

Choroidal folds can be an intriguing clinical finding as they may be associated with a plethora of ocular and extraocular diseases, and thus require further investigation to identify the underlying cause. In this article, Carol Chu explores the clinical characteristics of choroidal folds to understand how and why they form, and investigates some of the disease associations.
Choroidal folds appear clinically as alternating light and dark subretinal lines due to undulations in Bruch’s membrane, the retinal pigment epithelium (RPE), or inner choroid.1,2 They can follow a parallel horizontal, vertical, or oblique arrangement, and radiating or concentric patterns have also been described. They vary greatly in number and may be unilateral or bilateral, but they are typically found in the posterior pole, most commonly temporal to the optic nerve head.3,4 Choroidal folds associated with optic disc swelling can either radiate from the disc or form concentric arcs around the disc.2,5
If the overlying neurosensory retina is involved, they are termed chorioretinal folds.
The pathophysiology and management are essentially the same in both choroidal and chorioretinal folds and as such, the term ‘choroidal folds’ is used for the purposes of this article. Figure 1 illustrates the structural differences between choroidal folds, chorioretinal folds, and retinal folds.
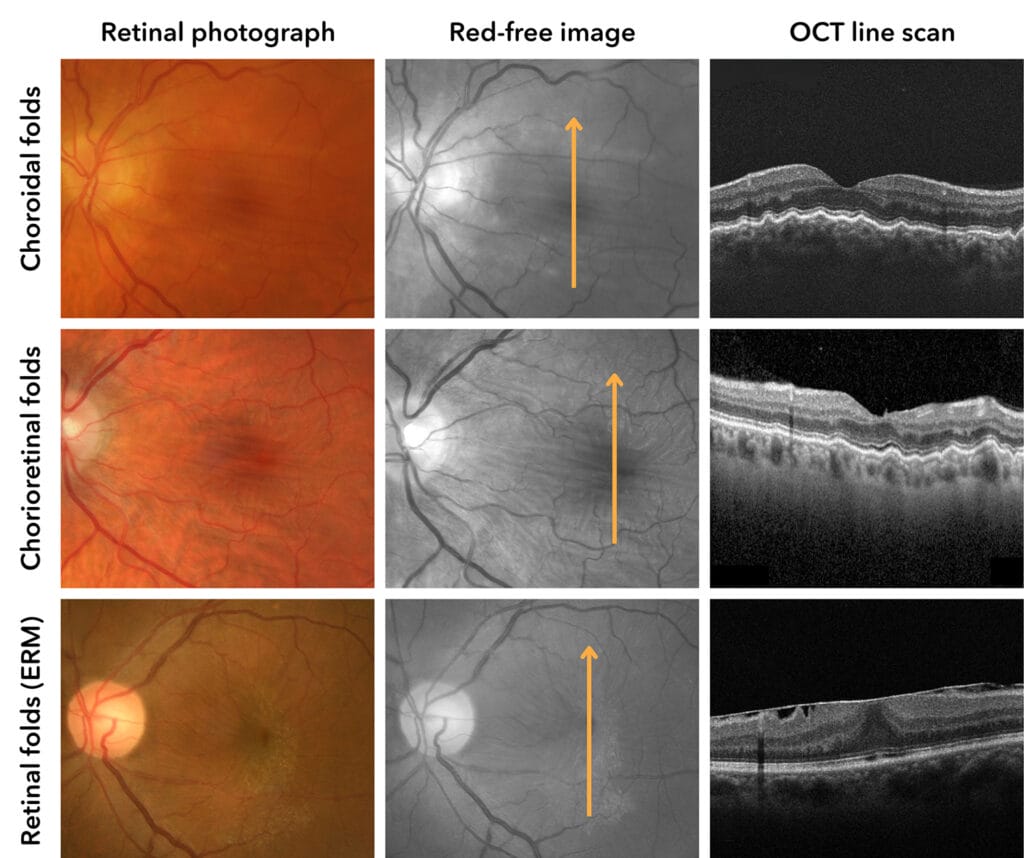
Figure 1. Structural differences between choroidal folds, chorioretinal folds, and retinal folds.
Striations due to retinal folds are generally thinner than those observed in choroidal folds, often radiate from pathological lesions in the retina, and only impact the superficial layers of the retina. There is often some anomaly at the vitreoretinal interface; commonly epiretinal membrane (ERM), and there may be an associated increase in tortuosity of retinal vasculature.
IMAGING CHOROIDAL FOLDS
As can be seen in Figure 1, the alternating light and dark lines observed in choroidal folds are best appreciated in optometric practice with red-free (green filter) viewing.
Historically, fundus fluorescein angiography (FA) was considered the preferred technique for detection and diagnosis of choroidal folds as it is more sensitive than ophthalmoscopy and fundus photography. At the crest of a choroidal fold, the RPE is thinner, allowing a greater transmission of choroidal fluorescence so that a bright (hyperfluorescent) line is observed. Conversely, there is compacted RPE at the trough of a choroidal fold and hence a dark (hypofluorescent) line is seen. There is no leakage of fluorescein.1 Fluorescein angiography can also assist in the detection of some underlying causes of choroidal folds, such as choroidal neovascularisation and posterior scleritis.
In practice, fundus autofluorescence (FAF) imaging is much more accessible to optometrists than FA, and this imaging modality yields the opposite light/dark pattern to fluorescein angiography. At the crest of a choroidal fold there is a relatively lower density of RPE cells and thus lipofuscin, so that a dark line is observed. The compacted RPE cells along the trough form a hyper-autofluorescent line.
At present, however, structural optical coherence tomography (OCT) is the favoured imaging tool in aiding diagnosis and characterisation of choroidal folds. Aside from the benefits of being a non-invasive and widely available imaging modality, the crosssectional visualisation of retinal architecture on OCT allows for confirmation of the undulations of the choroid, RPE, and retina (when involved) when the line scans are taken perpendicular to the folds.
When imaging suspected choroidal folds, it is important to realise that the (typically) horizontal folds will not be visible on a horizontal line scan as they follow the crest or trough of the fold. A vertical or radial macular line scan will show the structural changes much more clearly, as in Figure 2.

Figure 2. OCT line scans taken perpendicular (left) vs parallel (right) to the direction of choroidal folds, with undulations at the level of the choroid/RPE readily visible on the perpendicular scans.
FORMATION OF CHOROIDAL FOLDS
Choroidal folds are associated with an extensive range of potential causes, and understanding these can aide in the differential diagnosis of causative conditions. The pathological structural changes associated with choroidal folds include the following, which may occur independently or in combination, depending on the causative condition:2,3
- Contraction of the RPE/Bruch’s membrane. The collagenous composition and elastic properties of Bruch’s membrane allow it to corrugate or ‘buckle’ as it shortens.6
- Thickening of the choroid from congestion in the choriocapillaris.
- Scleral shrinkage, thickening or deformation.1 These structural changes may be the result of inflammation or tractional/mechanical forces.
- Reduced rigidity of the sclera.
CONDITIONS CAUSING CHOROIDAL FOLDS
There are many conditions that can cause choroidal folds, and these are outlined in Table 1. The most common causes of monocular choroidal folds are scleritis, hypotony, and ocular tumours, with binocular cases more commonly attributed to age-related macular degeneration (AMD), hyperopia, and idiopathy.1 Before coming to a diagnosis of idiopathic choroidal folds, it is vital that all other differential diagnoses be excluded. Regression of choroidal folds occurs in some cases following treatment of the underlying cause, however there may be adaptive remodelling of the outer retinal and RPE layers leading to persistent folds.

Table 1. Conditions causing choroidal folds.
MANAGEMENT OF PATIENTS PRESENTING WITH CHOROIDAL FOLDS
Choroidal folds are usually noted as an incidental finding in an asymptomatic patient during routine eye examination. Management should be directed at diagnosis and treatment of the underlying cause, and as such it is important to analyse the specific features of each individual case. Diagnosis and management of the causative condition may require a multidisciplinary approach, and effective communication, history taking, appropriate referral and collaboration are paramount.
Reduced visual acuity or metamorphopsia may occur if the choroidal folds develop acutely, and particularly if the macula is involved. Symptoms relating to the underlying cause of choroidal folds can also arise; it is pertinent to ask about symptoms of intracranial hypertension such as headaches, nausea, vomiting or visual disturbances.
A thorough ocular and medical history should be taken to try to determine an underlying cause. Intraocular pressure should be measured to rule out hypotony and investigation for signs of intra or extraocular inflammation, pain or optic disc swelling should be undertaken. In some cases, repeating OCT and visual field examination within a fairly short time interval of a few months may be indicated to monitor for change to rule out intracranial hypertension. In the absence of any notable abnormalities, consider referral for B-scan ultrasound.
Unilateral cases are more likely to be associated with orbital disease than bilateral cases and further orbital imaging such as CT (computed tomography) scan or MRI (magnetic resonance imaging) may be required as well as complete ocular examination. When there are no detectable ocular or orbital diseases with ocular imaging, careful patient history and referral to rule out associated systemic autoimmune, inflammatory or infectious diseases should be considered.11
Idiopathic cases and those associated with acquired hyperopia should be monitored routinely. Focal RPE defects can develop along choroidal folds, which may predispose to choroidal neovascularisation development. As such regular monitoring is recommended.14
CONCLUSION
As a clinician, it is important to understand that choroidal folds are usually not a benign finding. They are formed due to alterations in the tension on the sclera, choroid, Bruch’s membrane or RPE, usually occurring when there is a change in size of these structures or there is physical pressure on or near these structures. Although they can be an idiopathic clinical finding, a discovery of choroidal folds always warrants investigation into an underlying cause, which can be intraocular or extraocular.
Carol Chu BOptom (Hons) GradCertOcTher is a senior staff optometrist at Centre for Eye Health Australia (CFEH). Ms Chu received her Bachelor of Optometry and Graduate Certificate in Ocular Therapeutics from the University of New South Wales, also receiving the University Medal. She has worked in private and corporate optometric practices and joined the CFEH in 2011.
The author thanks Michele Clewett and Michael Yapp for their assistance in reviewing this article.
References
- Leahey, A.B., Brucker, A.J., Wyszynski, R.E., Shaman P., Chorioretinal folds. A comparison of unilateral and bilateral cases. Arch Ophthalmol. 1993 Mar;111(3):357–9.
- Grosso. D., Borrelli. E., Querques, G,. et al., Recognition, diagnosis and treatment of chorioretinal folds: current perspectives. Clin Ophthalmol. 2020 Oct 19;14:3403–3409.
- Jaworski, A., Wolffsohn, J.S., Napper, G.A., Aetiology and management of choroidal folds. Clin Exp Optom. 1999 Sep-Oct;82(5):169–176.
- Agrawal, M., Tripathy, K., Choroidal folds. 2023 Aug 25. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan– . PMID: 32491704.
- Cassidy, L.M., Sanders, M.D., Choroidal folds and papilloedema. Br J Ophthalmol. 1999 Oct;83(10):1139–43.
- Bullock, J.D., Egbert, P.R., Experimental choroidal folds. Am J Ophthalmol. 1974 Oct;78(4):618–23.
- Tran, A.Q., Zhang-Nunes, S.X., Wester, S.T., Thyroid eye disease with choroidal folds. Orbit. 2021 Jun;40(3):206–214.
- Ishida, T., Shinohara, K., Ohno-Matsui, K., Chorioretinal folds in eyes with myopic staphyloma. Am J Ophthalmol. 2015 Sep;160(3):608–613.
- Giocanti-Auregan, A., Lavia, C., Gaudric, A., Grenet, T., Cohen, S.Y., Staphyloma-related chorioretinal folds. Am J Ophthalmol Case Rep. 2020 May 26;19:100747.
- Vermeirsch, S., Testi,I., Pavesio, C., Choroidal involvement in non-infectious posterior scleritis. J Ophthalmic Inflamm Infect. 2021 Oct 27;11(1):41.
- Bagnis, A., Cutolo, C.A., Traverso, C.E., Chorioretinal folds: a proposed diagnostic algorithm. Int Ophthalmol. 2019 Nov;39(11):2667–2673.
- Kalina, R.E., Mills, R.P., Acquired hyperopia with choroidal folds. Ophthalmology. 1980 Jan;87(1):44–50.
- Murdoch, D., Merriman, M., Acquired hyperopia with choroidal folds. Clin Exp Ophthalmol. 2002 Aug;30(4):292–4.
- Olsen, T.W., Palejwala, N.V., Yeh, S., Chorioretinal folds: associated disorders and a related maculopathy. Am J Ophthalmol. 2014 May;157(5):1038–47.





