

Dry amniotic membrane therapy can be a powerful way to treat the ocular surface in cases of significant pathophysiological compromise, as this case study demonstrates.
In my last mivision column, I discussed dry amniotic membrane therapy, which is becoming increasingly available to Australian eye care professionals. Additionally in the same article, Dr Art Epstein shared practical guidelines for prescribing amniotic membrane to treat anterior eye pathophysiology conditions.
Amniotic membranes can be a powerful medium for improving ocular surface health

Figure 1. John’s left eye on his first consultation at our practice.
Amniotic membranes can be a powerful medium for improving ocular surface health where there has been pathological compromise. Interestingly, they work in several key ways.
Firstly, an amniotic membrane works as a mechanical barrier, shielding the underlying epithelium from the friction of eyelid interactions, and promoting corneal epithelial growth, differentiation, migration and adhesion.
Secondly, an amniotic membrane resembles corneal and conjunctival basement membrane, acting as a scaffold for epithelial growth. These properties can also prevent cellular apoptosis while the corneal cells are attempting to re-epithelialise.

Figure 2. John’s left corneal fluorescein staining on first consultation at our practice.
Thirdly, amniotic membranes have antiinflammatory and anti-fibrotic properties. Our corneal fibroblast cells, the corneal keratocytes, have a highly specialised role in maintaining corneal transparency. When dormant, these corneal keratocytes maintain corneal transparency, and when active, they form corneal scarring and loss of transparency in the cornea. These anti-fibrotic properties inhibit proliferation and differentiation of corneal, limbal and conjunctival fibroblasts, which in turn inhibits subsequent corneal scarring in an instance of corneal trauma or infection. There is evidence that amniotic membrane therapy helps induce apoptosis of inflammatory cells, and in the expression of corneal growth factors, supports corneal healing.

Figure 3. Appearance of the AmnioTek-C amniotic membrane in place – note the appearance of folds of the amniotic membrane under the contact lens on the corneal surface (on immediate application). It is important to ensure the amniotic membrane makes good contact with any particular corneal area of
concern, i.e. areas with more corneal trauma.
Lastly, amniotic membranes have antimicrobial properties as well as antiangiogenic properties that inhibit blood vessel growth. At the site of the eye, the cornea shows non-immunogenic characteristics, as do amniotic membranes, and this minimises the risk of ocular tissue rejection when using amniotic membrane therapy. Consequently, no immunosuppressive agents, such as topical steroids, are required when prescribing this therapy in a ‘dry’ form with a bandage contact lens.
CASE STUDY OF A CONCRETER
John,* a 47-year-old concreter, was referred to me for a bandage contact lens and my view as to whether there was any way to improve his vision.
Unfortunately, during a workplace accident four years prior, John’s left eye had been forcibly blasted with a very strong alkaline concrete cleaning reagent, combined with a slurry of concrete particles and highly caustic alkaline mixture.
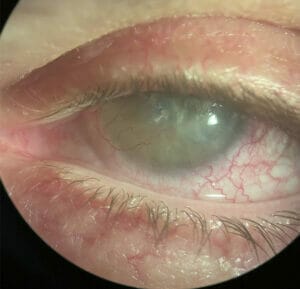
Figure 4. John’s left eye on day three of amniotic membrane therapy. Note the amniotic membrane has largely dissolved and folds are no longer visible.
Because he worked alone on the job site, without adequate and immediate first aid, there was a long delay in obtaining appropriate treatment. This allowed the alkaline burn to extensively damage his cornea.
The damage was compounded due to uncertainty, at the local medical clinic, as to how to manage the condition. Eventually he was referred to the corneal ophthalmologist at the local eye hospital for surgery, removing the many suspended foreign bodies and profusely irrigating his left eye with saline to dilute and flush out the alkaline reagent.
The Consultation
John’s entering visual acuity (VA) was R 6/9 (refractively corrected to 6/6), and L 6/120 (Figure 1).

Figure 5. John’s left corneal fluorescein staining, post amniotic membrane therapy.
John’s regimen for managing symptoms at the time of presentation was one drop of Bion tears, about every hour in his left eye, to soothe symptoms of irritation, and prednisolone, twice to three times a day, as required in his left eye, for persistent irritation.
Corneal staining showed extensive irregular remodelling on the corneal surface and corneal scarring, as shown in slit lamp photos (Figure 2).
I advised John to switch from Bion tears to Hyloforte as needed.
I then discussed amniotic membrane therapy as an option, and described the procedure. When John opted to go ahead, I applied for the Special Access Scheme via email.

Figure 6. John’s left eye before and after Amniotek-C amniotic membrane therapy.
Approval was granted in just two days, and we proceeded with the therapy.
Results
Following amniotic membrane therapy, John was able to discontinue prednisolone completely as the symptoms of eye irritation were greatly reduced.
Instead of using Bion tears hourly, he was able to use Hyloforte once or twice a day to manage irritation.
John’s VA improved from L 6/120 to L 6/30.

Figure 7. John’s difference in blood vessel calibre and corneal vascularisation reduction before and after amniotic membrane therapy – note a reduction in vessel calibre and visible corneal vascularisation, demonstrating antiangiogenic properties of amniotic membrane therapy.
Once fitted with a specialty semi-scleral RoseK2 XL contact lens, his VA further improved to L 6/21.
Having undergone amniotic membrane therapy, John’s corneal staining significantly reduced (Figure 5) as did corneal opacification and corneal vascularisation (Figure 7). Corneal transparency significantly increased (Figure 8).
AN IMPRESSIVE THERAPY
Recent changes to legislation mean that optometrists and ophthalmologists with appropriate training can now prescribe and perform amniotic membrane therapy.
While still in its very early days, extensive reports and feedback from our American and international colleagues who have decades of experience, demonstrate excellent patient outcomes in prescribing dry amniotic membrane therapy.

Figure 8. John’s difference in corneal keratocytes and corneal stromal scarring and opacification. Note a significant increase in corneal transparency, demonstrating anti-fibrotic properties of amniotic membrane therapy.
Interested optometry and ophthalmology practitioners can contact the Cornea and Contact Lens Society of Australia (www. cclsa.org.au) for resources and a step-by- step approach on how to apply for, and gain access to, this therapy under the Therapeutic Goods Administration’s Special Access Scheme.
*Patient name changed for anonymity.
Dr Margaret Lam is the National President of the Cornea and Contact Lens Society of Australia, a National Director of Optometry Australia and a Director of Optometry NSW/ACT. She teaches at the School of Optometry at UNSW as an Adjunct Senior Lecturer and works as the Head of Optometry Services for George and Matilda Eyecare.





