
A study of monozygotic twins randomised one twin to receive RLRL therapy, and the co-twin to the single vision spectacle control group.
Dr Margaret Lam chats about the potential to prescribe red light therapy for myopia management with Prof Mingguang He, global expert in vision-related clinical and epidemiologic research and Professor of Ophthalmic Epidemiology at the University of Melbourne.
Q. What is the science behind red light therapy for myopia management?
Recent evidence has demonstrated that repeated low-level red light therapy (also known as RLRL) could induce sustained choroidal thickening from treatment,1 ultimately reducing myopic progression.
Scleral hypoxia – a lack of oxygen in the sclera – has been identified as a promoter for scleral remodelling and myopia development.2 The current hypothesis is that repeated RLRL therapy may sustainably increase blood flow of the fundus, alleviating the scleral hypoxia, and therefore, contributing to myopia control.
Red light treatment is also very well tolerated, with no significant side effects observed…
Q. How much evidence is there for red light therapy now?
Studies by Jiang et al.3 and Xiong et al.4 were the first to explore the long-term efficacy and safety of continued RLRL therapy on myopia control over a two-year period. Jiang et al. carried out the first randomised trial of red light therapy and found a 65% reduction in refractive power, which increased to 87.7% in children with good (>75%) compliance.
Among those continuing RLRL for over two years, 75% reduction in both axial length and spherical equivalent refraction was observed. A modest rebound effect was observed after one year of treatment cessation. With no adverse effects recorded in either study, RLRL is considered to be a safe therapy option for myopia control.
From Chen et al.5 there is also study data for 60 children that demonstrated that RLRL was more effective for controlling axial length and myopia progression over 12 months of use compared with 0.01% atropine eye drops.
At the time of writing this article, research had commenced in preventing the incidence of myopia in pre-myopic children. JAMA Network Open had just accepted a paper describing, for the first time, a 12-month, parallel-group, school-based randomised-controlled trial conducted in Shanghai.
Results for this trial indicated up to 54.1% reduction in the incidence of myopia was achieved within 12 months among pre-myopic children.
Through the study results that are already published, RLRL therapy has proven it has merit for myopia control management, and that it is definitely an area of prescribing to keep a close eye on.
Q. There are already many myopia control options available to patients. How will these studies for RLRL affect the prescribing of orthokeratology, atropine, and myopia control spectacles?
Red light therapy is regarded as a viable alternative for managing myopia. It is non-invasive and can potentially be prescribed in very young children. In the European Union, there is regulatory approval for this therapy to be used in patients as young as three years old.
Red light treatment is also very well tolerated, with no significant side effects observed, either in clinical trials or in large real-world usage. The light source has been assessed by a United States Food and Drug Administration (FDA) certified lab under the ANSI Z80.36 standard and was found to be a ‘Group 1’ device, meaning it is safe for use. It is also the only treatment that has proven ability to reduce axial length for myopic children.
During the initial phase of implementing this technology, healthcare professionals have been advised to prioritise patients who exhibit early onset myopia, highly progressive myopia, high myopia, or those who are unresponsive or ineligible for treatment with orthokeratology or long-term atropine use.
Q. Is there merit for combining red light therapy with other therapies?
The merit of combining RLRL therapy and orthokeratology lens prescribing is presently being researched. The combination has already shown promising efficacy and safety in slowing myopia progression over one year among Chinese children aged eight to 13 years who responded poorly to orthokeratology lens wear alone.
Atropine is a contraindication for adjunctive treatment with red light therapy. To mitigate the risk of potential over-exposure to red light, we suggest stopping the use of atropine at least two weeks before initiating red light therapy.
Q. Can you provide a case study example of myopia reduction and axial length increase following treatment with RLRL?
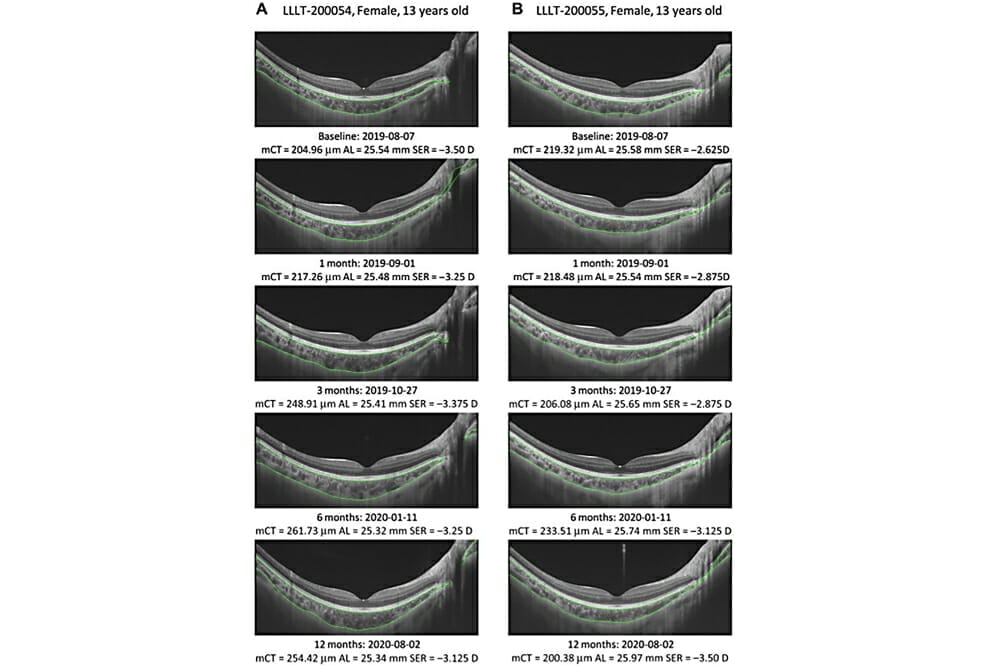
Figure 1 illustrates two interesting cases where the participants were monozygotic twins, meaning they had exactly the same genetic background. One twin was randomised to the RLRL therapy group, and the co-twin was in the single vision spectacle control group. The twin in RLRL demonstrated 0.2mm axial length shortening, reversal of myopia progression, and significant choroidal thickening. In contrast, the twin in the control group continued to exhibit myopic progression, axial length elongation, and choroidal thinning.
Figure 1. A study of monozygotic twins randomised one twin to receive RLRL therapy, and the co-twin to the single vision spectacle control group.
Q. When will RLRL be available in Australia and elsewhere?
Currently, RLRL therapy has been applied for under the Therapeutic Goods Administration (TGA) in Australia and the application is undergoing review. We expect to have TGA approval by the third quarter of 2023. In the meantime, the Special Access Scheme allows ophthalmologists and optometrists to access this treatment, based on clinical need.
In the European Union, United Kingdom, New Zealand, and Turkey, the RLRL device has already gained regulatory approval. The regulatory submission process has begun in Singapore, Malaysia, India, and the United Arab Emirates. Our sister company in China has the device registered there, and it has been accessible as a treatment for more than five years. More than 100,000 children in China are actively undergoing RLRL treatment at present.
Via a scheme similar to the Special Access Scheme in Australia, the RLRL device has already been distributed and prescribed in countries in the European Union, United Kingdom, New Zealand, and Japan. There are plans to make the device available in the Australian market as soon as TGA approval is obtained.
Q. What else is happening to further our knowledge about the use of RLRL for myopia control?
Table 1 lists innovative myopia control research projects that are ongoing and/or due to commence in various countries including China, Japan, Australia, and the United States of America.

Table 1. Ongoing work and work about to start around the world.
 Dr Margaret Lam is the National President of Optometry Australia and a Director of Optometry NSW/ACT. She practises optometry at 1001 Optical in Bondi Junction, Sydney and teaches at the School of Optometry at UNSW as an Adjunct Senior Lecturer.
Dr Margaret Lam is the National President of Optometry Australia and a Director of Optometry NSW/ACT. She practises optometry at 1001 Optical in Bondi Junction, Sydney and teaches at the School of Optometry at UNSW as an Adjunct Senior Lecturer.
 Professor Mingguang He is the Professor of Ophthalmic Epidemiology at the University of Melbourne. He undertook his medical training in China and holds a Master of Public Health degree from Johns Hopkins University in Baltimore, and PhD in ophthalmology at Moorfields Eye Hospital in London.
Professor Mingguang He is the Professor of Ophthalmic Epidemiology at the University of Melbourne. He undertook his medical training in China and holds a Master of Public Health degree from Johns Hopkins University in Baltimore, and PhD in ophthalmology at Moorfields Eye Hospital in London.
A global expert in vision-related clinical and epidemiologic research, his publications have attracted more than 13,000 citations. He has received more than $10 million in major research grants in Australia, including the prestigious National Health and Medical Rearch Council Investigator Grant and Medical Research Future Fund for his research on artificial intelligence.
References
1. Xiong R., Zhu Z., Jiang Y., et al., 2023. Longitudinal changes and predictive value of choroidal thickness for myopia control after repeated low-level red-light therapy. Ophthalmology, 130(3), 286–296.
2. Wu H., Chen W., Zhao F., et al., Scleral hypoxia is a target for myopia control. Proc Natl Acad Sci U S A 2018; 115(30):E7091–E100.
3. Jiang Y., Zhu Z., Tan X., Morgan IG., He M., et al., Effect of repeated low-level red-light therapy for myopia control in children: a multicenter randomized controlled trial. Ophthalmology. 022;129(5):509–19.
4. Xiong R., Zhu Z., Jiang Y., et al., Sustained and rebound effect of repeated low-level red-light therapy on myopia control: A 2-year post-trial follow-up study. Clinical & Experimental Ophthalmology. 2022;50(9):1013–24.
5. Chen., Yanxian., Xiong R., et al., Efficacy comparison of repeated low-level red light and low-dose atropine for myopia control: a randomized controlled trial. Translational Vision Science & Technology 2022: 33-33.





