


When a patient presents with painful blurry vision, closed angles and elevated intraocular pressures (IOP), the diagnosis of an acute angle closure attack is intuitive. However, acute angle closure represents only one small part of a spectrum of angle closure disease, ranging from anatomically narrow angles with normal IOPs to angle closure with manifest glaucoma.1
Mechanisms underlying narrow angles can be broken down into two categories: pupillary and non-pupillary block.2 Early detection and timely management of patients with narrow angles is key to maximising visual outcomes.3 Clinicians are often faced with challenges surrounding the diagnosis and management of angle closure spectrum disease such as:
- Does gonioscopy simply involve recording what deepest structure is visible on primary gaze?
- What is the usefulness of ancillary imaging of the anterior chamber angle and how can I apply it to these results?
- When should I refer my patient for treatment of narrow angles?
This article will provide you with an up to-date, evidence-based approach to the clinical assessment of these patients.
HOW DO I ASSESS FOR ANGLE CLOSURE?
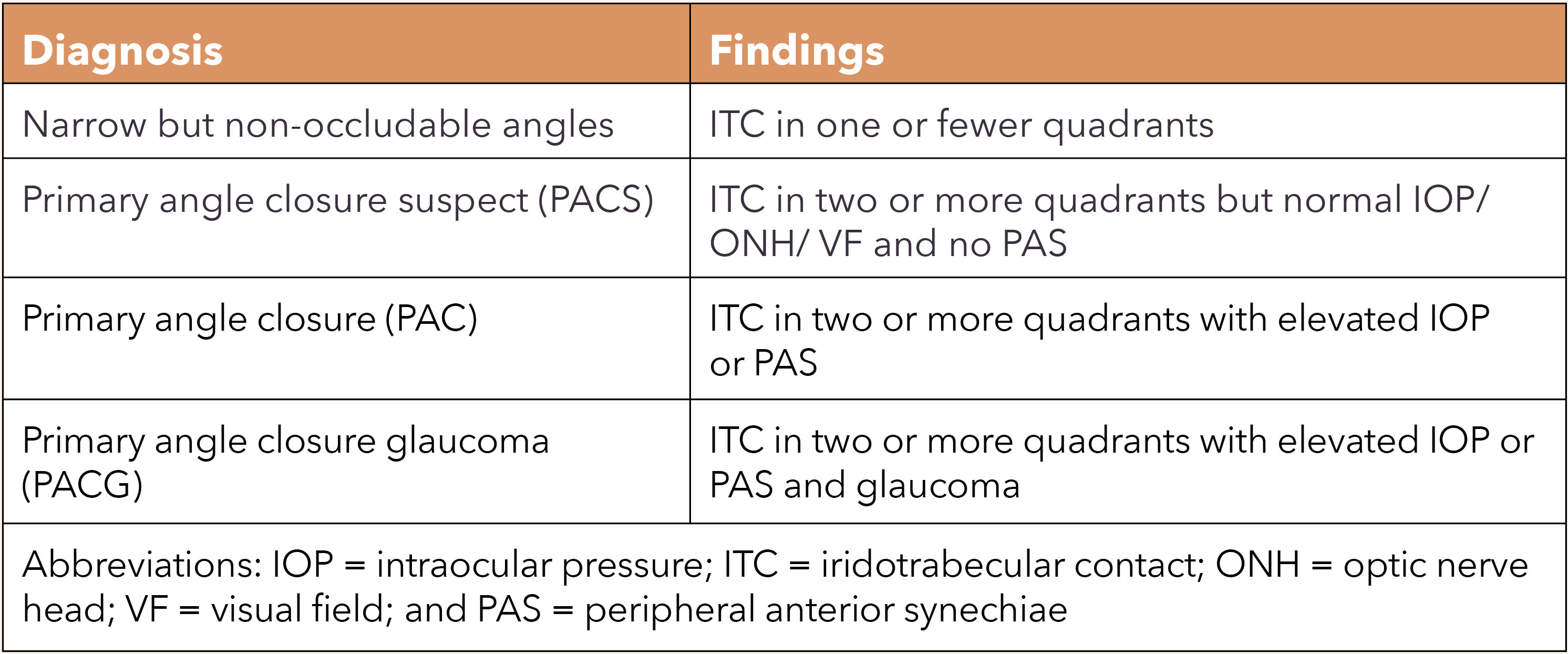
Arguably, the most important feature to identify in the assessment of narrow angles is the presence or absence of iridotrabecular contact (ITC).4 The spectrum of angle closure is defined by the extent of ITC and includes several presentations (Table 1).
Risk Factors
There are several risk factors that are associated with a higher risk of angle closure. Ocular risk factors, which affect anatomical variations in angle configuration, include shorter axial length, hyperopia, shallow anterior chamber depth, and increased thickness or anterior insertion of the iris or lens.5,6,7,8
Demographic risk factors include age, family history, female sex, and Asian or Inuit ethnicity due to the propensity for an ‘at-risk’ anterior chamber morphology, such as a thickening crystalline lens with age, or a shallow anterior chamber in females and Asian populations.9,10,11 These ocular and demographic risk factors are important to keep in mind when evaluating a patient’s risk for developing angle closure.
Work Up
In addition to assessing a patient’s risk factors, a thorough history and clinical examination is essential for determining where your patient lies on the narrow angle spectrum. A comprehensive work up should involve the following tests.
- History and Symptoms: Most patients are asymptomatic unless acute or intermittent angle closure occurs.12 Classic symptoms of acute or sub-acute closure include a blurry, red and painful eye that may be associated with headaches, nausea, vomiting, and haloes around lights, especially exacerbated during dark (scotopic) environmental conditions.12,13 Specifically, the timing and pattern of symptoms are important to elicit as there is often an association with night or early morning, or tasks such as driving at night or watching a movie in a dark cinema.14
 History-taking should also elicit for any secondary causes of angle closure including history of uveitis or scleritis, previous ocular surgery or systemic vascular disease. Systemic medications can also increase the risk of angle closure such as systemic anticholinergics or sulfa-containing drugs, with a recent study by Na and Park providing a comprehensive list.15 A classic example of drug-induced angle closure is topiramate, a drug that may be used for seizures or migraines, among other conditions.16 More commonly, patients may be self-medicating with over-the-counter topical ocular decongestants (adrenergics), which may also precipitate angle closure.17
History-taking should also elicit for any secondary causes of angle closure including history of uveitis or scleritis, previous ocular surgery or systemic vascular disease. Systemic medications can also increase the risk of angle closure such as systemic anticholinergics or sulfa-containing drugs, with a recent study by Na and Park providing a comprehensive list.15 A classic example of drug-induced angle closure is topiramate, a drug that may be used for seizures or migraines, among other conditions.16 More commonly, patients may be self-medicating with over-the-counter topical ocular decongestants (adrenergics), which may also precipitate angle closure.17
- Pupils: In acute angle closure, the affected eye may present with a fixed, mid-dilated pupil. It has also been suggested that primary angle closure (PAC) and primary angle closure glaucoma (PACG) may subtly alter pupil dynamics such as the speed of pupillary constriction.18 This occurs due to iris ischaemia and failure of the iris smooth muscle with increasing IOPs.19
- Intraocular Pressure: In angle closure, the IOP typically increases due to mechanical obstruction of the aqueous outflow, which impairs the eye’s outflow facility. An elevated IOP is one of the main differentiating features between a primary angle closure suspect (PACS) and PAC.4
- Slit Lamp Examination: Careful examination of the anterior eye is required to identify any secondary components of angle closure and signs of an acute attack, including conjunctival injection or corneal oedema.12 The Van Herick technique can be used as a non-contact estimation of the limbal anterior chamber depth to identify at-risk patients that require additional tests such as gonioscopy.20
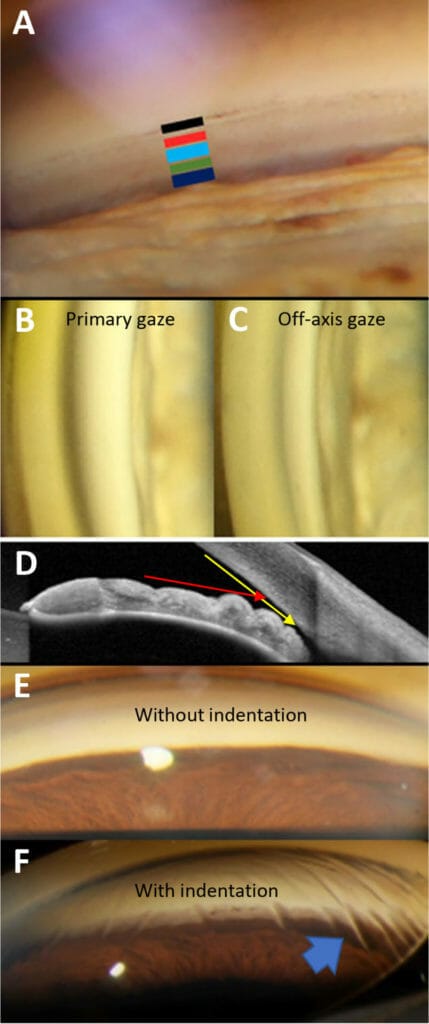
- Gonioscopy: Gonioscopy is the current gold standard for angle assessment as it offers clinicians a dynamic and in vivo method to assess for iridotrabecular contact (ITC). An example of anatomical structures seen on gonioscopy is shown in Figure 1A.
Arguably, the most important feature to identify in the assessment of narrow angles is the presence or absence of iridotrabecular contact (ITC)
In primary gaze, clinicians are able to examine pertinent features, such as visible structures, extent of pigmentation, angle width and the height and character of the iris insertion using gonioscopy.21
 For angles that appear narrow in primary gaze, off-axis gonioscopy and indentation gonioscopy are necessary to assess for ITC and the presence of peripheral anterior synechiae (PAS). Off-axis gonioscopy involves tilting the lens in the direction of the mirror (i.e. tilt upwards for the superior angle) or directing the patient’s gaze in the opposite direction (i.e. downgaze for the superior angle).22 This allows for visualisation ‘over the hill’ of the iris contour without manipulating the iridocorneal configuration to assess for ITC.
For angles that appear narrow in primary gaze, off-axis gonioscopy and indentation gonioscopy are necessary to assess for ITC and the presence of peripheral anterior synechiae (PAS). Off-axis gonioscopy involves tilting the lens in the direction of the mirror (i.e. tilt upwards for the superior angle) or directing the patient’s gaze in the opposite direction (i.e. downgaze for the superior angle).22 This allows for visualisation ‘over the hill’ of the iris contour without manipulating the iridocorneal configuration to assess for ITC.
If the trabecular meshwork cannot be visualised in both primary gaze and with lens tilt, ITC is present. An illustrative example comparing primary gaze and off-axis viewing is shown on Figure 1B-D.
On the other hand, indentation gonioscopy involves the direct application of pressure on the eye using a non-flanged gonioscopy lens until corneal stress lines are visible. If the angle remains closed despite indentation, this indicates synechial or adhesionrelated closure is present.23 An example of a gonioscopic view, with and without indentation, is shown in Figure 1E-F.
- Anterior Segment OCT (AS-OCT): Although gonioscopy is the gold standard for angle evaluation, there are a few limitations to the procedure.24 Firstly, it is skill-intensive, requiring ocular contact with topical anaesthesia. Secondly, the results can be affected by variability in illumination, unintentional pressure on the anterior chamber from the gonioscopy lens, as well as subjective interpretation.
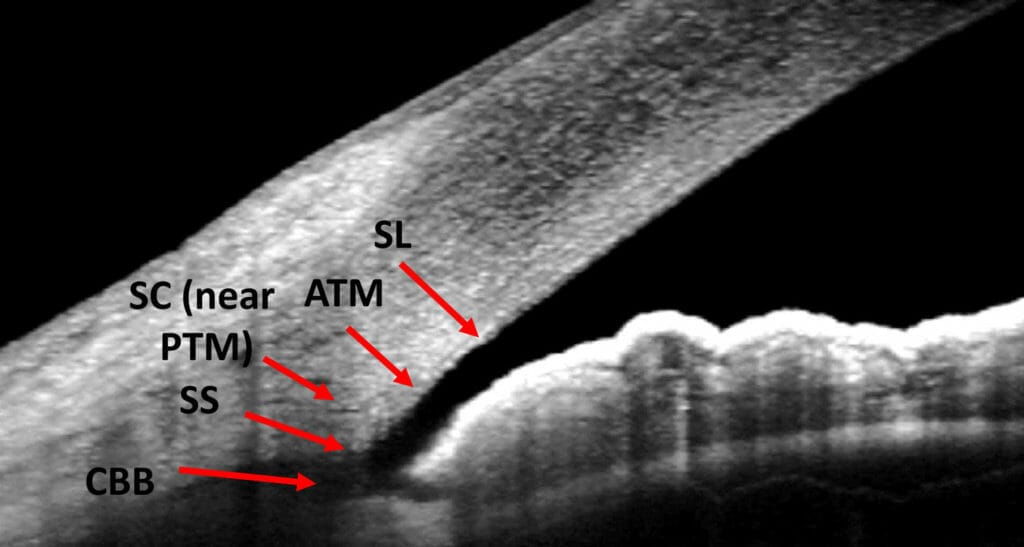
 In recent years, AS-OCT has evolved to become a quick and non-invasive technique to evaluate the anterior chamber angle.24 An illustrative example of anatomical structures on AS-OCT is shown in Figure 2. AS-OCT can be used to evaluate:
In recent years, AS-OCT has evolved to become a quick and non-invasive technique to evaluate the anterior chamber angle.24 An illustrative example of anatomical structures on AS-OCT is shown in Figure 2. AS-OCT can be used to evaluate:
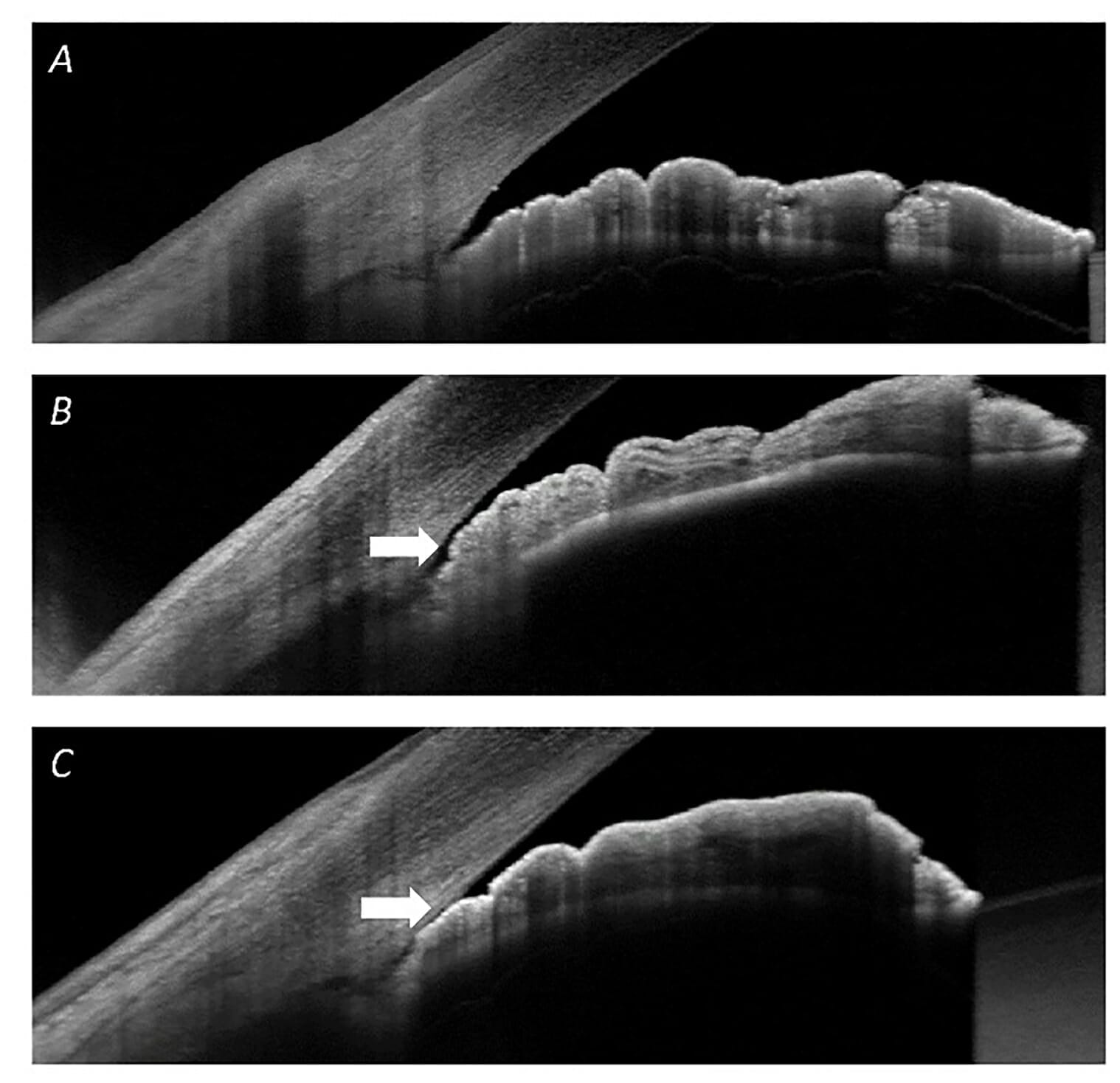
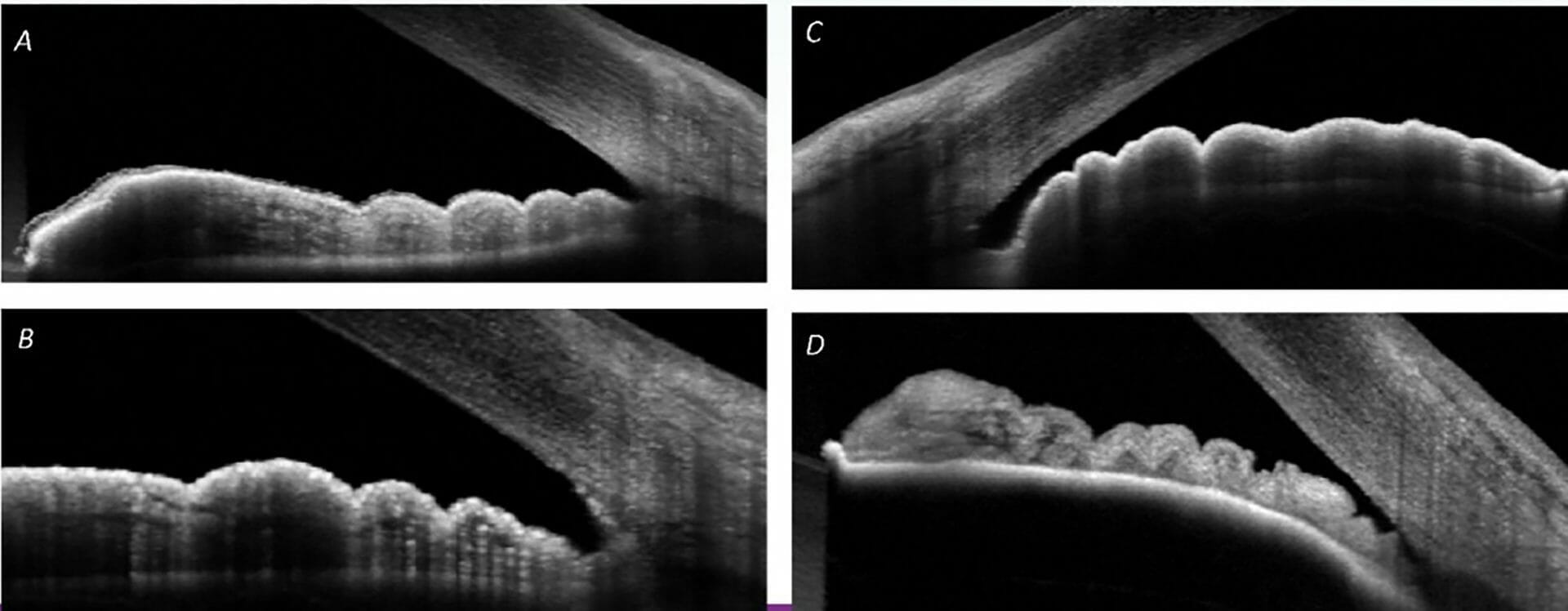
- The iris-cornea-angle relationship, specifically ITC which would indicate a closed angle (Figure 3).
- Iris profile, particularly at the insertion point (Figure 4), as well as other associated features such as lens vault, anterior chamber depth, and iris thickness.
Classic symptoms of acute or sub-acute closure include a blurry, red and painful eye that may be associated with headaches, nausea, vomiting, and haloes
While AS-OCT provides a non-invasive method for characterising the iris-lens relationship, it is not without limitations. Firstly, major angle structures, such as the scleral spur, may not always be visible25 or can be obscured by common anterior eye opacities such as corneal arcus and pterygium. Unlike gonioscopy, AS-OCT only assesses a single slice of the angle and provides limited to no information of angle pigmentation or the presence of peripheral anterior synechiae.26 Finally, while AS-OCT offers quantitative outputs such as the angle opening distance, or the trabecular-iris space area,26 no guidelines currently exist for staging narrow angle spectrum disease. Thus, while useful as an adjunct to gonioscopy, the application of AS-OCT in guiding management for these patients is limited.
WHEN SHOULD I REFER?
The longstanding consensus is that peripheral iridotomy or similar interventions for angle opening are indicated in patients diagnosed with at least PACS (defined as ITC in at least three quadrants regardless of glaucoma status).4 In the cases of PAC and PACG, the goals of treatment strategies are to reduce the risk of further disease progression in the form of ongoing glaucomatous damage.
Careful examination of the anterior eye is required to identify any secondary components of angle closure and signs of an acute attack
In PACS, however, treatment is prophylactic in nature, that is to reduce risk of onset of glaucomatous damage, and appears largely rooted in historical precedent.27,28 The National Health and Medical Research Council (NHMRC) guidelines for glaucoma29 recommend treatment in PACS patients based on risk profile, although definitions for low versus high-risk are not clear-cut. Moreover, recently the Zhongshan Angle-Closure Prevention Trial reported only two cases of spontaneous angle closure in PACS patients without intervention across five years of monitoring, translating to an annual incidence of one in 2,273 PACS patients;30 this represents a relatively low risk of acute angle closure developing in untreated PACS patients. Nonetheless, given the high visual morbidity associated with PACG, it is prudent to err on the side of caution. As such, referral for consideration of prophylactic treatment in PACS patients is reasonable until more longitudinal data on treated versus untreated outcomes are available.
In terms of patients with narrow and potentially occludable angles, monitoring appears more appropriate given the relatively low risk profile for conversion.4,27,29 While timeframes for monitoring are not clearly established in the literature, gonioscopic review every six to 12 months would be reasonable, and is practised at Centre for Eye Health (CFEH). Onward referral for treatment would be warranted should conversion to PAC or worse be observed, that is in the face of elevated IOP, progressive narrowing and/or development of peripheral anterior synechiae.4,29
Sophia Zhang is a senior staff optometrist at the Centre for Eye Health (UNSW). Her interests lie in the early detection of ocular disease, and she is currently involved in the glaucoma/ neuroophthalmology and macula unit. In addition to providing clinical services, Ms Zhang is focussed on clinical education, coordinating the undergraduate optometry placement program and professional development resources at CFEH.
Henrietta Wang is a senior staff optometrist at the Centre for Eye Health (UNSW) with clinical interests in optic nerve and retinal pathology. She received numerous clinical and academic awards during her undergraduate optometry degree, including a research scholarship for her work in the Retinal Networks Laboratory. She became a Fellow of the American Academy of Optometry in 2019 and has been regularly invited as a speaker at both national and international conferences.
Janelle Tong graduated with a Bachelor ofOptometry (Hons)/Bachelor of Science degree from UNSW, where she was awarded the University Medal. Prior to joining CFEH, she worked in a full-scope private practice in Sydney, where she developed her interest in managing posterior ocular disease. In addition to her involvement as a clinical optometrist at CFEH, Ms Tong is currently undertaking her PhD studies with a PhD titled Application of novel techniques enabling detection of early function deficits in ocular pathologies. This research will continue the work she began as a research optometrist at CFEH to develop new methods to enable the early, accurate detection of eye diseases such as glaucoma.
References
- Phu J., Wong B., Lim T., Kalloniatis M., Assessment of angle closure spectrum disease as a continuum of change using gonioscopy and anterior segment optical coherence tomography. Ophthalmic Physiol Opt. 2020;40(5):617-31.
- Sun X., Dai Y., Chen Y., et al., Primary angle closure glaucoma: What we know and what we don’t know.Progress in Retinal and Eye Research. 2017;57:26-45.
- Ang L.P., Aung T., Chua W.H., Yip L.W., Chew P.T., Visual field loss from primary angle-closure glaucoma:a comparative study of symptomatic and asymptomatic disease. Ophthalmology. 2004;111(9):1636-40.
- Thomas R., Walland M.J., Management algorithms for primary angle closure disease. Clin Exp Ophthalmol. 2013;41(3):282-92.
- Alsbirk P., Anterior chamber depth and primary angleclosure glaucoma: An epidemiologic study in Greenland Eskimos. Acta Ophthalmologica. 1975;53(1):89-104.
- Lowe R.F.. Aetiology of the anatomical basis for primary angle-closure glaucoma. Biometrical comparisons between normal eyes and eyes with primary angleclosure glaucoma. The British Journal of Ophthalmology. 1970;54(3):161.
- Friedman D.S., Gazzard G., Foster P., et al., Ultrasonographic biomicroscopy, Scheimpflug photography, and novel provocative tests in contralateral eyes of Chinese patients initially seen with acute angle closure. Archives of Ophthalmology. 2003;121(5):633-42.
- He M., Foster P., Johnson G., Khaw P., Angle-closure glaucoma in East Asian and European people. Different diseases? Eye. 2006;20(1):3-12.
- Zhang N., Wang J., Chen B., et al., Prevalence of primary angle closure glaucoma in the last 20 years: a metaanalysis and systematic review. Frontiers in Medicine. 2021;7:624179.
- Foster P.J., (Ed.) The epidemiology of primary angle closure and associated glaucomatous optic neuropathy. Seminars in ophthalmology; 2002: Taylor & Francis.
- Quigley H.A., Broman A.T., The number of people with glaucoma worldwide in 2010 and 2020. British Journal of Ophthalmology. 2006;90(3):262-7.
- Weinreb R.N., Aung T., Medeiros F.A., The pathophysiology and treatment of glaucoma: a review. JAMA. 2014;311(18):1901-11.
- Amerasinghe N., Aung T., Angle-closure: risk factors, diagnosis and treatment. Prog Brain Res. 2008;173:31-45.
- Turnbull A.M., Smith M., Ramchandani M., Angleclosure glaucoma on long-haul flights. JAMA Ophthalmol. 2014;132(12):1474-5.
- Na K.I., Park S.P., Association of Drugs With Acute Angle Closure. JAMA Ophthalmology. 2022;140(11):1055-63.
- Aminlari A., East M., Wei W., Quillen D., Topiramate induced acute angle closure glaucoma. Open Ophthalmol J. 2008;2:46-7.
- Ah-Kee E.Y., Egong E., Shafi A., et al., A review of drug-induced acute angle closure glaucoma for nonophthalmologists. Qatar Med J. 2015;2015(1):6.
- Zheng C., Cheung C.Y., Narayanaswamy A., et al., Pupil dynamics in Chinese subjects with angle closure. Graefe’s Archive for Clinical and Experimental Ophthalmology. 2012;250(9):1353-9.
- Loon S.C., Chew P.T., Oen F.T., et al., Iris ischaemic changes and visual outcome after acute primary angle closure. Clin Exp Ophthalmol. 2005;33(5):473-7.
- Dabasia P.L., Edgar D.F., Murdoch I.E., Lawrenson J.G., Noncontact Screening Methods for the Detection of Narrow Anterior Chamber Angles. Invest Ophthalmol Vis Sci. 2015;56(6):3929-35.
- Phu J., Wang H., Khuu S.K., et al. Anterior Chamber Angle Evaluation Using Gonioscopy: Consistency and Agreement between Optometrists and Ophthalmologists. Optom Vis Sci. 2019;96(10):751-60.
- Riva I., Micheletti E., Oddone F., et al., Anterior Chamber Angle Assessment Techniques: A Review. J Clin Med. 2020;9(12).
- Forbes M., Gonioscopy with corneal indentation. A method for distinguishing between appositional closure and synechial closure. Arch Ophthalmol. 1966;76(4):488-92.
- Cutolo C.A., Bonzano C., Scotto R., et al., Moving beyond the Slit-Lamp Gonioscopy: Challenges and Future Opportunities. Diagnostics (Basel). 2021;11(12).
- Narayanaswamy A., Sakata L.M., He M-G., et al., Diagnostic performance of anterior chamber angle measurements for detecting eyes with narrow angles: an anterior segment OCT study. Archives of Ophthalmology. 2010;128(10):1321-7.
- Maslin J.S., Barkana Y., Dorairaj S.K., Anterior segment imaging in glaucoma: An updated review. Indian JOphthalmol. 2015;63(8):630-40.
- Gedde S.J., Chen P.P., Muir K.W., et al., Primary Angle-Closure Disease Preferred Practice Pattern. Ophthalmology. 2021;128(1):P30-P70.
- Lowe R., Acute angle-closure glaucoma the second eye: An analysis of 200 cases. Br J Ophthalmol. 1962;46:641-50.
- National Health and Medical Research Council. NHMRC Guidelines for the screening, prognosis, diagnosis, management and prevention of glaucoma. Canberra, Australia; 2010.
- Friedman D.S., Chang D.S., Jiang Y., et al., Acute Angle- Closure Attacks Are Uncommon in Primary Angle-Closure Suspects after Pharmacologic Mydriasis: The Zhongshan Angle-Closure Prevention Trial. Ophthalmol Glaucoma. 2022;5(6):581-6.





