

The COVID-19 pandemic has heightened awareness and stimulated discussion about the risks of infection during ocular consultations and surgeries.
A YouTube video released from Bristol Eye Hospital, suggesting aerosols produced during cataract surgery place surgical staff at risk of viral infection, prompted surgeons at Royal Victorian Eye and Ear Hospital to perform a study of their own. Their findings were reassuringly benign.
Cataract surgery is safe, accurate and highly successful.1 Unlike most surgeries involving the upper respiratory tract, it has not been considered to be an aerosol generating procedure (AGP)2 and therefore is not believed to place surgical staff at risk of contracting COVID-19 from infected patients.
A recent YouTube video produced by staff at Bristol Eye Hospital (youtube/8LGwI9LIYmU3), suggested that this may not be the case and that cataract surgery may, in fact, produce significant aerosols and therefore place surgical staff at risk of infection.
Our study clearly demonstrates that cataract surgery does not produce any significant particles…
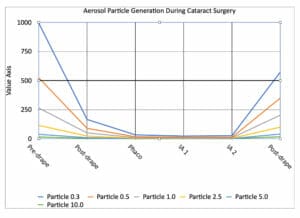
Figure 1. Lighthouse handheld particle counter, held 30cm from eye during cataract surgery.
Feature Image (Figure 2). Aerosol particles
measured during phases of routine cataract surgery.
Investigators who produced the video used a novel human cadaveric eye, the Alcon Centurion phacoemulsification system, and a 2.75mm wound and sleeve. They used high magnification and contrast cameras, which clearly demonstrate significant aerosol vapour extruding from the wound during phacoemulsification.
The recommendations from this study were to use:
- Pre-operative diluted povidone-iodine solution in the surgical field as this has been shown to be effective in eliminating the SARS-CoV and MERS-CoV viruses,
- Irrigation/aspiration for a minimum six seconds prior to starting active phacoemulsification,
- A N-(2-Hydroxypropyl)methacrylamide (HPMA) gel at the wound site, which clearly demonstrates a reduction in produced vapour, and
- Smaller wound sizes as the 2.75mm wound showed significantly more vapour than the 2.2mm wound.
While the above mentioned measures help reduce possible viral dissemination from the eye, anxiety remains over whether cataract surgery exposes staff to aerosols potentially contaminated with COVID-19.
To find out more, a small study at the Royal Victorian Eye and Ear Hospital (RVEEH) measured aerosols produced during routine cataract surgery to establish whether significant measurable amounts of aerosols were produced during phacoemulsification surgery.
METHOD
Ethics approval was granted for a lowrisk study by the Human Research Ethics Committee at the RVEEH. Aerosol generation was measured during 10 standard cataract surgeries, using a 2.4mm wound and sleeve and Alcon Centurion system. A 5% Povidone-iodine solution was placed in the fornix after speculum insertion, as per standard practice. Routine draping was performed and staff wore standard surgical personal protective equipment (standard face-masks).
Particle measurements were taken using the Lighthouse handheld 3016 1AQ particle counter during different stages of cataract surgery. The particle counter measures particle sizes of 0.3μm; 0,5μm; 1,0um; 2.5μm, 5,0um, and 10,0μm simultaneously.
The particle counter was calibrated before each case and held 30cm from the operated eye. One minute measurements were made during the following phases of cataract surgery: pre-drape, during phacoemulsification, during irrigation and aspiration, during viscoelastic removal and after the drape was removed.
Collected data was downloaded and analysed.
Particle Sizes
Viruses can potentially travel in all particle sizes. The bigger the particle, the more virus the particle may contain. The smaller the particle, the further it can travel/spread. Larger particles are considered to originate from the upper respiratory tract and are therefore most relevant to this study, although it should be assumed that all sized aerosol particles may contain virus.4
Results
All particle numbers decline to negligible readings during cataract surgery. Particles are generated by surgical staff and patient movements before and after surgery.
There is no demonstrated aerosol generation during any active stages of cataract surgery.
This was consistent throughout all 10 cases studied.
COVID-19 Surgical Precautions
A number of peri-operative precautions have been put in place across Australia to prevent COVID-19 spread in the elective surgery setting. These include:
- Alerting patients that they should not attend their surgery if they have symptoms suggestive of possible COVID-19 infection,
- Temperature and symptom testing of patients and staff on arrival at their surgical facility, and
- Implementing social distancing measures in waiting rooms and staggering admission times.
DISCUSSION
COVID-19 is a highly infectious and potentially lethal virus.5 The health and safety of medical staff and patients is paramount in performing any medical procedure. Cataract surgery has always been considered to be an extremely safe and effective surgery and has not previously been considered to be aerosol generating. Therefore, it has been perceived to be safe for surgical staff and patients.
The in vitro study conducted by Bristol Eye Hospital questioned that hypothesis. Declaring cataract surgery an aerosol generating procedure would have significant impact on the ability to continue to perform cataract surgery in the current format by increasing the costs of surgery and decreasing efficiencies in the cataract theatre.
Our study clearly demonstrates that cataract surgery does not produce any significant particles and therefore should not be considered an AGP.
Cataract surgery is an elective procedure in the vast majority of cases. It would be assumed that cataract surgery would occur in patients without any upper respiratory tract infection symptoms and therefore, would only occur in potentially asymptomatic or pre-symptomatic COVID-19 patients. The number of asymptomatic /pre-symptomatic patients with COVID-19 in the community is unknown. The viral load/ infectious status of these patients is also unknown, but is considered to be very low.6,7
CONCLUSION
Cataract surgery is not an aerosol generating procedure. Standard cataract surgery care should continue in its current form and no further precautions are required during surgery to protect staff and patients from disseminating/acquiring COVID-19 during surgery.
Perioperative COVID-19 precautions should continue to be practised until the crisis has resolved. Other perioperative precautions, such as pre-operative COVID-19 testing of all staff and patients, may be a necessary step in further insuring that staff are not infected, and that we are not conducting surgery on infected patients who may potentially spread COVID-19 in the perioperative setting.
Dr Anton van Heerden FRANZCO is a cataract and refractive surgeon. He is Head-of-Unit, Surgical Ophthalmology Services at the Royal Victorian Eye and Ear Hospital in Melbourne. He also consults at Armadale Eye Clinic, Mornington Peninsula Eye Clinic and Eye Laser Specialists.
Note: This study has not been peer-reviewed/ published in any scientific journal. The purpose of this article is to fast-track COVID-19 related information which may have public health implications relating to COVID-19 infection and ophthalmic surgery.
References
- Gogate et al: Safety and efficacy of Phacoemulsification Compared with Manual Small-Incision Cataract Surgery by Randomised Controlled Clinical Trial: Six Week Results. Ophthalmology; Vol 112, Issue 5, May 2005, Pages 869-874
- Aerosol generation from high speed ophthalmic instrumentation and the risk of contamination from COVID19. Kosher ZR, Dickie D: Eye (4 June 2020)
- youtu.be/8LGwI9LIYmU
- Verreault et al: Methods for Sampling of Airborne Viruses. Microbiology and Molecular Biology Reviews, Sept 2008, p. 413-444
- Baud et al: Real Estimates of Mortality Following COVID-19 infection. The Lancet: https://doi.org/10.1016/ S1473-3099(20)30195-X
- Bai et al: Presumed Asymptomatic Carrier Transmission of COVID-19. JAMA. 2020; 323(14):1406-1407
- Michael E: Is asymptomatic spread common in COVID-19?. Heal News, June 12, 2020, Source: WHO. COVID-19 Virtual Press conference, 8 June 2020.





