

Managing women living with diabetes presents particular challenges during pregnancy, delivery and in the ensuing months and years. Patient education, careful monitoring and co-management with the patient’s physicians is essential.
Diabetic retinopathy (DR) is the leading cause of visual impairment in people aged between 20 and 64-years-of-age, and pregnancy is a well-documented independent risk factor for progression.1 Management of diabetic retinopathy has changed dramatically over the last 10–20 years with the advancement of imaging modalities such as widefield photography, optical coherence tomography (OCT) and OCT angiogram (OCTA), as well as the use of intravitreal agents such as anti-vascular endothelial growth factors (anti-VEGF) and steroids. However, it continues to be a challenge, especially in the pregnancy cohort, due to a variety of reasons such as potential for rapid progression, treatment effects on foetus and numerous competing medical appointments.
Diabetes affects 9.9% of pregnancies in Australia

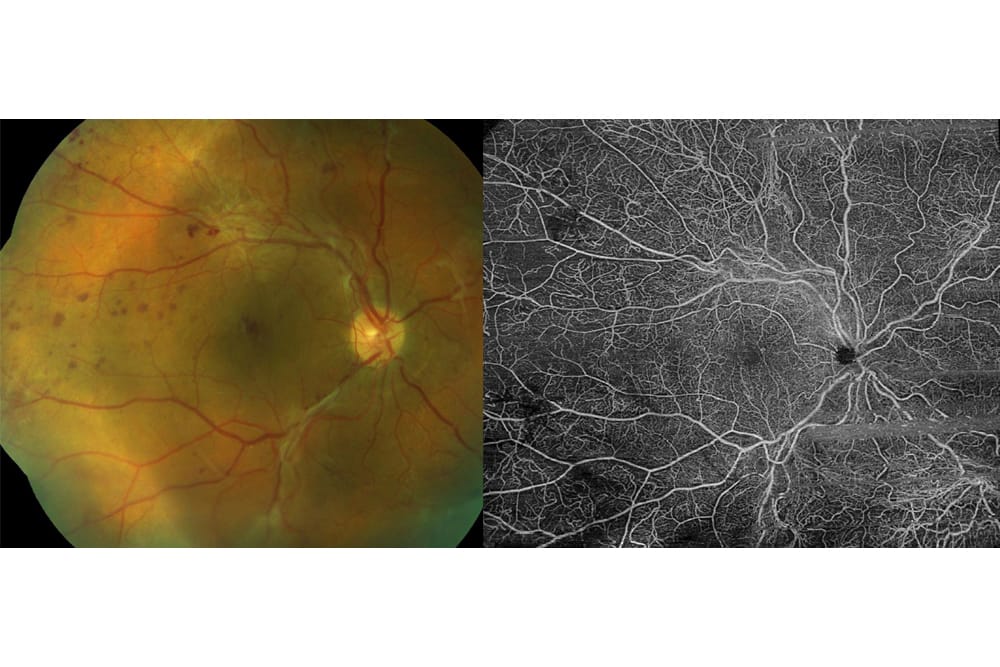
Figure 1. Severe pre-proliferative DR on fundus photo with widefield OCTA.
EPIDEMIOLOGY
Diabetes affects 9.9% of pregnancies in Australia. The vast majority are gestational diabetes (GDM) occurring in 8.9% of pregnancies, with 1% having pre-existing diabetes.2 This represents an approximate doubling of the prevalence over the past decade, where diabetes affected only 5.3% of pregnancies at the beginning of the last decade.3
GDM is a transient form of diabetes that occurs during pregnancy but resolves after giving birth. However, our understanding of the relationship between GDM and DR during pregnancy is incomplete. GDM patients are generally considered to be at minimal risk due to its transient nature. Unfortunately, a proportion of patients who are diagnosed with GDM may have undetected existing diabetes, and this subgroup are at risk of developing DR during pregnancy.
The prevalence of diabetes in pregnancy also varies significantly in different ethnicities. It is estimated that diabetes in pregnancy occurs most frequently in South East Asia, while the rate of pre-existing diabetes in pregnancy is highest in the Middle East and North Africa. It is also known that diabetes in pregnancy is 10 times higher in Aboriginal and Torres Strait Islanders compare to other Australian mothers.4
RISK FACTORS FOR PROGRESSION IN PREGNANCY
Pregnancy is an independent risk factor in the progression of DR and is estimated to progress at twice the rate when compared to non-pregnant women. There are other risk factors that accelerate the progression of diabetic retinopathy during pregnancies, including poor glycaemic control, duration of disease, severity of pre-existing DR and hypertension. These risk factors are similar to those of the general population with diabetes.
… patients with GDM are at higher risk of developing diabetes later on in life and… GDM is associated with increased ophthalmic co-morbidities including DR in the long term
Glycaemic Control
It is evident that poor glycaemic control before conception is a risk factor for DR progression in pregnancy. The relationship between glycaemic control and DR progression during pregnancy is a little more complex, where rapid tightening of glycaemic control during pregnancy has been demonstrated to worsen DR. This is because of the underlying retinal phsyiology – when it becomes accustomed to wasteful glycolysis in the setting of persistent hyperglycaemia, a sudden reduction of glucose will result in reduced blood flow, subsequent hypoxia and worsening of the DR. Therefore, it is optimal to have a gradual tightening of glycaemia control pre-conception to avoid the short-term risks of DR progression during pregnancy from intensive glycaemic tightening.
From a holistic perspective, physicians will always seek to maximise glycaemic control during pregnancy, and any patient having rapid tightening should have retinal examinations on a more regular basis.

Figure 2A. OCT showing macular oedema at 29 weeks; pregnant vision was 6/12 at this time. B. OCTA and macular OCT at 12 weeks after delivery.
Duration of Disease
Multiple studies have shown that the progression of DR in pregnancy is strongly correlated to the duration of diabetes, and so unsurprisingly, type 1 diabetes mellitus (T1DM) has a much higher prevalence of DR in pregnancy than type 2 (T2DM). This was demonstrated in a study regarding T1DM – patients whose DR remained stable in pregnancy had an average duration of disease of 13.5 years, while those whose DR progressed, had an average duration of 19.7 years. Duration also has a profound effect on progression to proliferative diabetic retinopathy (PDR), where 38% of patients with duration greater than 15 years developed PDR during pregnancy, compared to 15% of patients with duration less than 15 years. Consequently, some guidelines recommend women with diabetes plan and complete their pregnancies early in life if possible.
Pre-existing Diabetic Retinopathy
The degree of baseline diabetic retinopathy pre-conception is another risk factor for progression of DR in pregnancy. In the Diabetes in Early Pregnancy Study (DIEP), 21.1% of patients with mild nonproliferative diabetic retinopathy (NPDR) progressed during pregnancy and only 6% of these patients went on to develop PDR. Of patients with moderate to severe NPDR, 54.8% demonstrated disease progression and had a 29% risk for developing PDR.5
Other studies have shown rates of progression as high as 78%, with duration of diagnosis of diabetes proving the most significant factor.
Multiple studies have shown that the progression of DR in pregnancy is strongly correlated to the duration of diabetes
Hypertension
There is mixed evidence on hypertension and DR progression in pregnancy. One study found that hypertension, both chronic and pregnancy-induced, carries more than double the risk of DR progression in pregnancy (61% vs. 50% respectively) versus normotension (25%).
New-onset hypertension from after 20 weeks of gestation, with significant proteinuria, is known as pre-eclampsia. This pregnancy specific condition is a significant risk factor for DR progression in pregnancy. One study found 50% of women with pre-eclampsia developed sight threatening disease compared to 8% in those without pre-eclampsia.6
SCREENING AND MONITORING
Prenatal
Prenatal counselling and screening is, perhaps, the most effective method to minimise DR progression in pregnancy because it provides greater opportunities to intervene and address the modifiable risk factors prior to conception, such as gradual tightening of glycaemic control or treating existing DR. Unfortunately, less than a quarter of Australian women (27.8% in T1DM and 12% in T2DM) have had any general diabetic prenatal counselling.
Diabetic retinopathy screening is recommended in all patients with diabetes but is even more vital in those who are planning to become pregnant. Retinal examinations can be performed by dilated fundus slit lamp examination or nonmydriatic widefield fundus photographs. This allows for an accurate assessment of the DR severity that can provide prognosis on the risks of DR progression during pregnancy. Furthermore, treatment such as laser photocoagulation and anti-VEGF injections can be given if clinically indicated pre-conception, again to minimise risks of DR progression in pregnancy. Optimising diabetic control prior to pregnancy is the best option to prevent complications including diabetic retinopathy.
Antenatal
Retinal examination is recommended in the first trimester of pregnancy for those with diabetes. Guidelines also recommend retinal examination in the second and third trimester of pregnancy, depending on the severity of DR as well as the number and severity of risk factors of progression as discussed above. Fortunately, DR tends to regress in the third trimester of pregnancy but progression is at its worst at the end of the second trimester.
While diabetic macular oedema (DMO) and NPDR may improve following delivery, PDR does not regress and should be treated urgently to minimise further sight threatening complications.

Figure 3. Left fundus images, pre and post injection of ranibizumab.
Postpartum
It is known that patients with GDM are at higher risk of developing diabetes later on in life and there have also been longitudinal studies to show that GDM is associated with increased ophthalmic comorbidities including DR in the long term.7 It is therefore vital for these patients to follow-up closely with their family doctor to monitor for onset of diabetes, and if found, to follow the screening guidelines of biennial or yearly retinal examination to detect onset of DR. The increased risk of progression of diabetic retinopathy persists for six to 12 months following pregnancy and delivery, and increased optometric/ophthalmic review is recommended in this period.
INVESTIGATIONS AND TREATMENT
Fluorescein Angiogram
Traditionally, fundus fluorescein angiogram (FFA) is the ancillary test of choice for determining the severity, and planning treatment for DR. However, the safety profile of fluorescein is scarcely investigated and has been assigned a pregnancy category of B2 by the Therapeutic Goods Administration (TGA) in Australia. Category B2 refers to drugs which have been taken by a limited number of pregnant women, without demonstrating an increase in frequency of malformation or harmful effects on the foetus. Additionally, studies in animals, while inadequate, do not demonstrate an increased incidence of foetal damage. Due to the limited data available on its safety profile, FFA is not usually performed in pregnant women unless it is clearly indicated. Fortunately, the advancement of noninvasive imaging modalities such, as OCT and OCTA, have allowed clinicians to detect diabetic macular oedema (DMO), retinal ischaemia and neovascularisation, minimising the use of FFA in pregnancy.
Laser Photocoagulation
Laser photocoagulation can be used to treat different forms of DR, namely PDR or DMO. It is a safe and effective treatment modality, especially in those who are pregnant as it does not affect or damage the foetus, and has been shown to reduce significant visual loss from DR.
Pan retinal laser photocoagulation (PRP) is used to treat PDR or severe NPDR. Generally it is recommended to have a lower threshold to treat pregnant women with PDR or severe NPDR for several reasons. These include the increased risks of DR progression during pregnancy, logistical difficulties of attending multiple healthcare appointments during pregnancy, and evidence of progression post-partum.
Focal laser photocoagulation can also be used to treat DMO. However, the American Academy of Ophthalmology (AAO) suggests that treatment can be deferred during pregnancy due to its relatively short duration, the potential for DMO to regress post-partum, and relatively little difference in the long-term outcomes in prompt versus deferred treatment in DMO. When treatment is necessary for centre involving severe DMO, intravitreal steroids are often preferred.
Intravitreal Injections (Anti-VEGF/Steroids)
Intravitreal injections (IVI) are another effective treatment for DR in general. However, unlike laser photocoagulation, IVI does have systemic absorption and its safety profiles are not well studied for those who are pregnant. For example, although anti-VEGF agents have transformed the way we manage DR, the TGA assigned it a pregnancy Category D due to its mechanism of action. Category D drugs are suspected to have an increased incidence of foetal damage or malformations. It is therefore recommended that patients wait at least three months after administration of anti-VEGF before conceiving. Similarly, women of child bearing age who are receiving anti-VEGF treatment are advised to use contraception to mitigate the risks of teratogenicity.

Figure 4A. Macular oedema with vision reduced to 6/24. B. Three weeks following intravitreal injection, the patient’s vision was 6/9.
Although there have been case series demonstrating uneventful pregnancies following administration of antenatal intravitreal anti-VEGF, it is still not recommended to administer these agents unless there are clear benefits that outweigh the potential risks to the foetus, and extensive counselling and consent is required if proceeding with anti-VEGF administration. If administration is deemed necessary, the risk of teratogenicity is thought to be lowest in the third trimester. Sometimes, obstetricians can be consulted to bring forward the delivery to allow safe administration of these agents.
Intravitreal steroid injection (triamcinalone) may be an option in sight threatening severe DMO, but again, treatment can often be deferred until delivery.
Deferring treatment of DMO by 12 months has not been shown to alter the longterm visual outcomes, and it is therefore reasonable to withhold anti-VEGF/steroid treatment for a duration of six to nine months during pregnancy.
CASE ONE
A 23-year-old Type 1 diabetic patient was referred at 28 weeks pregnancy for review. She had been diagnosed with diabetes 14 years prior with brittle control in youth. At 29 weeks gestation, her vision was 6/12. Twelve weeks after delivery, her ischemic changes and macular oedema had improved and the patient’s vision had returned to 6/9 (Figure 1).
CASE TWO
A 30-year-old woman presented with severe pre-proliferative DR in both eyes with vision threatening macular oedema. She was counselled on treatment options, and returned for treatment later in pregnancy, in the seventh month. She had bilateral intravitreal ranibizumab (Lucentis) (Figure 2).
CONCLUSION
Management of pregnant women with diabetes requires a team approach. Close cooperation and communication among the patient and her obstetrician, ophthalmologist, and other physicians, as necessary, is essential to develop an individual management plan for optimal outcomes.
Diabetes during pregnancy is becoming more common, due to obesity, increasing gestational age, and the younger age of onset of T2DM in the population.
Ideally, women with diabetes should be examined comprehensively, including a dilated fundus exam prior to conception. Otherwise this exam should occur as soon as possible in the first trimester. Follow up then depends on the severity of retinopathy. For example, if the patient has minimal or no DR she may be able to be examined approximately every three months and within three months postpartum. If the patient has moderate DR, examination every four to six weeks may be required and referral to an ophthalmologist is recommended; if more advanced DR is noted, the patient may require examination every one to two weeks, with intervention as needed. Continued monitoring and management postpartum is also important.
Severe NPDR or PDR should be treated immediately with scatter pan retinal photocoagulation. Treatment recommendations for DME during pregnancy are lacking, postponing treatment and observing closely can be justified as disease may regress postpartum, but some cases may need macular laser.
Further research in the field will focus on the use of non-invasive OCTA imaging to further aid diagnosis and prognostication of sight threatening complications for DR in pregnancy.
Dr Rahul Dubey MBBS (Hons), MMed (Clin Epi), MM (OphthSci), FRANZCO is a cataract, medical and surgical retinal specialist. He is a consultant Vitreoretinal Surgeon at Westmead and the Prince of Wales Hospital in Sydney and privately in Chatswood and the PersonalEyes network. Dr Dubey maintains a commitment to rural and regional ophthalmology in Dubbo and Bourke with the Outback Eye Service, supported by the Fred Hollows Foundation. Dr Dubey has published extensively in peer-reviewed medical literature and is passionate about training the next generation of optometrists and ophthalmologists.
Dr Christopher Go undertook his medical training at University of New South Wales and ophthalmology training in the Sydney Eye Hospital Network. He is currently the senior ophthalmology registrar at Westmead Hospital and is planning to undertake his surgical retina fellowship overseas in Taiwan next year. He is a clinical associate lecture at University of Sydney.
Photos provided courtesy of Professor Paul Mitchell.
References
- Hartnett ME, Baehr W, Le YZ. Diabetic retinopathy, an overview. Vision research. 2017;139:1-6.
- Australian Institute of Health and Welfare. Diabetes in pregnancy 2014–2015. Bulletin no 146 Cat no CDK 7 Canberra: AIHW. 2019.
- Australian Institute of Health and Welfare. Diabetes in pregnancy: its impact on Australian women and their babies. Diabetes series no 14 Cat no CVD 52 Canberra: AIHW. 2010.
- Morrison JL, Hodgson LA, Lim LL, Al-Qureshi S. Diabetic retinopathy in pregnancy: a review. Clinical & experimental ophthalmology. 2016;44(4):321-34.
- Chew EY, Mills JL, Metzger BE, Remaley NA, Jovanovic- Peterson L, Knopp RH, et al. Metabolic control and progression of retinopathy: The Diabetes in Early Pregnancy Study. Diabetes care. 1995;18(5):631-7.
- Lövestam-Adrian M, Agardh CD, Åberg A, Agardh E. Pre-eclampsia is a potent risk factor for deterioration of retinopathy during pregnancy in type 1 diabetic patients. Diabetic Medicine. 1997;14(12):1059-65.
- Auger N, Fraser WD, Paradis G, Healy-Profitós J, Hsieh A, Rhéaume M-A. Preeclampsia and long-term risk of maternal retinal disorders. Obstetrics & Gynecology. 2017;129(1):42-9.





