While using advanced imaging to evaluate diseases affecting the central retina is established in primary eye care, the advantages for assessing peripheral lesions are less often cited. This presents a missed opportunity as peripheral retinal degenerations occur in up to 31% of individuals and may be associated with serious complications such as retinal breaks, tears and detachments.1
In this article, we present new evidence on the unique imaging features and significance of peripheral degenerations in the retina, which have been developed into a handy chairside guide to aid clinical decision making.

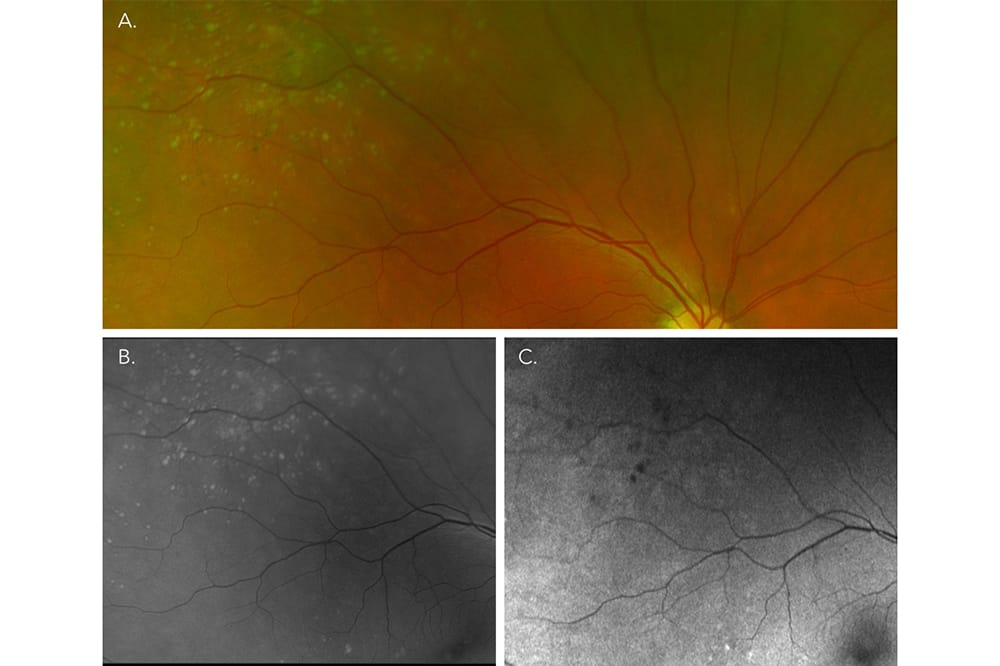
Figure 1. Peripheral drusen.
For many optometrists, a thorough, peripheral retinal exam can be difficult to perform within the time constraints of a routine consultation. The difficulties in assessing the periphery can be further compounded when dilation is refused due to patient aversion to the cycloplegic and photophobic effects induced or a need to drive immediately afterwards. Yet identifying peripheral anomalies is an important part of routine eye care and, in particular, distinguishing between lesions that are benign versus those associated with potentially serious sequelae such as retinal breaks, or detachments. Emerging evidence showing associations between peripheral degenerations and ocular and systemic disorders is also transforming previous perceptions that the significance of these retinal lesions is isolated to the retina.
THE PROMISE OF ADVANCED IMAGING
Technologies, including ultrawidefield (UWF) and widefield optical coherence tomography (OCT) imaging, have vastly improved our ability to image the periphery. For example, images from the UWF scanning laser ophthalmoscope (Optomap) provide extensive views of up to 200º or 82.5% of the total retina and can be used to optimise the view of the inner retina/ retinal vasculature, and of deeper retinal and choroidal structures via green and red channel settings, respectively. The technology is also capable of imaging in other modalities, including fundus autofluorescence (FAF), indocyanine green and fluorescein angiography.2 Additionally, 55º of eccentric capture can be reached using wide-field OCT on commercial devices.3 With up to 41% of optometrists having these imaging devices available in their practice,4 enhancing our visualisation of peripheral retinal degenerations using advanced retinal imaging in a routine eye examination is eminently achievable for many.

Figure 2. Reticular pigmentary degeneration.
What is lacking, however, is easily accessible evidence on how such lesions are visualised using these devices to facilitate their use in clinical practice. Researchers at the Centre for Eye Health and School of Optometry at UNSW identified this and recently published a review article detailing the advanced ocular imaging features and clinical significance of numerous retinal degenerations that are commonly encountered in the periphery.5 In this article, we highlight key case study examples provided in the review and offer a chairside guide for clinical practice.
ADVANCED IMAGING OF BENIGN PERIPHERAL RETINAL DEGENERATIONS
A number of peripheral retinal degenerations do not involve the vitreous and are considered benign without associated visual complications. Thus, one might suggest that advanced imaging of these lesions is inconsequential. Emerging evidence however, suggests that some of these entities, such as peripheral drusen and reticular pigmentary degeneration, are linked to ocular and systemic disorders such as age-related macular degeneration (AMD), Alzheimer’s and chronic kidney disease. Therefore, as the knowledgebase around this expands, enhanced visualisation may become an integral part of holistic care, providing information that helps to manage the overall health of the patient. The following section describes visualisation of benign peripheral retinal degenerations using UWF and widefield OCT and the benefit to clinical practice.

Figure 3. Horsehoe tear.
Peripheral Drusen
Peripheral drusen appear similar to macular drusen but are more reflective on multimodal imaging (Figure 1). UWF imaging is useful for highlighting and capturing the extent and distribution of peripheral drusen. Their characteristics on FAF and OCT mirror that of macular drusen in that both may show increased or decreased intensity and display similar morphology features, respectively.5,6 Recent studies have also reported a significant association between peripheral drusen and AMD severity,7 and a higher prevalence in AMD, Alzheimer’s8 and chronic kidney disease populations.9 These findings suggests that the lesions may be linked to complement pathway dysfunction, and thus their presence could have future implications in managing AMD.
Reticular Pigmentary Degeneration
Reticular pigmentary degeneration is also known as ‘honeycomb’ chorioretinal degeneration due its net-like appearance of hyperpigmentary lines (Figure 2). Their overall pattern of distribution and density is easily visualised on UWF imaging, which assists in differentiating reticular degeneration from areas of chorioretinal scarring related to previous trauma or surgery. They are best observed on red-free, FAF and infrared imaging, and present as retinal pigment epithelium disruptions on OCT.5 Associations with increased AMD grade,7 severity,10 and scotopic visual function deficits in AMD11 suggest that the lesions may play a role in AMD. The appearance and location of this degeneration also closely resembles the bone spicules of retinitis pigmentosa, highlighting the importance of imaging for differential diagnosis.
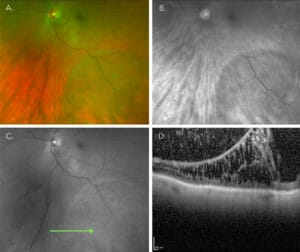
Figure 4. Bullous retinoschisis.
Other Benign Lesions
For degenerations without systemic associations, including white or dark without pressure, microcystoid and pavingstone degeneration, understanding their specific clinical and imaging features is important to distinguish them from other clinically significant peripheral anomalies of similar appearance, such as chorioretinal laser scars or commotio retinae. Further information on the clinical and imaging properties of lesions can be obtained by accessing our review paper.5
PERIPHERAL RETINAL DEGENERATIONS PREDISPOSING TO RETINAL BREAKS
Other peripheral degenerations including lattice, acquired retinoschisis, retinal holes and vitreoretinal tufts, have been associated with retinal breaks and detachment as a result of vitreoretinal interactions. Thus, enhanced visualisation of these entities is essential to appropriate clinical management and documentation to identify signs of progression. The following section provides unique descriptions of their clinical features and advanced imaging characteristics.
Retinal Holes

Figure 5. Retinal hole in lattice degeneration.
Retinal holes are full thickness retinal breaks, which may be round or horseshoeshaped and sometimes present with a fluid cuff (Figure 3). Degenerative processes that may be associated with holes, including retinoschisis and vitreoretinal tufts, are easily visualised on OCT imaging in conjunction with stereoscopic fundus assessment.12 Although atrophic holes generally have not been linked to clinical retinal detachment, 5–10% of patients experiencing symptoms,13 or presenting with lattice-associated holes,14 may experience progression to detachment. Hence, documenting their appearance with sequential UWF imaging is useful for clinical management of these lesions.
Acquired Retinoschisis
Acquired retinoschisis appear as elevated retinal areas that may be shallow (typical) or bullous (reticular) in shape (Figure 4). Their peripheral extent and shape are distinguished more easily on UWF imaging, and clearly differentiated from retinal detachment when evaluated using peripheral OCT. Research shows that the risk of retinal breaks or progression to detachment from retinoschisis is only 0.85/million.15
Lattice Degeneration
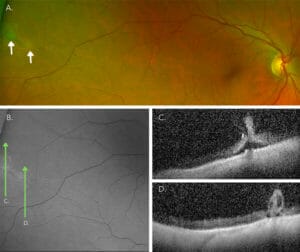
Figure 6. Vitreoretinal tufts.
Lattice degeneration appears as elongated, white lesions that run parallel to the ora serrata in the far periphery (Figure 5).16 They are easily visualised on red and green-free imaging, while alterations at the vitreoretinal interface, inner and full thickness retina changes are visible on peripheral OCT imaging. Although atrophic holes present in 18–45% of lattice degeneration,17,18 they rarely progress to retinal detachment (~1%) and when they do occur, tend to be slowly progressive.19 The risk is slightly greater in phakic eyes, with bilateral lattice that have a history of retinal detachment in the fellow eye (1–5%),20 and high myopes (4.4%).21
Vitreoretinal Tufts
Vitreoretinal tufts appear as round, well demarcated retinal elevations that display overall hyperreflectivity when they are non-cystic, and a hyperreflective apex with a hyporeflective core in cystic lesions on OCT.22 While non-cystic lesions are not associated with retinal breaks, cystic tufts are associated with a low risk of rhegmatogenous retinal detachment (0.28%).
SUMMARY
Visualisation and characterisation of peripheral retinal lesions is enhanced using advanced imaging modalities, such as UWF imaging and widefield OCT imaging. While the association of many peripheral retinal degenerations with retinal breaks and detachment is typically low, associations with systemic and ocular diseases is still unclear and may have growing future importance in clinical assessments for these conditions.
These findings are summarised in a handy chairside guide to aid clinical decisionmaking, which can be obtained by accessing our review paper.5
Dr Lisa Nivison-Smith BSc (Hons), PhD, FAAO, is currently a National Health and Medical Research Council fellow and Senior Scientia Lecturer at the Centre for Eye Health and the School of Optometry and Vision Science at the University of New South Wales. She did her undergraduate degree in molecular biology and genetics at the University of Sydney in 2006 and then continued to a PhD in tissue engineering, making a synthetic blood vessel model for testing of therapeutics in vitro. She finished her PhD in 2011 and moved fields again, starting in the field of vision science at the University of New South Wales. She helped establish the Retinal Networks Laboratory with Michael Kalloniatis and then the research group at the Centre for Eye Health. Dr Nivison-Smith’s current research interests lie in retinal disease biology, particularly photoreceptor degenerations such as age-related macular degeneration and retinitis pigmentosa.
Rene Cheung BSc(Hons), BOptom, MOptom graduated in 2013 from University of New South Wales and completed her postgraduate studies while working full time as an optometrist in the Hunter New England region. She joined the Centre for Eye Health in 2021 to start her PhD, which explores strategies to improve retinal imaging analysis in clinical practice and understanding potential barriers to accessing the technology. Her research is supported by the Australian Government Research Training Program Scholarship and the Small Grants Funding Scheme from the Australian Human Rights Institute UNSW.
References
- Flaxel CJ, Adelman RA, Bailey ST, et al. Posterior Vitreous Detachment, Retinal Breaks, and Lattice Degeneration Preferred Practice Pattern(R). Ophthalmology. 2020;127(1):P146-P181.
- Nagiel A, Lalane RA, Sadda SR, Schwartz SD. ULTRAWIDEFIELD FUNDUS IMAGING: A Review of Clinical Applications and Future Trends. Retina. 2016;36(4):660-678.
- McNabb RP, Grewal DS, Mehta R, et al. Wide field of view swept-source optical coherence tomography for peripheral retinal disease. Br J Ophthalmol. 2016;100(10):1377-1382.
- Tang V, Symons RCA, Guest D, McKendrick AMJO, Optics P. An overview of optometrists’ diabetic retinopathy practice patterns–a cross-sectional survey. 2021;41(4):885-895.
- Cheung R, Ly A, Katalinic P, et al. Visualisation of peripheral retinal degenerations and anomalies with ocular imaging. Paper presented at: Seminars in Ophthalmology 2022.
- Suetsugu T, Kato A, Yoshida M, et al. Evaluation of peripheral fundus autofluorescence in eyes with wet age-related macular degeneration. Clin Ophthalmol. 2016;10:2497-2503.
- Seddon JM, Reynolds R, Rosner B. Peripheral retinal drusen and reticular pigment: association with CFHY402H and CFHrs1410996 genotypes in family and twin studies. Invest Ophthalmol Vis Sci. 2009;50(2):586-591.
- Ritchie CW, Peto T, Barzegar-Befroei N, et al. Peripheral Retinal Drusen as a Potential Surrogate Marker for Alzheimer’s Dementia: A Pilot Study Using Ultra-Wide Angle Imaging. Investigative Ophthalmology & Visual Science. 2011;52(14).
- Choi J, Moon JW, Shin HJ. Chronic kidney disease, early age-related macular degeneration, and peripheral retinal drusen. Ophthalmic Epidemiol. 2011;18(6):259-263.
- Lewis H, Straatsma BR, Foos RY, Lightfoot DO. Reticular degeneration of the pigment epithelium. Ophthalmology. 1985;92(11):1485-1495.
- Lains I, Park DH, Mukai R, et al. Peripheral Changes Associated With Delayed Dark Adaptation in Age-related Macular Degeneration. Am J Ophthalmol. 2018;190:113-124.
- Choudhry N, Golding J, Manry MW, Rao RC. Ultra- Widefield Steering-Based Spectral-Domain Optical Coherence Tomography Imaging of the Retinal Periphery. Ophthalmology. 2016;123(6):1368-1374.
- Davis MD. Natural history of retinal breaks without detachment. Arch Ophthalmol. 1974;92(3):183-194.
- Byer NE. Long-term natural history of lattice degeneration of the retina. Ophthalmology. 1989;96(9):1396-1401; discussion 1401-1392.
- Xue K, Muqit MMK, Ezra E, et al. Incidence, mechanism and outcomes of schisis retinal detachments revealed through a prospective population-based study. Br J Ophthalmol. 2017;101(8):1022-1026.
- Byer NE. Clinical study of lattice degeneration of the retina. Trans Am Acad Ophthalmol Otolaryngol. 1965;69(6):1065-1081.
- Guo XJCJoO. Clinical features and prognosis of retinal lattice degeneration. 1990;26(4):216-218.
- Straatsma BR, Zeegen PD, Foos RY, Feman SS, Shabo ALJAjoo. Lattice Degeneration of the Retina: XXX Edward Jackson Memorial Lecture. 1974;77(5):619-649.
- Tillery WV, Lucier AC. Round atrophic holes in lattice degeneration–an important cause of phakic retinal detachment. Trans Sect Ophthalmol Am Acad Ophthalmol Otolaryngol. 1976;81(3 Pt 1):509-518.
- Folk JC, Arrindell EL, Klugman MR. The fellow eye of patients with phakic lattice retinal detachment. Ophthalmology. 1989;96(1):72-79.
- Ho T-C, Ho A. Long-term natural course of lattice degeneration of the retina in high myopic eyes – A ten-year long term study. 2015.
- Byer NE. Cystic retinal tufts and their relationship to retinal detachment. Arch Ophthalmol. 1981;99(10):1788-1790.