
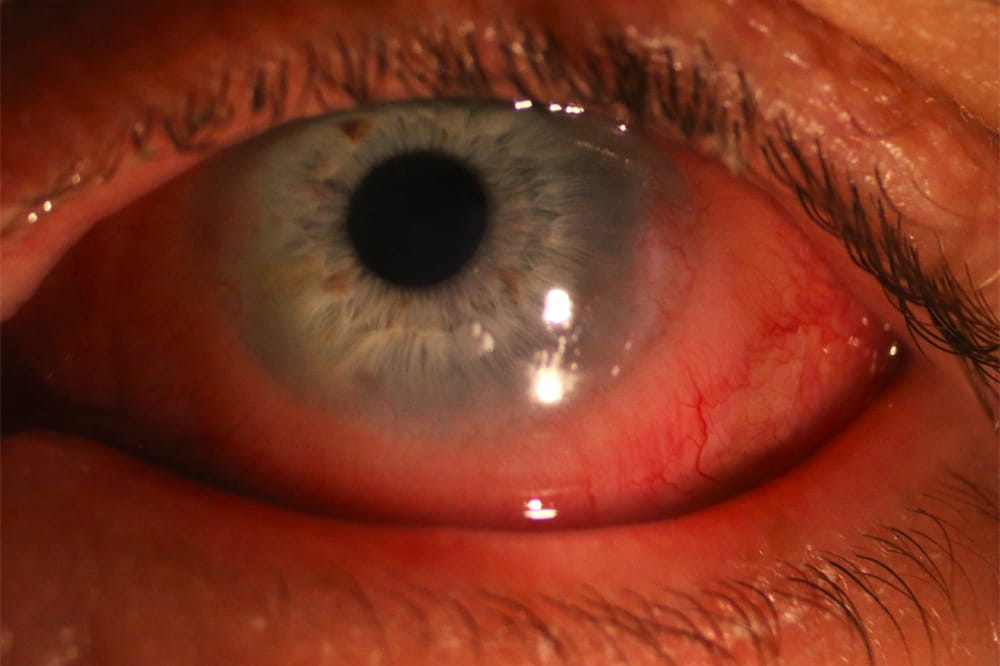
Figure 1. The patient presented with red, watery eyes and swollen eyelids.
Scleral lenses are a gamechanger for keratoconic patients, however they are not without complications, so careful fitting and regular review is essential.
Mr James,* a 46-year-old male, presented complaining of sore, red, irritated eyes beginning three weeks prior. Over the previous three days his symptoms had worsened to the extent that he could barely wear his scleral contact lenses. He reported cloudy vision in his left eye, and constant irritation and soreness with his contact lenses. Mr James suffers from bilateral keratoconus and extreme ocular allergies.
He typically manages well with his contact lenses, experiencing few problems aside from occasional episodes of severe allergies when he struggles to tolerate his contact lenses.
Even before Mr James entered the consult room, it was evident that his eyes were inflamed. They appeared bright red, his eyelids were swollen, and his eyes were watery (Figure 1). He also displayed signs of photophobia, wearing sunglasses indoors.
Compared with his last consult only four months prior, Mr James’ vision with his contact lenses had reduced from R 6/9, L 6/7.5 to R 6/9 and L 6/38. Examination of his left contact lens revealed 600 microns of clearance over the cornea at the apex, and over 800 microns elsewhere (Figure 2).

Figure 2. Contact lens with 600 microns of clearance over the cornea.
As a practitioner, I momentarily panicked, wondering if I had fitted the lenses with too much clearance, or if the wrong lens had been dispensed. However, Mr James had not received a lens since before his last consultation, during which his lenses were well fitting with 200 microns of clearance over the corneal apex (Figure 3). I suspected he had mixed up his lenses as his right eye is more advanced, requiring a contact lens with greater sagittal depth, however there was less than 100 microns of difference in sagittal height between the right and left lenses. A quick inspection of the contact lens engravings confirmed that Mr James was wearing the same pair as at the last visit, so I concluded that the eye had changed. Further examination revealed that the lenses were also landing on the limbus, which exhibited significant oedema (Figure 4).

Figure 3. Lens clearance at initial fitting

Figure 4. Oedema at the limbus and contact lens touching.
Scleral contact lenses are usually forgiving in fit, as small changes in the keratoconus typically do not have an impact unless the lens has been fitted with insufficient clearance. However, if keratoconus was to progress, we would expect less, not more clearance. It is very odd to review a patient with significantly more clearance than prior exams. Assessment of the contact lenses revealed tight edges, and examination showed significant limbal oedema with raised, fluid filled cysts (Figure 5), and marked conjunctival oedema and hyperaemia L>R. There was extensive corneal neovascularisation and lipid keratopathy with significant haze and oedema superiorly. The corneal haze, reduction in vision, and dramatic change in fit led to suspicions of corneal hydrops, however no breaks in Descemet’s membrane were noted.

Figure 5. Fluid filled cysts on the limbus.
Mr James was diagnosed as having extreme allergic conjunctivitis, which caused the change in his contact lens fit in the left eye. Scleral lenses are named as such because they land on the sclera – or to be technically correct, the bulbar conjunctiva (which overlays the sclera). Mr James’ resultant conjunctival oedema was so dramatic that it elevated the lens off the eye, resulting in excess corneal clearance. Continued wear of the lens for many hours every day induced corneal hypoxia, leading to a cycle of further limbal oedema, further elevation of the contact lens over the cornea, and so forth.
DISCUSSIONS
cleral lenses have been a gamechanger for patients suffering with keratoconus: patients who were previously considered ‘unfittable’ can become successful scleral contact lens wearers. They are relatively easy to fit and well tolerated by patients, providing an option for those who are intolerant to corneal rigid gas permeable lenses due to lens discomfort. Scleral lenses also enable practitioners to vault over highly ectatic and displaced cones, which may have been a challenge to fit with corneal lenses.
However, as these lenses are a ‘sealed lens system’, there has been debate about their oxygen transmissibility. The contact lens itself is an obvious barrier to the oxygen passing through the system. What has also become apparent is that the post-lens tear film, or the fluid reservoir beneath the lens is also a barrier. To maximise oxygen transmissibility, the lens should be manufactured in a highly oxygen-permeable material with minimal lens thickness. However, it should not be so thin that it becomes fragile and subsequently prone to breakage and flexure.
Studies have confirmed that a larger tear reservoir results in less oxygen delivery to the cornea – it has been shown that the oxygen delivered to the cornea is reduced by 30% for a 400 micron tar reservoir compared to a 200 micron tear reservoir.1 However, these lenses tend to ‘settle’ over time, resulting in reduced tear reservoir throughout wear.
With this in mind, the goal when fitting should be to ensure the lens never touches the surface of the cornea. In keratoconus, the apex of the cornea is ectatic and thin, and needs to be avoided at all costs as a lens rubbing on the apex can result in progression of keratoconus and corneal scarring. Consequently, there needs to be a balance between a lens with clearance enough to ensure no contact between the cornea and the contact lens, but not so much that hypoxia results.
Limbal oedema causes hypoxia, which causes the lens to land on the cornea. This mechanical stress can disrupt the epithelial tight junctions, causing fluid to accumulate between these cells, which can then trigger an immune reaction, resulting in corneal neovascularisation2 as was the case for Mr James.
Further hypoxia results in further corneal oedema. At 5% corneal oedema there is a loss of tissue transparency, resulting in stromal haze.3 This was the main cause of the reduction in vision for Mr James, coupled with the increased debris in the tear reservoir caused by excess clearance and increased inflammation.
THE SOLUTION
Mr James was instructed to cease contact lens wear for his left eye, and topical corticosteroids (Prednefrin Forte) were prescribed. At review two weeks later, the corneal oedema had reduced but not completely subsided. He was counselled to avoid allergens where possible, which was not easy given his extreme level of atopy. He was advised to consult an allergist to consider desensitisation. The Prednefrin Forte was tapered, and he was prescribed compounded topical ciclosporin 1% to be used twice daily on an ongoing basis.
*Patient name changed for anonymity.
 Jessica Chi is the Director of Eyetech Optometrists, an independent speciality contact lens practice in Melbourne. She is the current Victorian, and a past National President of the Cornea and Contact Lens Society, and an invited speaker at meetings throughout Australia and beyond. She is a clinical supervisor at the University of Melbourne, a member of Optometry Victoria Optometric Sector Advisory Group and a Fellow of the Australian College of Optometry, the British Contact Lens Association, and the International Academy of Orthokeratology and Myopia Control.
Jessica Chi is the Director of Eyetech Optometrists, an independent speciality contact lens practice in Melbourne. She is the current Victorian, and a past National President of the Cornea and Contact Lens Society, and an invited speaker at meetings throughout Australia and beyond. She is a clinical supervisor at the University of Melbourne, a member of Optometry Victoria Optometric Sector Advisory Group and a Fellow of the Australian College of Optometry, the British Contact Lens Association, and the International Academy of Orthokeratology and Myopia Control.
References
- Glasson, C.J., Morency, J., Melillo, M., Michaud, L., Oxygen tension beneath scleral lenses of different clearances. Optom Vis Sci. 2017 Apr;94:466–475.
- Michaud, L., Vincent, S. Scleral lenses and hypoxia: A balanced approach. Contact Lens Spectrum, 2019, 34:40–42.
- Van der Worp, E., Garcia-Porta, N., GonzálezMéijome, J.M., Modern scleral contact lenses: A review. Cont Lens Anterior Eye. 2014 Aug;37:240–250.





