

Pathologic myopia describes structural abnormalities associated with excessive axial elongation in the posterior segment of myopic eyes.1 These abnormalities can occur at the macula, optic disc, and/ or peripheral retina, and they predispose patients to complications such as myopic maculopathy, glaucoma, and retinal detachment.
In this article, Pauline Xu and Dr Angelica Ly zoom in on the macula of the myopic eye, to introduce a systematic and practical approach to aid primary eye care practitioners in diagnosing and managing myopic maculopathy.
Myopia is a 21st Century public health issue and is projected to affect 50% of the world’s population by 2050.2 Dealing with pathologic myopia (alternatively termed ‘pathological myopia’), particularly in the aging population, becomes a high priority for eye care practitioners, given its associated risk of irreversible vision loss.
Despite the challenges, applying multi-modal imaging on myopic eyes is paramount due to the inherent limitations associated with individual modalities

Figure 1. Different spectrum of atrophic myopic maculopathy by colour fundus photograph: tessellated fundus (A), diffuse chorioretinal atrophy (B), patchy chorioretinal atrophy (C), and macular atrophy (D). White arrows in (C) denote the areas of focal atrophy and correspond to reduced signal on fundus autofluorescence (C’) and loss of outer retina, retinal pigment epithelium and choriocapillaris on optical coherence tomography (C”).
Given the plethora of clinical signs and the insidious nature of pathologic myopia, it can be difficult to recognise when referral to an ophthalmologist is indicated. Furthermore, the myopic eye is also notoriously difficult to examine, which introduces yet another challenge for identifying suitable candidates for ocular imaging.
STEP ONE: APPLY A TRICHOTOMOUS APPROACH TO DIAGNOSIS
The definition and terminologies used to describe myopic maculopathy have been heterogeneous in the literature and historically centred on atrophic changes.3-5
We recommend a trichotomous approach by classifying myopic maculopathy into one of three categories, as recently proposed by Ruiz-Medrano et al:6
1) Atrophy
2) Traction
3) Neovascularisation
The trichotomous approach serves as a reminder, to clinicians, of the different mechanisms underlying abnormalities such as degeneration, mechanical traction and neovascularisation, and the need for separate management plans. The categories are not mutually exclusive and different subcategories of maculopathy can co-exist in the same eye.
STEP 2: STAGE MYOPIC MACULOPATHY USING MULTIMODAL IMAGING
Atrophic myopic maculopathy (AMM) describes progressive atrophic changes at the macula associated with myopia. Using colour fundus photography (CFP), it can be categorised into the following: no myopic retinal lesions, tessellated fundus, diffuse chorioretinal atrophy, patchy chorioretinal atrophy and macular atrophy.5
The tessellated fundus appearance refers to increased visibility of the underlying choroidal vessels around the fovea and vascular arcades (Figure 1A). Diffuse chorioretinal atrophy (CRA) presents as a yellowish-white appearance to the posterior pole (Figure 1B). The extent of atrophy may vary from a restricted area around the optic disc and macula to the entire posterior pole.7 Patchy CRA are welldefined, greyish-white lesions in the macula or around the optic disc (Figure 1C).

Figure 2. OCT showing the spectrum of tractional myopic maculopathy: (A) myopic foveoschisis involving the outer plexiform layer, showing a thick inner layer and thin outer layer; (B) myopic foveoschisis involving inner retinal schisis (arrow) and outer retinal schisis (asterisk); (C) shallow neurosensory detachment
involving the fovea (star); (D) full-thickness macular hole. The most severe stage of tractional myopic maculopathy – macular hole with retinal detachment – is not presented here.
The clinical presentation of patchy CRA varies, depending on the origin and typically appears round within diffuse CRA, ovoid in association with lacquer cracks in the perifovea, or arcuate at the edge of posterior staphyloma.8 Macular atrophy describes a similarly well-defined, round chorioretinal atrophic lesion present in the foveal region (Figure 1D). It may stem from the coalescence of patchy CRA or regression of myopic choroidal neovascularisation (CNV).
Myopic traction maculopathy (MTM), also known as myopic retinoschisis or myopic foveoschisis, describes the splitting of the neurosensory retina in eyes with pathologic myopia diagnosed using optical coherence tomography (OCT). The splitting can occur at the outer retina (Figure 2A), inner retina, or involve both layers (Figure 2B). The split can also involve the fovea or non-foveal area. Associated tractional disorders, such as foveal detachment (Figure 2C), full-thickness macular hole (FTMH) (Figure 2D), and macular hole with retinal detachment, are also included under this umbrella term.
Neovascular myopic maculopathy (NMM) describes the retinal abnormalities predisposing to, or secondary to neovascularisation, and consists of three signs that chronicle the event of CNV – lacquer cracks (LCs), active CNV, and Fuchs’ spot. LCs are mechanical breaks of the retinal pigment epithelium (RPE), Bruch’s membrane, and the choriocapillaris complex.9 On CFP, LCs appear as yellowish linear lesions in the macula (Figure 3A) and are often found to criss-cross the underlying choroidal vessels.5 OCT examination shows discontinuation of the RPE, increased signal transmission into the deeper tissues (Figure 3B) and in some cases, perforating scleral vessels beneath them.10
Through the LCs, newly formed blood vessels from the choroid can develop and extend into the subretinal space, forming a type 2 or classic CNV.11 Funduscopically, it shows as a greyish area with hyperpigmented borders, occasionally accompanied by retinal bleeding and exudates (Figure 3C). On OCT, it appears as a highly reflective dome-shaped projection above the RPE (Figure 3D).12 Subfoveal location is more common than juxtafoveal and extrafoveal locations.12
When the CNV regresses, a pigmented scar, known as Fuchs’ spot, forms (Figure 3E). On OCT, the regressed CNV is flattened, and better-defined with underlying tissue attenuation (Figure 3F). Finally, atrophy develops around the Fuchs’ spot, overlapping with the patchy CRA or macular atrophy stage of AMM.
STEP 3: OVERCOME THE CHALLENGES OF ASSESSING THE MYOPIC EYE
Highly myopic eyes are notoriously challenging to image: defocus, mirror artefacts, image truncation, and segmentation errors are rife due to the long axial length, posterior staphyloma, the presence of the large CRA and other confounding factors. Even though acquiring images free from any spurious artefacts may be unrealistic, some simple strategies can be effective in improving image quality and boosting the diagnostic utility of ocular imaging. Firstly, a fully dilated pupil and optimised tear film are imperative, and even more so when the patient has miotic pupils and media opacity. Secondly, when the patient’s refractive error exceeds the instrument’s focus range, e.g., with CFP, fitting the eyes with corrective contact lenses before capturing the image likely lessens the defocus induced blur. The third strategy calls for clinicians to be flexible with testing strategies and scanning patterns. If the quality of the OCT scan is deficient using the standard macular cube or line scan, mitigate it by scanning on a different angle (e.g. using a vertical cube scan), applying a radial scan and/or shortening the scan length. Certain OCTs also have axial length parameters on the test menu to allow optimisation of the axial alignment between the patient’s eye and the objective lens. Clinicians should be acquainted with their armamentarium to leverage their testing capacities.
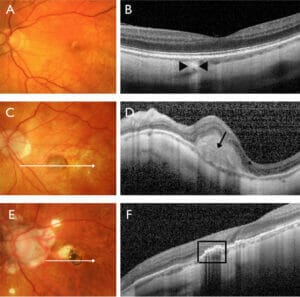
Figure 3. Stages of neovascular myopic maculopathy. Macular lacquer cracks predispose to the development of choroidal neovascularisation (CNV) and appear as yellow-white lines on CFP (A) and increased choroidal transmission (arrowheads) on OCT (B). Active CNV appears as a grey neovascular network accompanied by a subretinal haemorrhage (C) and corresponds to the hyper-reflective, dome-shaped elevation above the RPE (arrow) on OCT (D). Fuchs’ spot represents the scar formation secondary to CNV and appears as a round dark pigmented lesion adjacent to patchy chorioretinal atrophy (E) and corresponds to the flattened, well-defined lesion above the RPE (box) on OCT (F).
Despite the challenges, applying multimodal imaging on myopic eyes is paramount due to the inherent limitations associated with individual modalities. OCT enables detailed evaluation of the depth-resolved retinal layer architecture and precise detection of subtle exudative signs. It is the gold standard for imaging MTM, an indispensable tool for diagnosing NMM, and an adjunct tool for diagnosing AMM (Figure 1C”).
However, OCT is not as sensitive as CFP in detecting lacquer cracks10 and can miss small subretinal haemorrhages. Fundus autofluorescence (FAF) is a sensitive technique for diagnosing patchy CRA (Figure 1C’) and macular atrophy, although it does not differentiate other causes of atrophy from pathologic myopia. OCT angiography (OCTA) is an emerging non-invasive technique for detecting myopic CNV and assessing its activity.13,14 However, its diagnostic capacity remains limited due to the aforementioned challenges in imaging myopic eyes. Additionally, the instrument is not readily available in a standard optometric practice. Taken together, clinicians should fully use the ophthalmic imaging devices at their disposal but weigh in the results from the different modalities to achieve a more comprehensive assessment and accurate staging of myopic maculopathy.
STEP 4: RECOGNISE THE SIGNS THAT WARRANT OPHTHALMOLOGICAL REFERRAL
There is a wide spectrum of presentation of myopic maculopathy, representing the various levels of risk of vision loss. Primary eye care practitioners should be proficient in recognising red flag signs and referring to a retinal ophthalmologist for further assessment and management at an appropriate timeframe (Figure 4).
First and foremost, patients with active myopic CNV, or high suspicion of CNV, should be referred promptly (within one week) for investigation and treatment.
Symptoms, visual acuity, fundoscopy and OCT (supplemented by OCTA if available) are vital examinations to detect CNV. The patient may complain of reduced vision and/or metamorphosis. Fundoscopic signs may reveal a greyish area with hyperpigmented borders, with or without retinal bleeding and exudates. A high degree of suspicion ought to be raised if there is a hyperreflective dome-shaped projection above the RPE on OCT, corresponding with the fundus lesion. Associated exudative signs, such as subretinal and/or intraretinal fluid, further validate the CNV activity. However, as myopic CNV is less exudative than its age-related macular degeneration counterpart, the lack of exudative signs does not conclusively exclude CNV. Surrogate signs of active CNV include fuzzy borders of the dome-shaped projection and focal loss of the external limiting membrane.15,16 OCTA can be complementary to OCT and may display the CNV as an increased flow signal, shaped like a sea-fan with vascular branching and anastomosis/ loops on the avascular or outer retinachoriocapillaris slab.14
An important differential of myopic CNV is a simple macular haemorrhage, caused by the formation of a new LC in the absence of CNV. A simple haemorrhage tends to initially occur in younger patients with LCs17 and resolves spontaneously with good prognosis. However, differentiating a simple haemorrhage from CNV is not always straightforward on OCT and, given the devastating consequence of CNV without timely treatment and its tight therapeutic window, myopic patients with macular haemorrhages should be assumed to have CNV until proven otherwise. Fluorescein angiography used in combination with OCT, has higher sensitivity than individual techniques alone when diagnosing myopic CNV and differentiating it from a simple haemorrhage.17 Once CNV is confirmed, treatment typically begins immediately, if possible, or within one week.12 The first line of treatment is intravitreal anti-vascular endothelial growth factor injection, the efficacy and safety of which have been evaluated in several large prospective randomised clinical trials.12

Figure 4. Recommended management flowchart for myopic maculopathy. Primary eye care practitioners are recommended to diagnose, classify, and stage the myopic maculopathy using multimodal imaging, or refer if imaging
is unavailable. Selected signs that warrant referral to retinal ophthalmologists and the criteria for low vision service referral are also listed. *Adapted from Vision2020 adult referral pathway for blindness and low vision services.
Certain signs, such as patchy CRA, macular atrophy, and LCs,18 carry a higher risk of progression to CNV and may also need to be referred when in doubt or when multimodal imaging is not accessible.
Furthermore, MTM, if associated with progressive vision loss, may benefit from surgical interventions. Clinicians should heed the status of the fovea when evaluating the MTM, using the OCT radial scan. MTM with foveal detachment and/or FTMH should be referred within one month. If there is concurrent retinal detachment associated with the FTMH, an urgent referral within the same day is recommended. Treatment for MTM includes pars plana vitrectomy and/ or scleral buckling, and targets both anatomical (foveal reattachment) and functional (visual acuity) improvement while minimising the complications.19
STEP 5: PROVIDE APPROPRIATE OPTOMETRIC MANAGEMENT AND FOLLOW-UP
Equipped with advanced ocular imaging and in-depth disease knowledge, primary eye care practitioners are suitably positioned to monitor sizable manifestations of myopic maculopathy that do not require immediate onward referral. The frequency of review should be tailored based on the progression pattern, the risk of vision loss, and individual risk factors.
In AMM, patchy atrophy presents a higher risk of progression to macular atrophy and CNV than tessellated fundus and diffuse atrophy,8 and would require a shorter review window (six to 12 months) than the latter two (12 to 24 months). OCT and FAF are useful adjunct tools to monitor the progression in addition to CFP.
Milder presentations of MTM (no foveal detachment or FTMH) are generally slowly progressive20 and may be monitored every six to 12 months using the OCT macula cube and radial line scans. Clinicians should consider referral if there is a progressive decline in visual acuity in the context of anatomical worsening on OCT.
Patients with treated and resolved NMM, discharged from ophthalmological review, still require ongoing observation with fundoscopy and OCT. This is because 35% of patients with myopic CNV develop bilateral disease in the fellow eye within eight years.18
The individual risk factors for progression and vision loss may include older age, worse severity at baseline, posterior staphyloma and increased axial length.8,21 Those factors should be taken into account when determining the review period and threshold for referral, in combination with considerations such as the patient’s preference, visual demand and access to eye care.
Besides regular ocular health reviews, clinicians should optimally manage the patient’s refractive error, educate them on the signs, symptoms, and risks of CNV and macular atrophy, recommend Amsler grid self-monitoring in appropriate cases, and manage expectations as vision deteriorates with degeneration even with treatment.
The detrimental effect of myopic maculopathy on central vision may threaten a patient’s independence by challenging daily activities such as reading and driving. A conversation on low vision services should be initiated with the patient when the binocular visual acuity is less than 6/12 and/or there is reduced capacity to undertake activities of daily living. These criteria are endorsed in the Vision 2020 Australia low vision referral pathway guideline (www.vision2020australia.org. au/resources/adult-referral-pathway) and reflect the pivoted direction toward earlier interventions. It is important to know that low vision services go beyond magnifiers, encompassing multidisciplinary services such as occupational therapy to assist independent living, orientation and mobility, assistive technology to support access to information, peer support and social programs, and mental health support. Clinicians should ask questions about daily living on routine examination, make suitable recommendations on support and services, and empower the patient to make an informed decision. A list of service delivery organisations and how to refer to them can be found on the Vision 2020 website.
SUMMARY
Myopic maculopathy has a myriad of manifestations that are broadly categorised into three components: atrophic, tractional and neovascular. Using multimodal imaging modalities, primary eye care practitioners can accurately diagnose and stage the different components and effectively triage presentations that mandate timely referral to, and treatment by, a retinal ophthalmologist. Proactive referral to low vision services forms an integral part of managing not only the patient’s vision, but also the reduced independence associated with vision loss. Powered by a standardised systematic approach and rich practical insights, we hope this article will contribute to the overarching goal of reducing the incidence and impact of vision loss from pathologic myopia, and enhancing care for patients.
Pauline Xu BOptom (Hons), MOptom, GradCertOcTher is a Centre for Eye Health lead clinician (retinal dystrophies). She has experience in a variety of clinical settings, including rural and urban private practice, and she spent five years as a research optometrist with the Brien Holden Vision Institute before joining the Centre. While working at the Centre, she developed strong interests in advanced ocular imaging, macular diseases and retinal dystrophies.
Dr Angelica Ly BOptom (Hons), GradCertOcTher, PhD, FAAO is the lead clinician (macula) at the Centre for Eye Health. With a passion for evidence based optometry, ocular disease and clinical research, she has presented at global conferences and has been widely published.
References
- Flitcroft DI, He M, Jonas JB et al. IMI – Defining and Classifying Myopia: A Proposed Set of Standards for Clinical and Epidemiologic Studies. Invest Ophthalmol Vis Sci 2019; 60: M20-M30.
- Holden BA, Fricke TR, Wilson DA et al. Global Prevalence of Myopia and High Myopia and Temporal Trends from 2000 through 2050. Ophthalmology 2016; 123: 1036- 1042.
- Liu HH, Xu L, Wang YX et al. Prevalence and Progression of Myopic Retinopathy in Chinese Adults: The Beijing Eye Study. Ophthalmology 2010; 117: 1763-1768.
- Asakuma T, Yasuda M, Ninomiya T et al. Prevalence and Risk Factors for Myopic Retinopathy in a Japanese Population: The Hisayama Study. Ophthalmology 2012; 119: 1760-1765.
- Ohno-Matsui K, Kawasaki R, Jonas JB et al. International photographic classification and grading system for myopic maculopathy. Am J Ophthalmol 2015; 159: 877-883 e877.
- Ruiz-Medrano J, Montero JA, Flores-Moreno I et al. Myopic maculopathy: Current status and proposal for a new classification and grading system (ATN). Prog Retin Eye Res 2019; 69: 80-115.
- Ohno-Matsui K, Lai TY, Lai CC et al. Updates of pathologic myopia. Prog Retin Eye Res 2016; 52: 156-187.
- Hayashi K, Ohno-Matsui K, Shimada N et al. Long-term pattern of progression of myopic maculopathy: a natural history study. Ophthalmology 2010; 117: 1595-1611, 1611 e1591-1594.
- Klein RM, Curtin BJ. Lacquer crack lesions in pathologic myopia. Am J Ophthalmol 1975; 79: 386-392.
- Xu X, Fang Y, Uramoto K et al. Clinical Features of Lacquer Cracks in Eyes with Pathologic Myopia. Retina 2019; 39: 1265-1277.
- Freund KB, Zweifel SA, Engelbert M. Do we need a new classification for choroidal neovascularization in age-related macular degeneration? Retina 2010; 30: 1333-1349.
- Cheung CMG, Arnold JJ, Holz FG et al. Myopic Choroidal Neovascularization: Review, Guidance, and Consensus Statement on Management. Ophthalmology 2017; 124: 1690-1711.
- Querques L, Giuffre C, Corvi F et al. Optical coherence tomography angiography of myopic choroidal neovascularisation. Br J Ophthalmol 2017; 101: 609-615.
- Li S, Sun L, Zhao X et al. Assessing the activity of myopic choroidal neovascularization: Comparison Between Optical Coherence Tomography Angiography and Dye Angiography. Retina 2020; 40: 1757-1764.
- Introini U, Casalino G, Querques G et al. Spectraldomain OCT in anti-VEGF treatment of myopic choroidal neovascularization. Eye (Lond) 2012; 26: 976-982.
- Battaglia Parodi M, Iacono P, Bandello F. Correspondence of Leakage on Fluorescein Angiography and Optical Coherence Tomography Parameters in Diagnosis and Monitoring of Myopic Choroidal Neovascularization Treated with Bevacizumab. Retina 2016; 36: 104-109.
- Ren P, Lu L, Tang X et al. Clinical features of simple hemorrhage and myopic choroidal neovascularization associated with lacquer cracks in pathologic myopia. Graefe’s Archive for Clinical and Experimental Ophthalmology 2020; 258: 2661-2669.
- Ohno-Matsui K, Yoshida T, Futagami S et al. Patchy atrophy and lacquer cracks predispose to the development of choroidal neovascularisation in pathological myopia. Br J Ophthalmol 2003; 87: 570-573.
- Gohil R, Sivaprasad S, Han LT et al. Myopic foveoschisis: a clinical review. Eye (Lond) 2015; 29: 593-601.
- Shimada N, Tanaka Y, Tokoro T et al. Natural course of myopic traction maculopathy and factors associated with progression or resolution. Am J Ophthalmol 2013; 156: 948-957 e941.
- Fang Y, Yokoi T, Nagaoka N et al. Progression of Myopic Maculopathy during 18-Year Follow-up. Ophthalmology 2018; 125: 863-877.





