
As a speciality keratoconus practitioner for over three decades, and as a forme fruste keratoconus sufferer for five decades, one could say Alan Saks has some skin (or, perhaps, some cornea) in the game.
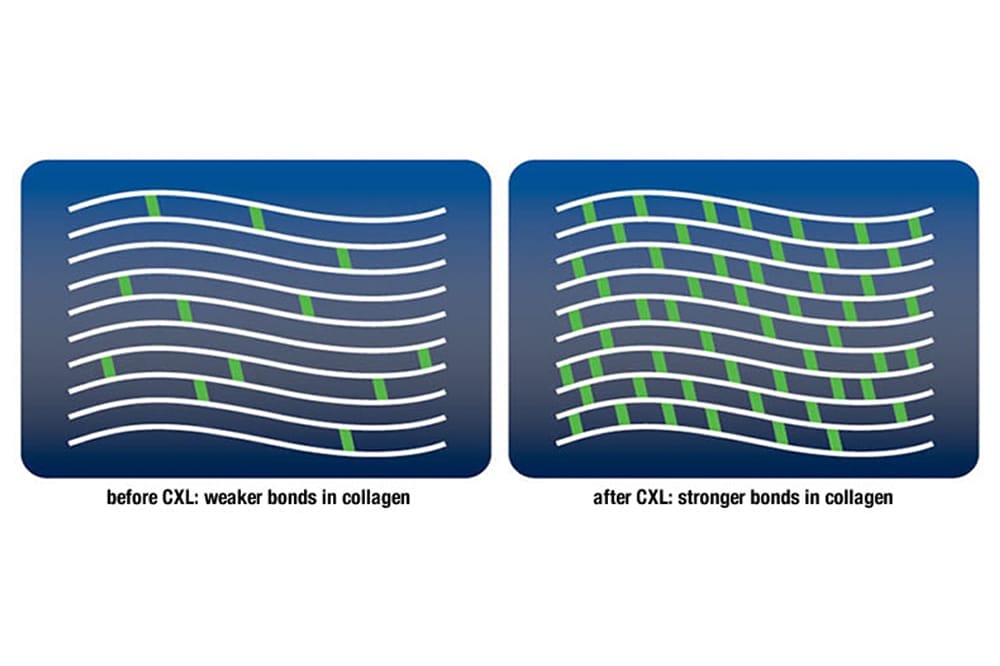
An observation that’s becoming clearer is that since corneal cross-linking (CXL) has become more commonplace over the past two decades, keratoconus (KC) is no longer progressing as much, or as severely, as in the past. KC is now being diagnosed earlier and in younger patients. As soon as evidence of progression is demonstrated, patients are advised to consider cross-linking, even as young as age eight.
An upside of this is that the need for penetrating keratoplasty (PKP) appears to be reduced in KC.
A number of other related elements are also improving the outlook for keratoconus sufferers. We can thank the increased access to topographers as well as better training and continuing education for this. Furthermore, there’s increased awareness and patient education on the need to avoid eye rubbing as a related, and some say causative, factor. We’ve also seen improved management of related allergic conjunctivitis and atopia. Prescribing rights of therapeutic drugs by optometrists are also relevant, providing broader access to treatment.
Corneal grafts were limited to PKP in the past, but these days less invasive techniques – such as deep anterior lamellar keratoplasty and endothelial keratoplasty – are improving outcomes, reducing rejection issues, and other complications, which can make contact lens fitting less of a challenge.
As technology and manufacturing have advanced, the contact lens options now available have greatly improved. The swing to avoiding apical touch in corneal lenses, and avoidance of touch with scleral lenses, means we see less apical scarring than in the past.
With CXL, the cornea is no longer progressing to such extremely steep profiles and marked thinning, reducing the incidence of endothelial rupture and related hydrops. These factors also reduce the need for PKP.
Artificial intelligence-based interpretation of topography, eye surface profiling, and advanced manufacture with four-axis lathes and milling machines, allows for supercomplex contact lenses with increasingly accurate parameters. Bitorics, asymmetric designs, and inclusion of aberration control are some examples. High Dk materials in both rigid gas permeable and soft lenses have also significantly improved outcomes.
However, despite the many advances and the improved outlook for young patients, KC remains a challenging condition that can cause significant anxiety among sufferers and managing practitioners alike.
OTHER CONSIDERATIONS
Laser refractive procedures are occasionally used in some cases of KC. Additionally, we see femtosecond laser assisted intracorneal ring segments and more recently, corneal allogenic intrastromal ring segments (CAIRS), used as another approach to managing keratoconus. Such procedures will, however, likely remain niche procedures and the results are not always as promised or as desired. Contact lens management can also be trickier after such procedures.
We still have many middle-aged and older keratoconus sufferers with advanced keratoconus and challenging PKPs that need close monitoring and expert contact lens management. Steroid eye drops are a boon to halting or even preventing graft rejection if the signs are noted early enough, but long-term use is not ideal. High Dk lenses can prevent or reduce neovascularisation, especially to, or beyond the graft-host junction, again reducing rejection risk. As keratoconus patients mature and cataracts develop, we are most fortunate that developments in cataract surgery and intraocular lens (IOL) designs / options mean ever better outcomes. Small aperture IOLs can be a boon in keratoconus. Toric IOLs can work wonders but should generally be avoided in extreme cases where a patient may still be contact lens dependent post-cataract surgery. Multifocal IOLs should similarly also be avoided, except in mild cases.
KC is one area that shows the benefit of co-management and collaboration between ophthalmology and optometry, along with allergists and other practitioners. The resulting improved relationships and mutual respect between anterior segment specialists and expert contact lens practitioners is of great benefit to patients, which is of course, the most important thing.
There’s much discussion online and at conferences surrounding metrics, indices, and algorithms that can diagnose KC from topography and other instrumentation. To my mind this is somewhat of a moot point, as KC has always been relatively easy to diagnose, simply by picking up your retinoscope and looking for a zonal (‘scissors’) reflex. An old-fashioned manual keratometer will show mire distortion and/or steeper than average keratometry (K) readings. Distortion can be seen on placido rings and with certain multifunction autorefractors. Pachymetry can raise alarm bells. Suspicious readings that don’t add up warrant deeper investigation. Anterior segment optical coherence tomography can show corneal thinning and/ or an atypical profile. Striae, Munson’s sign, and Fleischer’s ring also raise suspicions, but these are usually seen in more advanced cases.
Sub-par best corrected visual acuity should not be written off as amblyopia, and complaints of ghost vision, starbursts, and haloes should never be ignored!
It’s imperative that a diagnosis is made as soon as possible.
GET ON BOARD. IT’S REWARDING
Working with keratoconus has been a hugely rewarding and satisfying aspect of my career. I count sound relationships with patients who appreciated what I did for them. KC management also fostered great relationships with a handful of ophthalmologists – who provided the most fantastic surgical and other management strategies – some I now count among my close friends.
For anyone looking to create a speciality niche in this increasingly challenging eye care marketplace, keratoconus care is something to strongly consider and develop.
For those seeking support, and to develop such skills, the Cornea & Contact Lens Society of Australia – and other such societies around the world – are an excellent place to start. Plenty of keratoconus support, training and mentoring is offered in corneal and scleral lens design, fitting, and management. Topography use and interpretation, along with therapeutic management are other core aspects.
Technological developments have been incredible and continue to amaze. Things like corneal impression moulding derived designs, topographically assisted contact lens design, CXL, grafts, advanced imaging and manufacturing platforms, have changed the face of KC management.






