

When a new patient presented with optic nerve head drusen and rapidly progressing visual field loss, optometrist Jessica Chi had to decide on a course of action. She decided to wait and see.
Nigel,* a 44-year-old male, presented for the first time. He is a myopic astigmatic, which he manages with spectacles. His spectacles, which were over six years old, were obtained at his last eye examination. Nigel reported the need to take off his spectacles more often for reading than before and felt his night vision may have worsened.
As there is such variability in the disease course, patients should be monitored on a regular basis, including changes on fundus examination, OCT, and visual fields
Vision with his spectacle prescription of R -3.50/-0.50×145, L -1.50/-0.50×43 was: R and L 6/6.
Subjective refraction revealed a decrease in his myopia and emerging presbyopia: R -3.25/-0.50×145 (6/6), L -1.25/-0.50×45 (6/6), near add +0.75DS.
Spectacle lens options were discussed; Nigel found the decrease in his myopic prescription for near helpful and was happy to continue taking his spectacles off for reading.
Anterior eye examination revealed no abnormalities. Fundus examination revealed granular, yellowish, calcified deposits in the optic nerve head, which were diagnosed as drusen in both eyes (Figures 1 and 2).
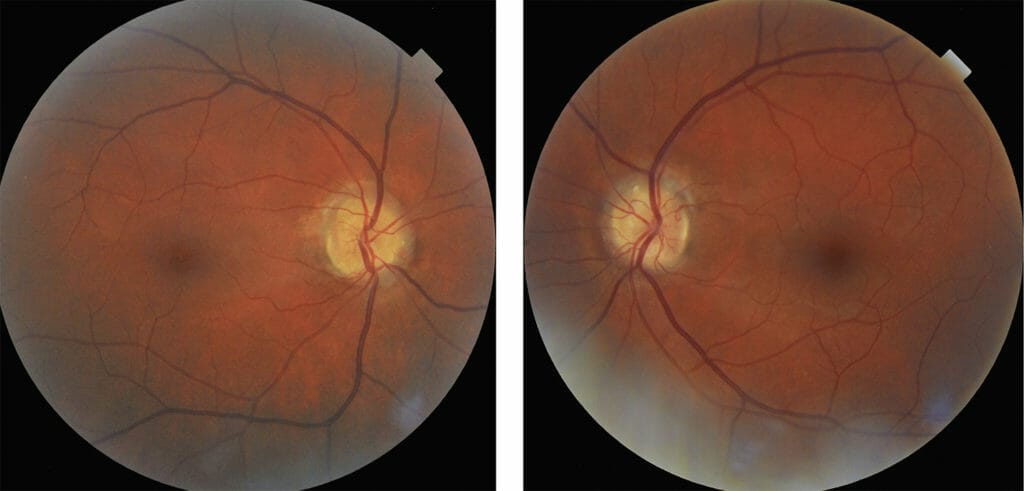
Figures 1 and 2. Drusen in both eyes revealed with fundus examination.
Optical coherence tomography (OCT) of the discs confirmed the presence of optic nerve head drusen – which appeared as hyperreflective lumpy bodies within the optic nerve head, with shadowing artefacts immediately beneath the drusen (Figure 3). There was also significant retinal nerve fibre layer drop out at the macula (Figure 4).
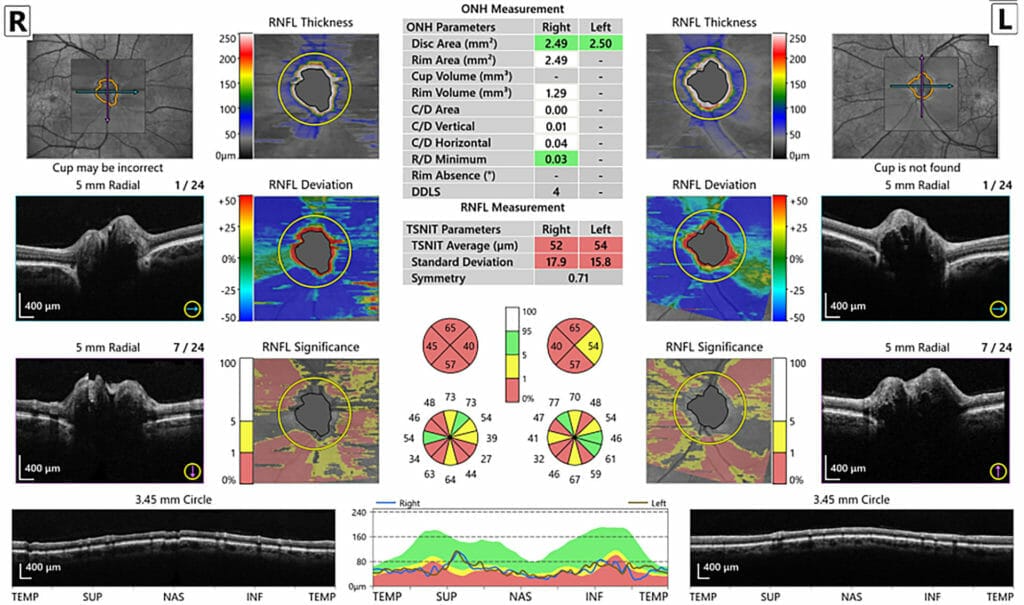
Figure 3. OCT confirmed optic nerve head drusen.

Figure 4. OCT confirmed significant retinal nerve fibre layer drop out at the macula.
Intraocular pressures (IOPs) were R and L 11mHg at 11am.
Visual field examination revealed constricted visual fields R>L (Figure 5).
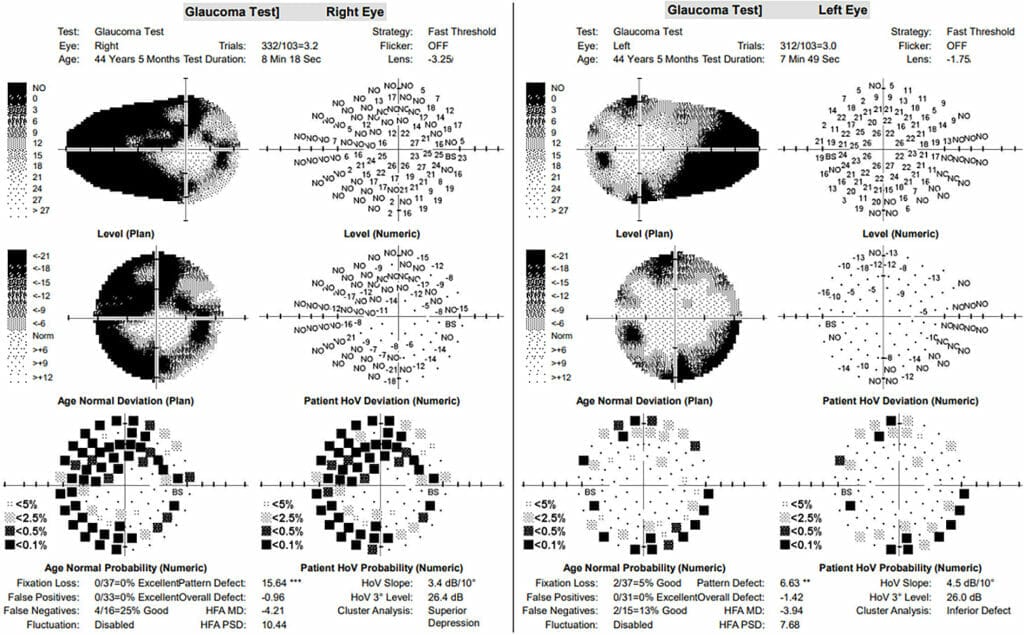
Figure 5. First visual field examination revealed constricted visual fields.
Nigel’s previous optometrist was contacted to obtain his history. Visual field testing had been performed and was reported normal eight years prior. Visual field examination was repeated four weeks later and fortunately, the results were improved compared to previous (Figure 6).
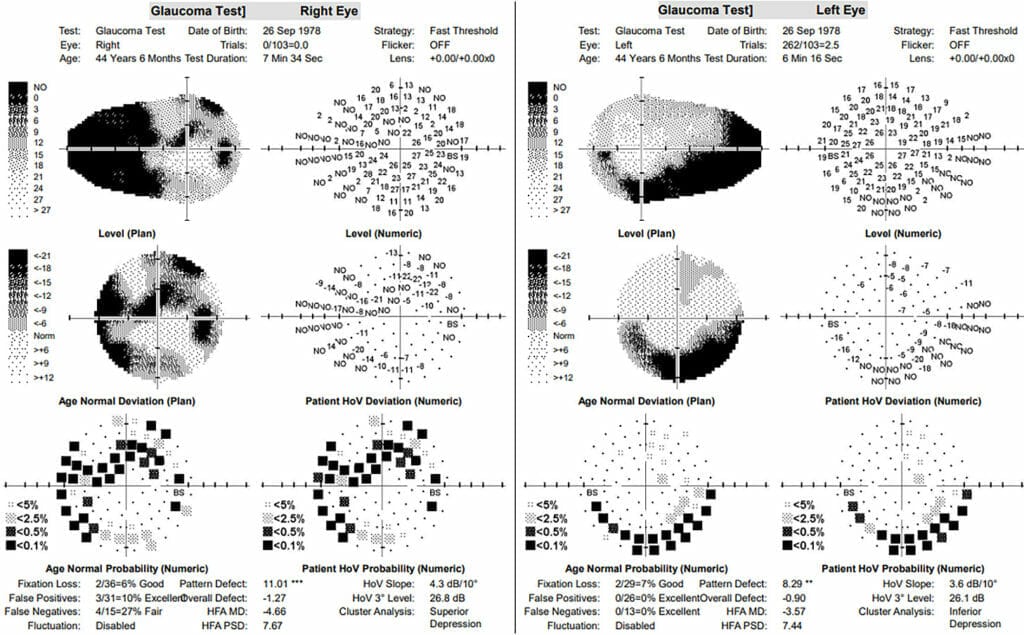
Figure 6. Improved visual field results four weeks later.
Discussion
Optic nerve head drusen (ONHD) are calcified deposits comprised of various acellular components including calcium, mucopolysacharides, nucleic acids and amino acids, that accumulate within the optic nerve head. These deposits occur posterior to Bruch’s membrane and anterior to the lamina cribrosa. Diagnosis is made through fundus examination with imaging tests including OCT or B-scan ultrasonography.
ONHD can impair axonal transport in the optic nerve and compress the retinal nerve fibres, resulting in decreased perfusion of the optic nerve head. This may give rise to optic neuropathy and retinal nerve fibre layer thinning, which in turn leads to visual field loss, and rarely, non-arteritic anterior ischemic optic neuropathy. The prevalence is between 0.3 to 2.4% of the population, and bilateral in 75%.1
It is critical to rule out optic nerve oedema or papilloedema as these can be caused by increased intracranial pressure, which can have serious implications if the result of intracranial masses, central nervous system inflammation, or cerebral venous thrombosis. Other differential diagnoses include optic neuritis, glaucoma, non-arteritic anterior ischemic optic neuropathy, or optic nerve glioma.
Impact On Visual Acuity
The impairment of visual acuity from ONHD is uncommon and patients presenting with ONHD are normally asymptomatic. However, ONHD can commonly give rise to visual field defects, which appear in 24% to 87% of adults,2 with abnormal visual fields more prevalent in those with visible drusen than buried drusen.
Visual fields may be stable and generally progress slowly, however rarely, some progress rapidly. As there is such variability in the disease course, patients should be monitored on a regular basis, including changes on fundus examination, OCT, and visual fields.
Treatment Options
Although there is no known cure for ONHD, there are several commonalities between ONHD and glaucoma, where the mainstay of therapy is IOP lowering therapy. IOP lowering therapy has been successful in treating other optic neuropathies in the absence of elevated IOP, notably normal tension glaucoma (NTG).3 The Collaborative Normal-Tension Glaucoma Study found that reducing IOP by 30% from baseline in patients with normal IOP reduced risk of visual field progression from 80% in untreated to 40% in treated eyes over five years.4 Subsequently, some patients with ONHD have been treated with IOP reducing therapy. Brimonidine is often used because, as well as lowering IOP, it has presumed neuroprotective benefits. However, as ONHD and NTG are different diseases, there is debate about the use of IOP lowering therapy. There is presently limited scientific evidence for the benefits of IOP reduction in ONHD, and there appears to be no correlation between IOP and visual field defects in ONHD.
Nigel’s Progression
Nigel’s first visual field test (Figure 5) was alarming due to the apparent reduction in his visual field. It was even more alarming when we determined that his visual field had been normal eight years prior. This suggested that he had rapidly progressing visual field loss.
Visual field testing relies on the observer’s ability to produce reliable results – this can be influenced by a patient’s poor concentration, by them being overly conservative, or over-zealous, and there is some degree of learning involved. Visual field tests need to be repeated to ensure reliability, and fortunately Nigel’s visual field test results were improved on the second exam, suggesting he was overly conservative in his first test. Being Nigel’s first presentation to the practice, we could not ascertain whether his visual field loss was stable or progressive without some history. Fortunately, intra-professional relationships in optometry in Australia are generally professional, uncomplicated, and patient-centric and Nigel’s previous history was easily obtained.
If Nigel’s visual field defects had been similar to those recorded in the past, the level of concern would have been much less. However, given the significant change over the years, we provided Nigel with thorough counselling regarding the implications and prognosis of his ONHD. We discussed the use of IOP lowering therapy, however given his already relatively low IOP and lack of clinical evidence, Nigel was happy with a six-month review. We agreed to administer IOP lowering therapy should there be further progression.
*Patient name changed for anonymity.
Jessica Chi is the director of Eyetech Optometrists, an independent specialty contact lens practice in Melbourne. She is the current Victorian, and a past national president of the Cornea and Contact Lens Society, and an invited speaker at meetings throughout Australia and beyond. She is a clinical supervisor at the University of Melbourne, a member of Optometry Victoria Optometric Sector Advisory Group and a Fellow of the Australian College of Optometry, the British Contact Lens Association and the International Academy of Orthokeratology and Myopia Control.
References
1. Auw-Haedrich, C., Staubach, F., Witschel, H., Optic disk drusen. Surv Ophthalmol. 2002; 47:515–532.
2. Morris R.W., Ellerbrock J.M., Hamp A.M., et al., Advanced visual field loss secondary to optic nerve head drusen: case report and literature review. Optometry. 2009 Feb;80(2):83-100
3. Falardeau J.M., Pineles S.L., Van Stavern G.P., Lee A.G.. Should patients with optic disc drusen be treated with intraocular pressure-lowering medications? J Neuroophthalmol. 2020 Dec;40(4):538-543.
4. Anderson D.R., Collaborative normal tension glaucoma study. Curr Opin Ophthalmol. 2003 Apr;14(2):86-90





