
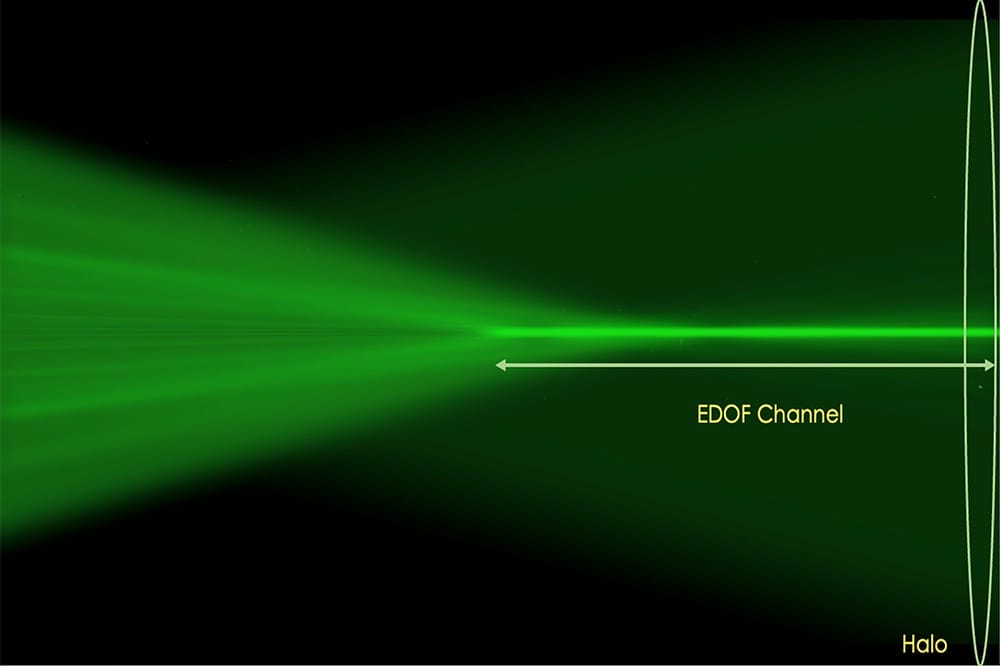
Figure 1. Laser ray tracing of the EDOF channel and diffuse myopic defocus created by the Neurofocus Optics technology of NaturalVue. The retinal place is on the far right of the image.
When considering the data on myopia control, Dr Emma Gillies urges eye care professionals to look outside the box of randomised control trials.
Imagine a bustling marketplace, the smells, the chatter, the vibrant colours of the different stalls. As you walk around, you notice one of the stalls is beautifully presented, with its wares carefully laid out. It’s different to the others, more like a boutique, with what you realise is a select range of carefully procured products. There’s a calmness to this stall, but you notice that not everyone seems to find what they are looking for here. As you continue to walk through the marketplace, you come across an alley that leads to a section that has been long overlooked. It is teeming with vendors offering a vast array of products, each with their own unique story and worth. You notice a diverse range of shoppers here – all ages, backgrounds, and preferences, and they come to this section of the marketplace because it reflects their real life needs and choices.
Historically we have relied upon a single, well-regulated store – a randomised clinical trial (RCT) – for our goods. While this store undoubtedly has its worth (ensuring the highest quality and consistency in its offerings) it may be limited, failing to account for long-term needs or unable to offer products for specific needs. Real world data, on the other hand, is rather like exploring the hidden marketplace, offering a wide range of goods (diverse patient population) and showcasing products in their real-life context; the patients in your chair, not just those limited to the inclusion criteria of the RCT.
REAL-WORLD EFFICACY
Our quest for comprehensive evidence of the real-world efficacy of an intervention is further strengthened when three independent studies reach a common conclusion.
When it comes to choosing an intervention for myopia management, there is a wide range of options to choose from. If a soft contact lens is deemed the most suitable for the child (bearing in mind that the intervention that works best is the one the child wears) there are still multiple options available to practitioners.
We know from the research that a design that corrects central vision clearly while simultaneously inducing peripheral defocus can be effective in slowing myopic progression.1-3 Studies have also shown that both the magnitude of the defocus4-6 (the additional plus in the design) and the location of that plus plays a role in the efficacy of the design.7-10 The higher the add and the greater the total retinal area exposed to this defocus, the greater the treatment effect.
NaturalVue 1 day multifocal with Neurofocus Optics technology is one soft contact lens option that satisfies these criteria. The lens is a centre distance, extended depth of focus (EDOF) design, and was granted CE approval for myopia management in 2018.
So how exactly does this lens design help reduce myopic progression? Neurofocus Optics technology generates an extremely high magnitude of myopic defocus (6–8D). What makes this design unique is the plus power increases in a rapid, smooth, and uninterrupted manner, creating a long and narrow EDOF channel. The high add in the design induces myopic defocus that extends over a wide area of the retina, yet the intensity of this blur is only one fifth as bright as the halo induced by a typical +2.50D add multifocal. This means visual quality and comfort are preserved, minimising haloes and glare (Figure 1).
CONSISTENT OUTCOMES
Three independent retrospective analysis studies have been published recently, demonstrating the consistency in the treatment effect of NaturalVue Multifocal in slowing myopia progression in children. The results of these studies were analysed to compare the outcomes in a group of 108 children wearing the lens after 12 and 24 months of wear.
- NaturalVue monotherapy subgroup analysis from the CAMP study (Clinical Algorithm for Myopia Progression), conducted by Treehouse Eyes,11
- A poster presentation: Myopia control with extended depth of focus multifocal contact lenses,12
- Subgroup analysis (n=66) from NaturalVue six-year retrospective data.13
CARE VALUES
To allow a true comparison of treatment effect, a subgroup of the six-year data was extracted to allow evaluation of data from 66 subjects that matched the age range of the other two studies limited to years one and two of lens wear. The results of the three studies are summarised in Table 1.
Two clear trends can be observed. We know that age and ethnicity are important factors in myopia progression, and while the distributions of each of those factors may be different across these three studies, the results are compellingly similar, with the average progression less than 0.15D (mean 0.10D) at years one and two of wear (Figure 2). This is significantly less than predicted in an age and ethnicity matched virtual control group (n=188, developed from 63 RCTs14-15). As the smallest measurable increment in a refraction is 0.25D, this means that the majority of the 108 children had no change in refractive error during the study period. But mean refractive error changes don’t really show the full picture. Figure 3 shows the individual outcomes for each subject across all three studies.
The axial length data (measured in two of the studies) tells a similar story. Axial length increased, on average, less than 0.10mm per year at 12 and 24 months; this is approximately the amount of axial elongation that would be expected in this time frame in emmetropic children. The cumulative absolute reduction of axial elongation (CARE) value is a measure of how effectively an intervention slows axial elongation (in mm) and is determined by comparing the degree of elongation expected from a virtual control group with the elongation measured in the group wearing the intervention. The CARE value being the difference between the two, measured in mm. This value is designed to help eye care professionals (ECPs) compare the outcomes of different studies more easily. The CARE value in these two groups was significant and comparable at 0.17mm at year one and 0.32mm at year two, compared with an anticipated 0.39mm and 0.47mm from the virtual control group.14-15 These three independent studies demonstrate that the real-world results with NaturalVue are consistent and reliable.
WATCH THIS SPACE!
Just as no shopping trip is complete without a visit to both the well-regulated store and the lively marketplace, keep your eyes peeled for the one-year results of the PROTECT study, the international double blind, randomised controlled clinical trial of children wearing NaturalVue.
The author is employed by Visioneering Technologies Inc, which designs, manufactures, and distributes NaturalVue contact lenses.
Dr Emma Gillies has an optometry degree and PhD from Glasgow Caledonian University. She has her own consultancy business specialising in behavioural dynamics, leadership coaching, selling skills and communication, and is currently the Director of Professional Services for Visioneering Technologies for ANZ.
References
- Smith, E.L. III, Kee, C., Ramamirtham, R., et al. Peripheral vision can influence eye growth and refractive development in infant monkeys. Invest Ophthalmol Vis Sci. 2005 November; 46(11): 3965–3972.
- Smith, E.L. III, Hung, L-F., Huang, J., Relative peripheral hyperopic defocus alters central refractive development in infant monkeys. Vision Res. 2009 September; 49(19): 2386–2392.
- Smith, E. L. III, (2011). Charles F. Prentice Award Lecture 2010: A case for peripheral optical treatment strategies for myopia. Optometry and Vision Science, 88, 1029–1044.
- Woods, J., Guthrie, S., Keir, N., et al., Inhibition of defocus-induced myopia in chickens. Investigative Ophthalmology & Visual Science. 2013;54(4):2662–2668.
- Irving, E.L., Yakobchuk-Stanger, C., Myopia progression control lens reverses induced myopia in chicks. Ophthalmic Physiol Opt. 2017 Sep;37(5):575–584.
- Walline, J.J., Walker, M.K., Mutti, D.O., et al., Effect of high add power, medium add power, or single-vision contact lenses on myopia progression in children. JAMA. 2020;324(6):571–580
- Wallman, J., and Winawer, J., (2004). Homeostasis of eye growth and the question of myopia. Neuron, 43, 447–468.
- Smith, E.L. III, Optical treatment strategies to slow myopia progression: Effects of the visual extent of the optical treatment zone. Experimental Eye Research 114(2013)77–88.
- Smith, E.L. III, Arumugam, B., Hung, L.F., et al., Eccentricity-dependent effects of simultaneous competing defocus on emmetropization in infant rhesus monkeys. Vision Research 177(2020) 32–40.
- Woods, J., Guthrie, S., Keir, N., et al., The effect of a unique lens designed for myopia progression control (MPC) on the level of induced myopia in chicks. Invest Ophthalmol. Vis. Sci. 2011;52: E-abstract 6651.
- Cooper, J., Aller, T., Smith, E.L. III, et al., Retrospective analysis of a clinical algorithm for managing childhood myopia progression. Optom Vis Sci. 2023 Jan 1;100(1):117–124.
- Lederman, C.R., Myopia control with extended depth of focus multifocal contact lenses. In: American Association for Pediatric Ophthalmology and Strabismus; 29 Mar 2023; New York, USA.
- Cooper, J., O’Connor, B., Aller, T., et al., Reduction of myopic progression using a multifocal soft contact lens: A retrospective cohort study. Clin Ophthalmol. 2 Jul 2022;16:2145–2155.
- Brennan, N.A., Toubouti, Y.M., Cheng, X., Bullimore, M.A., Efficacy in myopia control. Prog Retin Eye Res. 2021;83:100923. DOI:10.1016/j. preteyeres.2020.100923.
- Brennan, N.A., Why “CARE” for myopia? Review of myopia management; 1 October 2020.

Table 1. Summary of retrospective analysis. *Included children ages eight to 12 only. †Not all values cycloplegic. ‡Virtual control not available.

Figure 2. Cumulative refractive error change at 12 and 24 months for each study cohort.

Figure 3. Magnitude of refractive error change for individual subjects in each of the study cohorts (x axis represents each subject).








