Available directly from Jubelee Eye Care, it is available as Optimel 16% drops and 98% gel, is classed as a medical device through the Therapeutic Goods Administration and does not carry GST.
The Lashes
Lid margin disease and anterior blepharitis contribute significantly to dry eye, both as separate conditions or as contributors to meibomian gland disease, chalazia formation and the inflammatory process of dry eye. Common causes are bacterial and demodex mites. The regular use of SteriLid (Contact Lens Centre Australia), a tea tree oil-based lid wipe such as Blephadex (as both a foam and a wipe from Optimed) or OUST Demodex Foam from Good Optical, can promote healthy lid margins.
The Aqueous
The fastest way to retain the tear film on the eye surface is to ‘trap’ the aqueous. Measure aqueous production using a Schirmer or Phenol Red Thread test, then consider the use of punctal plugs, which are easily inserted at the slit lamp and usually offer quick relief if low aqueous is part of the problem. Topical cyclosporine can also improve the lacrimal gland function, although this often needs a commitment from the patient of six to 12 months. Remind patients that in low humidity conditions and air-conditioning they may need to use artificial tears more often. For your patients’ convenience, you may want to stock go-to recommendations for artificial tears, such as Hylofresh or Hyloforte from CLCA in-practice, as well as practitioner-only products.
However far you choose to delve into dry eye, this rapidly emerging area of health is one that will benefit many patients and help grow your practice
The Inflammation
Inflammation is part of the dry eye cascade and can be treated with topical steroids, omega 3 supplementation such as Dry Eye Forte from MD Eyecare or Lacritec by Stiltec, oral doxycycline or compounded cyclosporine. Cequa, when it becomes available through pharmacies, and Xiidra (Lifitegrast), which we hope is imminent, should also be included in your dry eye tool box. If you are not therapeutically endorsed, consider co-management with your local GP or a colleague who is.
THE REALLY FUN STUFF
When you feel confident that you have a handle on DED, it’s time to take your clinic to the next level. Although this requires an investment in equipment, having tools to diagnose and treat challenging dry eye conditions will be personally more rewarding and will lead to even more happy patients!
Investing in a multi-function unit, such as the Oculus Keratograph K5 from Designs for Vision, will also enable you to image meibomian glands as well as measure noninvasive tear break up times, tear meniscus heights, quantify eye redness and lipid layer thickness – all of which is valuable for diagnosis and monitoring progression. Hyperosmolarity, from increased tear evaporation, has been recognised by DEWS1 as a contributor to the dry eye spectrum. Investing in an osmolarity testing unit, such as the Tear Lab from IQ Medical, will add to your understanding of what is happening on the ocular surface.
Products, such as Blephex from Optimed, offer intensive cleaning of the lashes when treating anterior blepharitis, and don’t forget to use bandage contact lenses for persistent corneal defects and corneal erosions.
While investing in the ‘big guns’ with intense pulsed light therapy such as the Eyelight from Opticare, or in Lipiflow may seem daunting, suppliers are on hand to discuss appropriate patients’ fees and the numbers needed to recoup your investment. Again, Optometry Australia has resources to help guide your decisions.
Even high tier levels of DED management involve treatments such as autologous serum and amniotic membrane, but these are usually regarded as treatments for severe and advanced staged dry eye.
CONCLUSION
You and your practice are unique. How much you practise and invest in dry eye is very much up to you and is likely to change as your skill set develops.
However far you choose to delve into dry eye, this rapidly emerging area of health is one that will benefit many patients and help grow your practice. Patient compliance is integral to success and I find patients are generally dedicated to at-home work when they both financially invest in, for example IPL treatment or meibomian gland imaging, and also recognise their optometrist’s commitment to finding a solution for them.
So don’t be afraid to sink your teeth into dry eye management. Make the investment. I can tell you from personal experience, that these patients become very happy people when we can help them.
Dr Jennifer Rayner BAppSc (Optom), GradCertOcTher (UNSW) was a registered nurse before studying optometry. She has practised as an optometrist since 2003 and with her business partner Dr Rene Malingre, established South Australia’s first dedicated dry eye clinic, Alleve Eye Clinic, in 2016.
References
- Gayton JL. Etiology, prevalence, and treatment of dry eye disease. Clinical Ophthalmology 2009;3: 405–412.
- Wu SZ, Chong JK, Tracer N ; Wu M & Raju L. Prevalence of dry eye symptoms and relationship to screen time in a New York City pediatric population. Investigative Ophthalmology & Visual Science 2020; 61(7): 340.
- Pucker AD, Dougherty BE, Jones-Jordan LA, Kwan JT et al. Psychometric Analysis of the SPEED Questionnaire and CLDEQ-8. Investigative Ophthalmology & Visual Science 2018; 59(8): 3307-3313.
- Schiffman RM, Christianson MD, Jacobsen G et al. Reliability and Validity of the Ocular Surface Disease. Arch Ophthalmol 2000;118(5): 615-621.
- Gothwal VK, Pesudovs K, Wright TA & McMonnies CW McMonnies Questionnaire: Enhancing Screening for Dry Eye Syndromes with Rasch Analysis. Investigative Ophthalmology & Visual Science. 2010;51: 401-1407.
- Craig JP, Nelson JD, Azar DT, Belmonte C et al. TFOS DEWS II Report Executive Summary. The Ocular Surface 2017; 15(4): 802-812.
- Lemp MA, Crews LA, Bron AJ, Foulks GN & Sullivan BD. Distribution of aqueous-deficient and evaporative dry eye in a clinic-based patient cohort: a retrospective study. Cornea 2012;31(5): .472-478.
- Butovich IA. Meibomian glands, meibum, and meibogenesis. Experimental eye research 2017;163: 2-16.





