Gaining expertise in the more complex areas of contact lens practice can be as rewarding for you as it is for your patients.
In my previous ‘mipatient’ column (mivision Jul 16), I described a little of the pathophysiology of a patient who developed neovascularisation in their corneal graft. In this column I will explore specialty contact lens management for a patient who displays longstanding corneal graft vascularisation.
Potential red flags to be aware of in keratoconus and specialty rigid contact lens fitting are:
- Corneal neovascularisation.
- Corneal graft rejection.1
- Corneal oedema.
- Khodadoust line – a line showing the border of corneal graft rejection and rejected corneal tissue.
- Corneal infiltrative events – corneal infiltrates, CLARE, marginal keratitis.
- Corneal toxicity reaction produced from a suboptimal fitting, suboptimal lens choice or inappropriate use of contact lens products.
- Exacerbating dry eye symptoms.
- Microbial keratitis.
Developing Your Expertise
Prescribing for keratoconus with limited prior expertise and education can be a concern due to the higher risk of inducing adverse, irreversible responses.
When well-prescribed, rigid gas permeable contact lenses pose minimal risk of corneal neovascularization
Suboptimal contact lens fitting can induce corneal scarring which potentially, can be further complicated by induced corneal neovascularisation. This can dramatically increase a patient’s future risk of corneal graft rejection.
For inexperienced prescribers, this means proceed with caution:
- Invest in quality education on specialty contact lens fitting – the School of Optometry at UNSW and ACO, and the Cornea and Contact Lens Society of Australia (CCLSA) run courses on advanced contact lens prescribing.
- Gain experience and familiarise yourself with the characteristics of a ‘good fit’ for a rigid contact lens by prescribing simpler cases, then apply those skills to a post graft situation.
- Consider co-managing with a specialty contact lens colleague until you develop the skills to handle difficult cases independently.
My Patient in the Chair
Back to my patient in the chair, forearmed with background information documented in my last column:
Occupation: Medical specialist in the field of pathology
Spectacle Refraction:
RE -15.75/- 4.00 x 143 6/30
LE -16.50/- 4.50 x 78 6/24 OU 6/18
Habitual vision with existing contact lenses:
RE (Unknown parameters) 6/9
LE (Unknown parameters) 6/15- OU 6/7.5 N8 to N12 (variable due to bubbles).
Patient Concerns
- Dissatisfied with vision and comfort of his last few contact lenses and perceived his current CLs to ‘have never been right since the beginning’.
- Reports the lens feels as if it ‘lifts off the cornea’ and after two to three hours, bubbles form behind the lens, interfering with vision. The lenses feel dry and uncomfortable; they must be taken off and have rewetting drops applied to the posterior surface to remove bubbles.
- Open to two different pairs of lenses, one for distance and a pair especially for microscopy.
- Would like to avoid wearing readers on top of contact lenses when reading.
Clinical Results
- RE quiet and happy, as with most cases of keratoconus, neither eye displays frank clinical signs of keratoconus on microscopy. (Refer Figure 1).
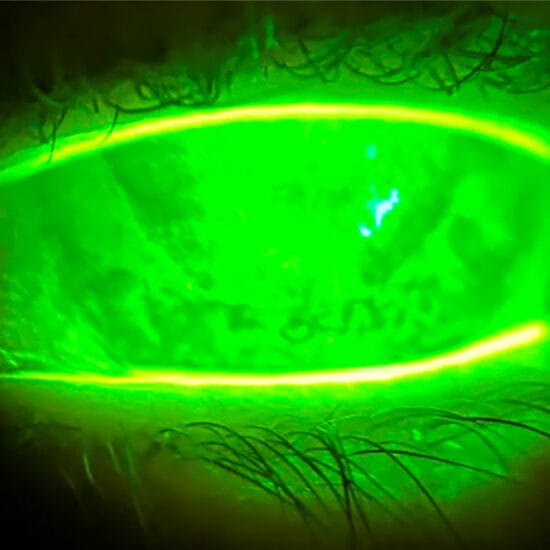
- Significant LE inferior corneal neovascularisation near full thickness.
- LE corneal full thickness transplant penetrating keratoplasty as per patient’s description in near rejection episode during 1986 (Refer Figures 2, 3).
- Lenses fitting too flat over the central cornea and over the graft/host corneal junction, with proud peripheral gaping edges over the host cornea. This is consistent with symptoms of how the air bubbles would track their way in over a few hours of wear to impair vision
(Refer Figures 4, 5). - A significant corneal graft/host junction height discrepancy on LE seen on Oculus corneal topography (Refer Figures 6, 7).
Risk Factors
When well-prescribed, rigid gas permeable contact lenses pose minimal risk of corneal neovascularisation. However, contact lenses with low oxygen permeability, or, as in the above example, contact lenses that cause biomechanical stress by chronic, heavy bearing of the lens over the corneal limbus, are at high risk of triggering corneal neovascularisation.2
Although nowadays, most contact lens practitioners use highly oxygen permeable fluoropolymers, the rigid contact lens in situ can sometimes be of a considerably high prescription. This may mean the lens is so thick that it delivers compromised levels of oxygen permeability.
My Strategy
- Prescribe a new contact lens with a centrally steeper fit, and better clearance over the graft/host junction interface.
- Explain the need for an optimal lens design with quadrant specific steeper inferior peripheral curves to fit more appropriately over patient’s cornea and eliminate bubble formation.
- Recommend an Intermediate Rx target in monovision power in CLs with the LE set for near (due to lower VA in this eye). Recommend the oculars for microscopy work are set to different focal powers to retain stereopsis. This will balance the need for clear stereoscopic vision and eliminate the need for over the top reading specs.
- Although beyond the scope of this article, a basic mental plan is to address the fit in this order: optimise the central base curve for corneal clearance, then the peripheral fitting to obtain the right amount of movement, then the lens diameter and Rx and finally, modify to correct for the presence of any significant OverRx on delivery.
First Lenses
- Custom RoseK2 Irregular Cornea Design prescribed in both eyes
- RE 6.8/11.20/-12.25 6/9
- LE 6.2/11.20/-18.50 6/12-1 OU 6/7.5
- Custom quadrant zoning for peripheral curves and incorporated asymmetric corneal technology tuck inferiorly
- Boston XO material RE clear, LE blue.
Patient Feedback
- Improved comfort and vision
- OverRx on delivery
- RE 0.00 6/12
- LE +0.50 6/15 OU 6/7.5 N4
- L lens still appeared to form bubbles at the junction and there was insufficient clearance of the graft host junction (refer Figures 8, 9). The lenses required further refinement.
Second Lenses
With the initial aim being intermediate Rx LE and monovision, lenses for fit and power were modified to:
- Custom RoseK2 Irregular Cornea Design
- RE 6.8/11.20/-12.25 6/9
- LE 6.0/11.20/-22.50 6/15 OU 6/7.5-2 N3.2
- Custom quadrant zoning for peripheral curves and increased asymmetric corneal technology tuck inferiorly.
- RE and LE CL NaFl images required nice central clearance RE, and nice graft/host junction and central clearance LE (refer Figures 10, 11).
Patient Feedback
- The slight VA reduction in distance allowed significant improvement in near vision and avoided the need to wear reading specs over the top.
- No bubbles forming beneath the lens, resulting in uninterrupted vision throughout the day.
- No comfort issues.
The Twist in the Plot line
Six months later, on his next follow up, I told my patient that I was recruiting live patients to help practitioners gain skills in the field of specialty contact lenses.
Rather ambitiously, I asked him to volunteer at a CCLSA event to teach Masters students in Advanced CLs at UNSW. I told him that as a volunteer, he’d have 140 practitioners poking, prodding and instilling sodium fluorescein into his eyes, so they could learn how to provide better patient care.
Then I told him Alan Saks would also be teaching this course. “I know Alan!,” he said. “He was my New Zealand optometrist who used to look after me as well as you are doing now… Sure, I’ll do it.”
With patient consent, Alan and I compared my records to his, which had been taken 16 years earlier, in pre-slit lamp imaging days (refer Figure 12).
The NaFl patterns are identical, I have managed to maintain the patient’s best correctible visual acuity and the neovascularisation hasn’t progressed any further. I have an incredible amount of respect for this third generation specialty contact lens optometrist, Alan Saks, and am proud to have learned a lot from him as one of my mentors.
But the moment your patient says he’s really struggled since relocating from Auckland, and that he’s finally found someone with expertise he’s happy with, it’s time to take yourself off the treadmill, at least for one moment, and be happy too.
Hard work always pays off.
Happy prescribing, folks.
Margaret Lam is an optometrist in theeyecarecompany practices in greater Sydney and Sydney CBD. Margaret practises full scope optometry, but with a passionate interest in contact lenses, retail aspects of optometry and successful patient communication and management. She has extensive experience in specialty contact lens fitting in corneal ectasia, keratoconus and orthokeratology, and is a past recipient of the Neville Fulthorpe Award for Clinical Excellence.
Margaret writes ‘mipatient’ on alternate months with Jessica Chi.
Footnote
In the first part of this column, comments from Dr. Doug Parker were included without him having the opportunity to review the final article. The author thanks him for his comments as a contribution to the previous mipatient column.