

The MS-39 AS-OCT combines placido disk corneal topography with high resolution anterior segment tomography to provide information on pachymetry, elevation, curvature and dioptric power of corneal surfaces.
With an available IOL calculation module and tools to perform accurate pupil diameter measurements and advanced tear film analysis, the MS-39 is also invaluable for refractive surgery planning. Cataract and refractive surgeon Dr Rick Wolfe writes about his clinical experience with the MS-39 AS-OCT.
In refractive surgery there are several ocular metrics we require. Perhaps most importantly, we want to exclude subclinical keratoconus (SCKCN) and we need to ensure there is no presence of ocular surface disease (OSD) – refractive surgeons spend a great deal of time assessing and treating this before surgery. The MS-39 ASOCT has made an enormous contribution to all of these ends.
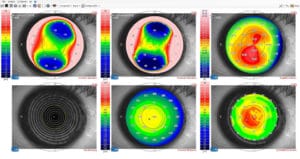
Figure 1. A hexamap refractive display of the right eye of a 36 year old refractive surgery applicant. Topography is normal showing no sign of keratoconus. The bottom right map shows epithelial thinning consistent with
keratoconus. The left eye has frank keratoconus.
The MS-39 AS-OCT is based on a spectral domain optical coherence tomographer (SD-OCT) and the Scheimpflug system that predated it. The option for spectral domain mode in the design, combined with a short wavelength of 845nm, provides the best possible axial precision of 3.6μm. Had swept source been incorporated into the design, it would have been less precise. A still or moving anterior segment OCT image can be generated, which covers 16mm.
FAST, SENSITIVE AND USER-FRIENDLY
The MS-39 AS-OCT provides all the usual corneal curvature and elevation values as well as pachymetric indices used in SCKCN detection.
Instead of using height data and converting this to curvature, as is the case with current tomographers, curvature is measured directly with placido images of both the anterior cornea (using 31,232 measured points) and the posterior cornea (using 25,600 measured points). This provides more sensitive curvature maps covering 10mm.
As opposed to most other devices, acquisition is brief and very easy to perform. All maps have common centration, and repeatability of most ocular metrics in health and keratoconus (KCN) is good.1,2
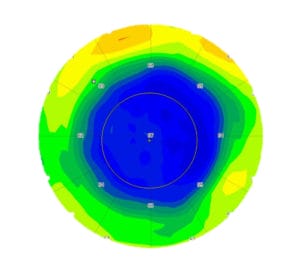
Figure 2. The left eye four months after -5.00D t-PRK. Regression to -0.50D with epithelium thickened to 67μm. t-PRK enhancement, if performed, would not even reach the stroma. Alcohol-assisted epithelial removal was able to be performed because the epithelial thickness was known.
EPITHELIAL MAPPING
The device can provide a corneal epithelial thickness map over the central 10mm of cornea.
Epithelial thinning with surrounding thickening has been linked to KCN histopathologically.3 Epithelial mapping has found the same pattern in KCN4,5 as well as SCKCN.6-9 It is logical, and seems likely, that the first sign of KCN is localised epithelial thinning over the cone apex, which is as yet, not visible on topography.
The epithelial map is helpful in two ways. In asymmetric bow tie, the absence of epithelial thinning at the proposed cone apex is evidence that SCKCN does not exist. This increases specificity. Similarly, localised epithelial thinning, in an otherwise normal cornea, might pick up SCKCN which is not detectable in any other way, increasing sensitivity (Figure 1). Epithelial thickening at a point of inferior steepening is consistent with corneal warpage and inconsistent with SCKCN.
Knowing the epithelial thickness is useful in transepithelial PRK (t-PRK), which has recently gained enormous popularity. While epithelial thickness centrally varies little (mean thickness 53.4 +/-4.6μm10), post LASIK or PRK there is an average 6μm increase in epithelial thickness.11 With the ability to estimate the likely epithelial thickness, this wouldn’t matter and the PRK enhancement could proceed. The problem is that in cases with regression, the epithelial hyperplasia can be significantly greater (Figure 2). It could be that with a small enhancement in such a case, there may be no or partial ablation of the stroma. Knowing the epithelial thickness is therefore helpful in t-PRK.
ARTIFICIAL INTELLIGENCE
Artificial intelligence (AI) is increasingly assisting medicine in general, and is particularly helpful in the detection of SCKCN in laser refractive surgery candidates. The MS-39 uses a Support Vector Machine (an AI method) to classify all topographies as normal, abnormal, suspect keratoconus or keratoconus. The sensitivity and specificity in detection of SCKCN from normal is 92% and 97.7% respectively.12
EXCEEDING EXPECTATIONS
The ability to quickly and simply measure non-invasive tear film break-up time (NITFBUT) using the MS-39 helps to detect and classify patients with ocular surface disease. This has significantly simplified the flow of patients to surgery or to treatment of the ocular surface before surgery.
There are several other features worthy of note:
Corneal aberrometry with point spread function, modulation transfer function and a convolved “E” helps the surgeon understand the quality of optics of the cornea.
Pupillography gives the size of the pupil under scotopic, mesopic and photopic conditions. There is also a glaucoma screening module and an intrastromal ring planning system.
The intraocular lens (IOL) calculation module works on the principle of ray tracing, and uses corneal, anterior chamber and lens position metrics. No IOL formula is used, just Snell’s law. It will be at its best in highly aberrated corneas. We are currently using it to calculate and compare the prediction error between it and traditional paraxial formulae.
As well as these features, OCT imaging of the anterior segments is possible. This ability provides further insights into refractive surgery.
If I were allowed only one instrument in refractive surgery, the MS-39 would exceed requirements.
Dr Rick Wolfe MB BS FRACS FRANZCO is one of Australia’s most experienced cataract and refractive surgeons. He has performed more than 30,000 cataract, RLE and LASIK procedures during the past 30 years while practising as an ophthalmic surgeon.
Dr Wolfe has provided more than 30 years’ service to the Royal Australian Navy Reserve, where he holds the rank of Lieutenant Commander. In 2004 he performed live surgery in front of 2,000 of his colleagues at the American Society of Cataract and Refractive Surgeons (ASCRS) in San Diego. Dr Wolfe regularly speaks at local and overseas conferences. His private practice, at Peninsula Eye Centre, Mornington, Victoria and at VISTAEyes Elsternwick Victoria, is limited to cataract and refractive surgery.
References
- Schiano-Lomoriello D, Bono V,Abicca I, Savini G Repeatability of anterior segment measurements by optical coherence tomography combined with placido disk corneal topography in eyes with Keratoconus Nature Scientific reports 2020 10:1124
- Vega Estrada A et. al Corneal Epithelial Thickness Intrasubject Repeatability and its Relation With Visual Limitation in Keratoconus Am J Ophthalmol 2019;200:255–262.
- Scroggs MW, Proia AD. Histopathological variation in kera- toconus. Cornea 1992;11(6):553–559.
- Reinstein DZ, Gobbe M, Archer TJ, Silverman RH, Coleman DJ. Epithelial, stromal, and total corneal thickness in keratoconus: three-dimensional display with Artemis very-high frequency digital ultrasound. J Refract Surg 2010;26(4):259–271.
- Reinstein DZ, Archer TJ, Gobbe M. Corneal epithelial thickness profile in the diagnosis of keratoconus. J Refract Surg 2009;25(7):604–610.
- Reinstein DZ, Archer TJ, Urs R, Gobbe M, Roy Choudhury A, Silverman RH. Detection of keratoconus in clinically and algorithmically topographically normal fellow eyes using epithelial thickness analysis. J Refract Surg 2015;31(11):736–744.
- Pircher N, Schwarzhans F, Holzer S, et al. Distinguishing keratoconic eyes and healthy eyes using ultrahighresolution optical coherence tomography–based corneal epithelium thickness mapping. Am J Ophthalmol 2018;189:47–54.
- Tang M, Li Y, Chamberlain W, Louie DJ, Schallhorn JM, Huang D. Differentiating keratoconus and corneal warpage by analyzing focal change patterns in corneal topography, pachymetry, and epithelial thickness maps. Invest Ophthalmol Vis Sci 2016;57(9):OCT544–OCT549.
- Li Y, Chamberlain W, Tan O, Brass R, Weiss JL, Huang D. Subclinical keratoconus detection by pattern analysis of corneal and epithelial thickness maps with optical coherence tomography. J Cataract Refract Surg 2016;42(2): 284–295.
- Reinstein DZ, Archer TJ, Gobbe M, et al. Epithelial thickness in the normal cornea: three-dimensional display with Artemis very high- frequency digital ultrasound. J Refract Surg. 2008;24:571–581
- Kanellopoulos AJ, Asimellis G. In vivo threedimensional corneal epithelium imaging in normal eyes by anterior-segment optical coherence tomography: a clinical reference study. Cornea. 2013;32:1493–1498.
- Arbalaez MC et. al. Use of a Support Vector Machine for Keratoconus and Subclinical Keratoconus Detection by Topographic and Tomographic Data Ophthalmology 2012;119:2231–2238





