
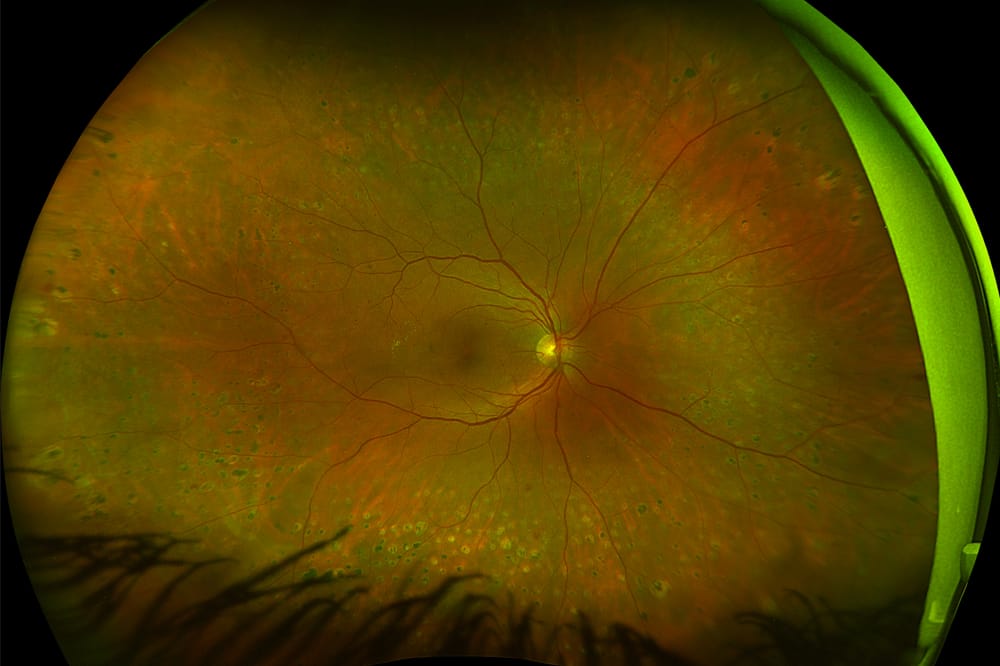
Proliferative diabetic retinopathy post PRP.
As an eye care professional with a special interest in diabetes-related eye disease for almost 20 years and, having lived with type 1 diabetes for over 32 years, Dr Amira Howari’s journey has been deeply intertwined with a commitment to bridging the gap in our healthcare system. Throughout her career, she has become increasingly determined to help build a robust, holistic, and collaborative multidisciplinary approach to diabetic ocular care.
Navigating the intricate landscape of diabetic ocular care demands a holistic approach that integrates clinical acumen with cutting-edge technology.
With the global prevalence of diabetes reaching unprecedented levels, particularly in countries like Australia where diabetic retinopathy ranks as the leading cause of blindness among working-age adults,1,2 the demand for advanced diagnostic and management strategies has never been more pressing.
In my daily practice, I encounter patients at various stages of diabetic retinopathy, each presenting unique challenges in terms of diagnosis, monitoring, and treatment.
Traditional retinal imaging methods have served as the cornerstone of our diagnostic approach, providing valuable insights into retinal health.3 However, these methods are limited by their inability to capture a comprehensive view of the retina, especially in cases where pathology extends beyond the central macula. Despite this, I previously held the view that retinal scans were somewhat comparable, regardless of the technology used; after all, a scan is a scan.
And then, along came ultra-widefield (UWF) retinal imaging.
A WATERSHED MOMENT
The unveiling and launch of UWF retinal imaging technology in Australia marked a watershed moment in my professional journey. I was fortunate enough not only to operate a newly launched cuttingedge technology but also to undergo a demonstration as a patient. What truly captivated me, however, was not merely its operational simplicity, but the revelation it offered: the chance to witness my own retina with an unprecedented level of clarity, detail, and scope.
Despite years of comprehensive explanations from esteemed retinal ophthalmologists and colleagues, nothing prepared me for the sheer impact of seeing my retinal landscape unfold before my eyes. Seeing my retinal anomalies with such magnification and resolution was profound. The concept that had been explained to me suddenly materialised into a tangible reality on the screen. Though my visual acuity remained unaffected, the subtle changes observed in my retina over time left indelible impressions. They were timely reminders of the silent yet potent effects of diabetic retinopathy.
This transformative experience catalysed a significant shift in my perspective, both personally and professionally. It ignited within me a renewed dedication to the meticulous management of my own diabetes, as well as a heightened awareness of the importance of regular specialist appointments. Moreover, it fundamentally altered my approach to every subsequent diabetes eye consultation, from the routine task of history taking to the nuanced discussions surrounding diabetes management, and the painstaking examination of the retina.
As a clinician living with type 1 diabetes, it also triggered an innate responsibility to challenge the status quo and redefine the conventional norms taught in academic settings – a commitment that continues to drive my professional ethos to this day.
THE FUNDAMENTAL ADVANTAGES OF UWF

OptosAdvance automatically arranges modalities according to the individual user preference.
This expanded view enables better visualisation of peripheral retinal pathology, which is often overlooked with traditional imaging methods. As a clinician, this enables us to better identify and monitor subtle retinal changes in areas previously inaccessible with conventional imaging techniques.
Additionally, UWF retinal imaging devices significantly enhance the patient experience during retinal examination, due to the nonmydriatic imaging feature.6
Although this does not remove the need for dilation upon indication, it certainly serves to capture a comprehensive view of the retina without the need of dilation in many routine cases, eliminating the associated discomfort and inconvenience. This feature also increases compliance with regular screening protocols, ultimately leading to better long-term outcomes.
The patient experience is also enhanced with UWF technology’s speed and ease of use. The ability to capture high-quality images quickly, often within seconds, streamlines the imaging process and minimises patient wait times. This efficiency is further enhanced by the intuitive interface system, which allows for integration into the daily workflow.7
From a clinician’s perspective, one of the most significant advantages of UWF retinal imaging is its impact on patient education and engagement. Being able to visually demonstrate retinal pathology on widefield images has proven invaluable in helping patients understand the significance of their condition and the importance of regular eye examinations. The ability to share these images with patients fosters open communication and empowers them to take an active role in managing their eye health.
Undeniably, the documentation and tracking capabilities of UWF retinal imaging have also revolutionised the way we monitor disease progression and treatment outcomes. The digital storage and easy accessibility of retinal images enable clinicians to track changes in retinal health over time, facilitating more informed decision making and personalised treatment plans for each patient.
In recent years, UWF retinal imaging has been the focus of extensive research and development aimed at optimising its capabilities and clinical utility. Studies have highlighted its effectiveness in detecting diabetic retinopathy and other retinal pathologies with high sensitivity and specificity.8,9 Additionally, advancements in imaging technology have led to improvements in image resolution, allowing for even greater detail and accuracy in the visualisation of retinal structures.
The accompanying software of UWF retinal imaging devices has also been instrumental in enhancing the ability to evaluate and analyse retinal images effectively. With features such as zoom functionality, measurement tools, image enhancement filters, annotation tools, comparative analysis, and export and sharing options, the software streamlines the interpretation process and ensures accurate and comprehensive assessments of retinal health.
THE POWER OF CONSISTENCY
When optometrists and ophthalmologists comanage patients with diabetic eye disease, it is important that they use the same technology because consistency in retinal imaging has never been more critical for early detection and comparing results over time.
When different devices are used, we find that optometrists and ophthalmologists will repeat the assessment to ensure reliability, repeatability, and consistency when comparing results over time. This considerably adds to the burden of care for patients, their carers, the providers, and economy.
Ultra-widefield retinal imaging has transformed the delivery of diabetic ocular care. With ongoing advancements in research and technology, UWF retinal imaging will continue to support eye care professionals in their efforts to prevent vision loss for these patients.
 Dr Amira Howari BOptom (Hons) GradCertOcTher MOptom (UNSW) is a senior clinical optometrist; healthcare industry and motivational keynote speaker; a Diabetes Australia and KeepSight Ambassador; and former Optometry Australia Councillor (NSW/ACT).
Dr Amira Howari BOptom (Hons) GradCertOcTher MOptom (UNSW) is a senior clinical optometrist; healthcare industry and motivational keynote speaker; a Diabetes Australia and KeepSight Ambassador; and former Optometry Australia Councillor (NSW/ACT).
Dr Howari has worked in corporate, independent, ophthalmology, and pharmaceutical settings; and at the University of New South Wales as a guest lecturer and clinical supervisor. She currently serves as a member of the Diabetes and Endocrine Network – Agency of Clinical Innovation (NSW Health).
References
- 2019 Global Burden of Disease Collaborative Network. Global Burden of Disease Study 2019. Seattle, United States: Institute for Health Metrics and Evalu.ation (IHME), 2020.
- Tan, C.S., Chew, M.C., Lim, L.W., Sadda, S.R., Advances in retinal imaging for diabetic retinopathy and diabetic macular edema. Indian J Ophthalmol. 2016 Jan;64(1):76–83. DOI: 10.4103/0301-4738.178145.
- Shoughy, S.S., Arevalo, J.F., Kozak, I. (2015). Update on wide- and ultra-widefield retinal imaging. Indian Journal of Ophthalmology. 63. 575–81. DOI. 10.4103/0301-4738.167122.
- Optomap ultrawidefield advances. Available at optos. com/ globalassets/public/optos/providers/clinical-papers/css-uwfadvances- us.pdf.
- Nanegrungsunk, O., Patikulsila, D., Sadda, S.R., Ophthalmic imaging in diabetic retinopathy: A review. Clin Exp Ophthalmol. 2022 Dec;50(9):1082–1096. DOI: 10.1111/ ceo.14170.
- Ellery, B., Milverton, J., Merlin, T., Retinal photography with a non-mydriatic retinal camera in people with diabetes. MSAC application no. 1181 Assessment Report; 2014. Commonwealth of Australia, Canberra, ACT.
- Optos. (2023). Optos Ultra-Wide Field Imaging Software Manual.
- Piyasena, M.M.P., Murthy, G.V.S., Kamalakannan, S., et al., Systematic review and meta-analysis of diagnostic accuracy of detection of any level of diabetic retinopathy using digital retinal imaging. Syst Rev. 2018 Nov 07;7(1):182. DOI: 10.1186/ s13643-018-0846-y.
- Hassan, B., Raja, H., Hassan, T. et al. A comprehensive review of artificial intelligence models for screening major retinal diseases. Artif Intell Rev 57, 111 (2024). DOI: 10.1007/s10462- 024-10736-z.
Amira’s Story
Amira was just eight years old when she was diagnosed with diabetes type 1.

Amira as a child.
“It was during the school holidays, and naturally being eight, I indulged in snacks and sweets that were usually reserved for weekends and holiday breaks. Unfortunately, it didn’t take long before I fell ill,” she explained to mivision.
“That day Mum took me to our local GP and they ran some tests. Diabetes was mentioned but before we could receive the results, I ended up in hospital. By that time, I was dehydrated. I couldn’t walk and it turned out my blood glucose levels were extremely high.”
The mention of a possible diabetes diagnosis turned out to be Amira’s new reality.
Amira’s family knew little about diabetes and, having migrated to Australia from Egypt just four years prior, cultural and language barriers made coming to terms with the diagnosis harder.
“Medical care for people with diabetes in Egypt was different to that available in Australia back in the day. When the diagnosis was translated for them, they were concerned about my life expectancy, and for me it was all doom and gloom. Listening in, I thought it was a terminal illness.”
RAPID LEARNING CURVE
Amira spent several months in hospital recovering and during that time, learnt how to manage her new life with diabetes.
“I grew up very quickly and learned a lot around nutrition in a relatively short timeframe – from calculating carbohydrates and sugars to portions and calculating how much insulin to give per 15 grams of carbohydrates. I had to learn about the correlation between energy and carbohydrates versus sugars, and what role saturated versus unsaturated fats had on my meals,” she said.
“I recall my mother could not look at needles; it was one of the reasons she turned down studying medicine. Despite this, she overcame her fears in order to be shown how to draw up syringes and administer insulin injections. I recall both of us having to sit down with the diabetes educator as we learnt how to draw up the insulin from the vial, flick the bubbles up from the syringe, and push out the excess insulin. Never had I imagined I would be doing this at the age of eight,” she said.
Amira said it was a pivotal time for her mother.
“Our staples are rice and bread with every meal – often cooking with various oils and ghee. Overnight, mum made adjustments to what she cooked and how she cooked. Although in theory I could have continued eating the same meals, she wanted to make sure I could calculate my carbohydrates and that I was eating healthily. As such the entire family had a change in diet. They were on the journey with me.”
As a young teenager she said life became a little more complicated again as she navigated eating out with friends.
“It took time for me to tell my friends I had diabetes; for many years I preferred not to talk of it – I just wanted to fit in. But later, as my close circle of friends came to know and I found how supportive they were, I felt more comfortable sharing it with others. At times, it even allowed us to have a laugh, knowing I could bring jellybeans into the classroom. There were often times when a bag of jellybeans would makes its way around the room.”
Over the long term, Amira said the knowledge around nutrition and portion control paid off. Today, healthy eating comes naturally.
LIVING WITH DIABETIC RETINOPATHY
As an optometrist, Dr Amira Howari has long been aware of the ocular complications associated with diabetes, but no more so than when she became pregnant with her first and then second child.
“The moment I found out I was pregnant, I strictly controlled my blood glucose levels and started to have very regular eye work-ups.”
In those early days of her first pregnancy she was told she had signs of “very mild, non-proliferative diabetic retinopathy, which hadn’t been there before – a common finding when blood glucose levels are suddenly strictly managed”.
Without retinal cameras, she was unable to see the retinopathy for herself. However, during her second pregnancy, a few years later, she was able to see imaging of her own retinas.
“It was 2010 when the ultra-widefield retinal camera was launched in Australia. I was one of a select few optometrists invited to the showroom to learn how to use the technology and I won’t ever forget the impression it left. During the training course they said, ‘Would you like a scan done?’. And of course I said ‘yes’”.
“The scan enabled me to see, for the first time, almost my entire retina. And for me, that was a game changer. Looking at an ultra-widefield retinal scan is very different from looking into someone else’s eyes via fundoscopy or ophthalmoscopy. I could see far more of the periphery than I had ever seen before – and I could zoom in to see every micro aneurysm or haemorrhage.
“While I had an image in my mind of what it would look like, I was unprepared for how much laser had already been done to protect my vision.
“I sat there analysing it for so long. Being well aware of the progress of diabetic retinopathy, I remember thinking: if that’s what my retina looks like after a moderate amount of prophylactic PRP, then I had better get more proactive, otherwise I wouldn’t like where I was heading.”
Dr Howari said those first images, and every subsequent image, have reinforced the need to carefully manage her health and to undertake regular diabetes eye examinations with the same eye care professional where possible. They also shaped her approach to managing patients, and the messages she clearly articulates when speaking with them.
INFLUENCE ON PATIENT MANAGEMENT
“The two things that I stress to patients, in terms of eye examinations, are to have a regular optometrist, just as you have a regular GP or a cardiologist, and if you are going to be comanaged, to have consistency in the standard of eye care, the management expectation, and where possible, the equipment used,” she said.
“When it comes to visual fields assessments, we know that in ophthalmology, the gold standard is the Humphreys. And hence, we prefer using similar equipment for repeatability, reliability, consistency and comparability. For me, using the Optos for retinal scans is also important so that the sequence of images are comparable, consistent and repeatable. Early detection is key. To do this effectively we need to minimise variables when comparing scans over time.
“I will often send my patients to meet the ophthalmologist before they reach the point where treatment is indicated. Building trust and rapport like this is an essential factor for long-term treatment success.
“I’ve found that patients who meet the ophthalmologist for the first time on the day of their treatment of anti-VEGF (vascular endothelial growth factor) injections or pan-retinal photocoagulation (PRP), can potentially find the experience too confronting. With little rapport built previously, these patients may be at risk of falling through the gaps of the health care system as they are too afraid to go back for further treatment.
“In addition to this, I follow-up with patients referred for treatment post their session. This is where we can talk through any concerns they have, and if there is concern that they will not continue with the treatment course despite further education around the first line treatment chosen, I can liaise with the ophthalmologist and discuss alternate treatment options that may increase the chances of patient compliance.”
Dr Howari said registering patients with KeepSight, Diabetes Australia’s free program that encourages and reminds people living with diabetes to have regular eye examinations, is also integral to the care she provides.
MAKING A DIFFERENCE
Now at 40 years of age, Dr Howari has lived with diabetes for 32 years.
“When you’ve had diabetes for over 10 years, especially type 1, there’s an 80% prognosis of developing diabetic retinopathy.
“The experience of living with diabetes and going through treatment for diabetic retinopathy, having had various treatments including PRP and anti-VEGF injections, has certainly highlighted the importance of compliance when it comes to regular optometric eye examinations, and ophthalmologist followups with regular retinal scans that can be shared and compared over time.
“My professional interest in diabetic eye disease and my personal lived experience have uniquely positioned me to have conversations with patients that delve deeper into diabetes, eye health and quality of life, which I hope will make a difference – not only to their long-term ocular health but also to their outlook on life and health as well.”

Dr Amira Howari supported the implementation of Diabetes Australia’s KeepSight program, which was initiated by ophthalmologist Professor Peter van Wijngaarden (left) and Greg Johnson from Diabetes Australia (right).





