
History will guide us when we listen. Phakic intraocular lenses (pIOL) have been used to treat refractive error for decades – well before lasers were even invented. Now gaining in popularity, pIOLs are understood, by surgeons and patients alike, to be a safe additive and reversible refractive correction procedure.
In 1953, Strampelli implanted the first anterior chamber (AC) pIOL to correct myopia. This was a negative powered polymethylmethacrylate (PMMA) lens that worked to correct myopia, however the lens design and material in the AC resulted in many complications, including endothelial cell failure, pupil ovalisation and angle fibrosis. Additionally, inappropriate lens size caused the lens to rub and damage angle structures, with consequent glaucoma(Figure 1).1
Laser refractive surgery is fast, safe and predictable for the right patient, but it does have intrinsic limitations

Figure 1. Strampellis’ first phakic lens (Barraquer Institute).
Theodore Maiman invented the world’s first laser in 1960 – the ‘Ruby Laser’ (Figure 2), but it was not until the 1980s that laser energy was used to correct myopia with corneal reshaping.
As we go further in this article and look at modern phakic lens implants, it will become evident that lens design features contributing to safety and success can all be traced back to the early observations with the Strampelli lens.
MYOPIA TREATMENT
Myopia is not going away. Acupoint (Figure 3) treatment was unsuccessful as a traditional medicinal intervention designed to reduce the progression of myopia in teenage children, and it is now estimated that there will be five billion myopes in the world by 2050 – half the world’s population.2

Figure 2. Components of the first ruby laser.
Three surgical approaches can permanently correct myopia;
- Refractive lens exchange,
- Laser corneal reshaping, and
- Phakic lens implants.
Refractive lens exchange offers a permanent solution but, as an intraocular procedure, is associated with loss of accommodation and increased risk of retinal detachment in this myopic population.3

Figure 3. Acupoints for eye exercises.
Laser corneal surgery is very effective as a correction for myopia and, with current technology including lenticule extraction (SMILE), 87% of patients will get correction within 0.5D of the intended outcome.4 Laser refractive surgery is fast, safe and predictable for the right patient, but it does have intrinsic limitations. The cornea is irreversibly weakened; the ocular surface disrupted with exacerbation of ocular surface disease and dry eye problems; the correction of refractive error is associated with an increase in higher order aberrations – particularly spherical aberration; and the mechanical components of the procedure – whether the flap in LASIK or the lenticule cut and removal in SMILE – have their own potential problems with loss of corneal clarity. Certainly there are limits to how much refractive error can be corrected with corneal laser reshaping, and this range of treatability has become narrower over the 25 years of LASIK as we better understand the impacts of our treatments on visual quality and corneal stability.

Figure 4. Nuvita angle supported pIOL (Bausch and Lomb), (Versace).
We now know that laser corneal refractive correction may not be suitable for patients with:
- Myopia greater than 8D,
- Hyperopia greater than 5D,
- Irregular astigmatism,
- Asymmetry across the cornea suggesting forme fruste kerataconus,
- Thin corneas, where the central pachymetry is less than 500μm (PRK may be acceptable for corneas as thin as 450μm), of more importance is the residual corneal thickness when treatment is complete,
- Ocular surface disease that is unresponsive to treatment, and
- Corneal pathology such as anterior basement membrane disease.
With our knowledge of the above, laser vision correction is an extremely successful procedure, with more than 40 million people having successfully undergone it since its introduction in the late 1980s. Patient satisfaction is high, with at least 98% of patients reporting being satisfied.5,6

Figure 5. Cache showing footplate compression.
PHAKIC LENS IMPLANTATION
Phakic lens implantation, as an alternate to laser corneal reshaping, offers a solution to each of the above contraindications to laser. The phakic lens is additive surgery; it does not weaken the eye; can treat a wide range of refractive correction (as the surgery is no different for -1D or -18D); there is minimal impact on the ocular surface; and, as the cornea is not weakened by phakic lens implant, there is minimal risk with thin corneas or corneal asymmetry suggestive of forme fruste kerataconus.

Figure 6. Iris clip lenses.
Patients quickly appreciate the reversibility and fast healing of the phakic lens as an alternative to laser and, while the phakic lens was originally used as a plan B for when laser was not possible, it is now common for patients to choose this as their preference for surgery.
Compared with laser corneal refractive correction, pIOLs offer several benefits:
- They offer a larger effective optic zone, achieved because the lens sits closer to the pupil,
- The crystalline lens’ natural accommodation is preserved,
- Image quality is enhanced as spherical aberration is reduced with pIOL correction rather than the typical two times increase with LASIK,7
- Refractive predictability is excellent as the refractive result is not dependent upon wound healing and is independent of the degree of correction,
- Being reversible; the lens can be removed, restoring the eye to its original state, and
- Complex and expensive lasers are not required for this vision correction surgery.

Figure 7. Pupillary lens, BJO 1962.
Phakic IOLs
Phakic IOLs are supplementary lenses implanted between the cornea and crystalline lens. They can be categorised as AC angle supported, AC iris supported, or posterior chamber.
Each category has different benefits and downsides with specific applications.
AC Angle Supported

Figure 8. The sputnik IOL, which is a form of iris clip lens, (Versace).
These were the first pIOLs to be used with Strampelli implanting them in 1953 and Barraquer reporting on more than 200 implants in 1959.8 Many of these earlier rigid acrylic lenses were explanted due to complications of endothelial cell damage, pupil cicatrisation with ovalisation, inflammatory peripheral anterior synechiae, and uveitis-glaucoma-hyphema syndrome.
Advances in materials and lens design saw several PMMA AC angle supported lenses come and go through the 1980s and 1990s (Figure 4). These lenses shared the same complications of the earliest design, with unacceptable damage to endothelial cells, pupil ovalisation and chronic anterior uveitis resulting in their withdrawal from the market.
Foldable Designs
Rigid materials and poor haptic design were the common themes associated with the complications of AC angle supported pIOLs. The development of foldable acrylics and a softer, more flexible haptic design, saw the introduction of foldable AC angle supported pIOLs, such as Alcons’ Acrysof Cachet. The Cachet was made from Alcons’ Acrysof foldable acrylic material with soft and deformable haptics. Foldable lenses allowed insertion through smaller wounds, allowing for more controlled surgery and better control of astigmatism. Coming in four different lengths, the lens size could be optimised based on the patient’s white-to-white measurements. Deformable footplates compensated for compression, allowing the optic to remain in a stable and predictable position in the AC over a range of chamber dimensions. Material and design improvement held the promise of an AC angle supported pIOL, that would avoid previous pitfalls. The Cachet lens was easy to implant and gave excellent visual results (Figure 5).

Figure 9. Active Dutch man (Pulp Librarian@ PulpLibrarian).
Unfortunately by 2014, five years after its introduction, the lens was withdrawn from the market because of the high rate of endothelial cell loss documented in analysis of the ongoing clinical trial. The TGA issued a second warning notice, advising that up to 3% of patients were requiring explantation for progressive decline in endothelial cell density.9 Many patients continue to have good spectacle free vision with Cachet lenses in their eyes, though some exhibit pupil ovalisation and peripheral synechiae around the lens footplate.
The overall challenge with angle supported pIOLs is physical. A small size lens may be loose enough to move and damage the endothelium or rotate, making toric correction difficult. A larger lens will be stable, but will put excess pressure on the angle, leading to pupil ovalisation and synechiae. Similar problems have plagued AC IOLs and it may be that this is just not a safe place for a lens in the eye.
Iris Fixation Iris fixation of an AC pIOL avoids the pitfalls of angle fixation. The concept of attaching an IOL to the iris dates back to the 1950s when an earlier form of aphakia correction after cataract surgery was the Binkhorst ‘Iris Clip’ lens. (Figures 6 and 7). The lens had two wire loops at the edge of the optic, allowing one loop to sit anterior to the pupil margin and the other behind it, similar to a paper clip. This approach, of iris clip at the pupil margin, fell from use over the following decades due to complications.10,11 These included:
- Corneal decompensation due to endothelial cell damage,
- Lens dislocation; miotics were used to control the pupil size, though in many patients, translucent pupillary membranes formed, preventing pupil dilation (Figure 8), and
- Inflammation with lens precipitates and glaucoma.

Figure 10. Iris Claw pIOL (Versace).
Iris support was better achieved using a claw design so that the lens was attached to the anterior surface of the mid peripheral iris stroma. In 1978, Worst (the Dutch were very active in this era of lens development) designed the iris claw single piece PMMA lens that was enclevated in a fold of midperipheral iris stroma using two ‘claws’ (Figure 9). In 1980, an opaque iris claw lens was first used in a phakic patient to suppress diplopia. This showed the lens to be safe in the phakic eye and in 1986, Worst and Fechner designed a biconcave iris claw lens for the treatment of high myopia. Fechners’ earliest cases were complicated by iritis but modification of the surgical technique and use of steroids resolved this problem.12 Refractive predictability was excellent and today’s iris claw phakic IOLs continue to use the same design with subtle changes (Figure 10). The main ongoing concern with iris claw pIOLs is progressive loss of endothelial cell density.

Figure 11. Traumatic dislocation of Artisan pIOL (Versace).
AC Iris Supported Lenses
AC iris supported lenses are currently available as the Artisan (Ophtec BV) – a rigid/non-foldable PMMA lens used for the treatment of aphakia as well as phakic refractive error, and the Artiflex (Ophtec BV) a foldable acrylic lens used as a pIOL. The rigid lens can treat myopia, hyperopia and astigmatism, coming in a range of powers from -3.0 to -23.5D, though the larger optic lens (6.0mm) is limited to -15.5D as the thick lens edge puts it into closer proximity with the corneal endothelium. Hyperopic powers range from +1.0 to +12.0D and astigmatism up to 7.0D cylinder. All lenses have the same overall dimension of 8.5mm, which means there are no issues with lens sizing.
The foldable Artiflex lens treats myopia and astigmatism and has the benefit of being implantable through a smaller incision – giving faster healing and better control of astigmatism.

Table 1. Minimum endothelial cell density required for implantation of Artisan pIOL.
Iris claw pIOLs are typically used in higher myopes who may not be suitable for laser vision correction. AC depth is critical to minimise damage to the corneal endothelium. Myopic cases require 3.5mm from the epithelium and hyperopic cases 2.8mm (the hyperopic lens is thicker centrally, where the AC is deeper). Specular microscopy is used to confirm an endothelial cell count of at least 2,500 cells/mm2 (or 3,500 for younger patients). To avoid pupillary block, an iridotomy is created pre-surgery with laser, or surgically at the time of surgery. A large (6mm) scleral tunnel incision is created and the lens placed into the AC with the pupil constricted. Two vertical paracentesis are used for enclevation of the lens – a small knuckle of iris is drawn into the lens claw. Toric lenses are aligned at the correct axis prior to attachment to the iris. The wound is sutured closed. Implantation of the foldable lens is similar, though the smaller wound requires only one suture.
The main advantages of AC iris claw lenses are that one size fits all eyes and they come in a wide range of powers. The disadvantages include:
- Surgery can be complex,
- Necessitates a large wound requiring sutures,
- Iris enclevation can be imprecise for achieving perfect centration and toric alignment,
- Lenses can de-enclevate, presenting an anterior segment emergency (Figure 11),
- Ongoing loss of endothelial cells,
- Low grade inflammation, and
- Difficult surgery when the patient comes to cataract operation.
Endothelial Health

Figure 13. Phakic IOL/ IPCL (Praveen Subudhi et al 2020).
Endothelial health remains an area of concern with iris supported lenses. Specular microscopy should be done annually to detect patients who may require lens explant to avoid corneal decompensation. Jonker et al carefully studied the endothelial cell density over 10 years for patients implanted with the Artisan iris supported pIOL.13 This paper highlighted the risk of projected long-term corneal problems, with 50% of lenses potentially coming to explant due to endothelial cell damage at 15 years (based on the American Academy of Ophthalmology guide of 25% decline in endothelial cell density or the French approach of a cell count of < 1,500 cells/mm2). Chronic endothelial cell loss between six months and 10 years after surgery was 21.5% for the toric myopic Artisan lens patients, and 6% of lenses had been explanted by 10 years due to reduced endothelial cell density.

Figure 14. Visian implantable collamer lens – EVO with central port (Staar).
The main risk factor for endothelial cell damage was reduced clearance between the lens edges and the corneal endothelium. There is a direct correlation between AC depth and the rate of endothelial cell density decline. With this in mind, the safety recommendations for Artisan pIOL are:
- Minimum AC depth of 3.2 or 3.5mm,
- Sufficient calculated distance between the pIOL and corneal endothelium of 1.5mm,
- No eye rubbing, and
- Age consideration both for changing AC depth (lens clearance will get less with age) and required minimum endothelial cell density.
The complications and downsides associated with AC iris supported lenses led to the development and widespread adoption of posterior chamber pIOLs. Posterior chamber lenses have the advantages of being optically superior, easier to implant, and further from the cornea and endothelium. Their position behind the iris, however, has associated increased risk of cataract formation, disturbance of aqueous flow with possible glaucoma, and more critical lens sizing. Lens designs have continued to evolve since Fyodorovs’ first posterior chamber pIOL in 1986, resulting in the most commonly used phakic lens today – the Visian implantable collamer lens (ICL) that we will discuss in more detail later.

Figure 15. Attempted vision achieved manifest SE five years after ICL implant (Kimiya Shimizu, MD, PhD, Kazutaka Kamiya, MD, PhD, Akihito Igarashi, MD, PhD, and Hidenaga Kobashi, MD, PhD).
Posterior Chamber pIOLs
Posterior chamber pIOLs are designed to sit in front of the crystalline lens, where they are supported in the ciliary sulcus. An aqueous filled space separates the pIOL from the anterior lens capsule. An alternate approach was tried over two decades in the form of the Phakic Refractive Lens (PRL; Carl Zeiss, Jena, Germany). This pIOL was designed to sit anterior to the crystalline lens, floating on a sea of aqueous and with no contact with the ciliary sulcus (Figure 12). As a free floating lens, it was too unstable to treat astigmatism and, in practise, it often rubbed against the ciliary sulcus.14 The lens was withdrawn from the market in 2012 due to unacceptable complications, including cases of the lens dislocating through the ciliary zonules into the vitreous cavity.15
Two posterior chamber pIOLs are available today:
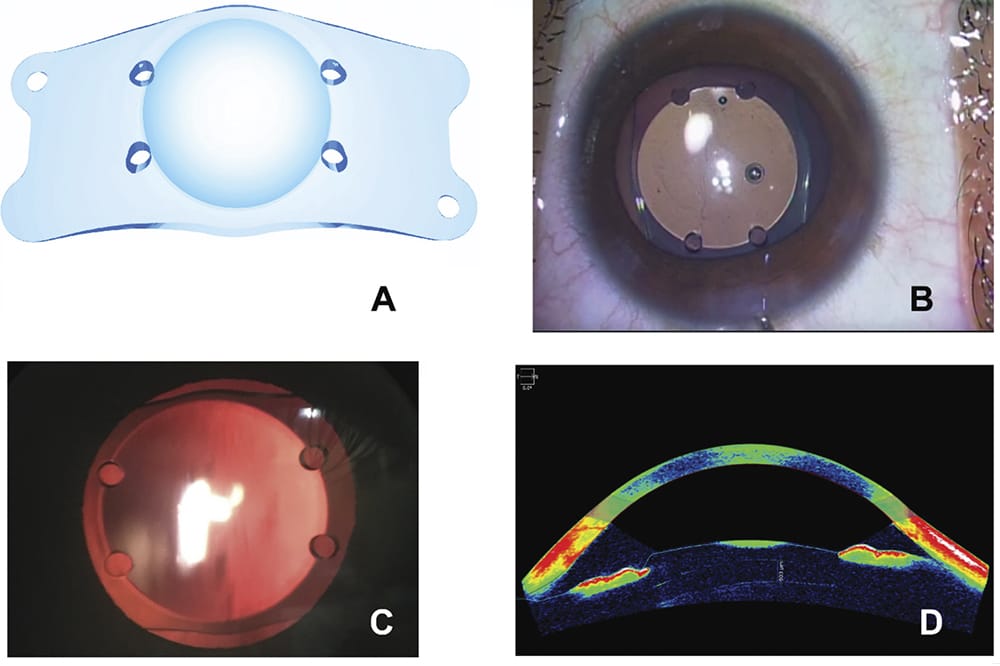
- The Implantable phakic lens (IPCL – Care Group, India), which is a newer lens developed as a cheaper alternative to the ICL. It is now available with a central port design and also as a trifocal diffractive presbyopia correcting pIOL (Figure 13). The IPCL comes in a wider range of refractive powers as compared with the ICL, treating up to -30 and + 15D. The IPCL is not yet available in Australia, however Therapeutic Goods Administration registration is pending.
- The Visian implantable collamer lens (ICL – Staar Surgical) is currently the most widely used pIOL with more than one million procedures performed worldwide (Figure 14). First implanted in 1993, the lens has seen several iterations and in its current form can correct myopia up to -18D, hyperopia up to +6D and 4D of astigmatism.

Figure 16. Anterior capsular cataract with ICL in situ (Versace).
The ICL is made of a collamer material (0.2% collagen, 60% hydroxyethylmethacrylate copolymer and water), which is unique in that the added collagen attracts the deposition of a layer of fibrinectin onto the lens surface. This inhibits protein binding, hides the lens from the immune system and enhances its biocompatibility.
Surgery is done under topical anaesthesia through a 2.8mm wound, with the lens implanted and positioned behind the iris to sit in the ciliary sulcus. The lens comes in a range of sizes to ensure a clear space between the implanted lens and the anterior lens capsule can be achieved. An AC depth of 2.8mm (from the endothelium) is required with a normal iris configuration. The hyperopic lens requires a peripheral iridotomy (typically created with YAG laser prior to surgery) to prevent pupil block, while the current myopic lens has a central fenestration in the lens optic to allow free movement of aqueous, obviating the need for an iridotomy.
ICL or Laser (PRK, LASIK, SMILE)?
Laser corneal reshaping has proven an effective and safe intervention for the correction of refractive error. Several studies have now been published, however, showing that an ICL may be a safer and better option as compared with laser vision correction. A Cochrane review from 2014 showed that ICL surgery was safer for the correction of mid-to-high myopia as it resulted in significantly less loss of best spectacle corrected visual acuity at 12 months postoperatively. ICL typically gave better contrast sensitivity and had higher subjective patient satisfaction scores.16 Similar results are shown for ICL versus SMILE.17

Figure 17. ICL central port and shadow cast onto anterior lens; patients may experience transient haloing (Versace).
Phakic lens implants have historically been used for patients where laser corneal reshaping is contraindicated, or for extremes of refractive error. Recent data supports the shift toward the use of ICL as the preferred refractive surgical correction across the full range of refractive error, regardless of a patient’s suitability for laser. Dry eye is almost non-existent and quality of vision is consistently better with ICL, with less induction of highorder abberations. An exception is for low astigmatism (< 3D) where LASIK was superior to both ICL and SMILE.18
ICL Refractive Predictability
ICL refractive predictability is excellent and stable over time. Shimizu showed that for patients treated with a mean myopia of -7.5D, 100% had uncorrected visual acuity of 6/6 or better after three years. All (100%) of patients were within 0.5D of the targeted refractive outcome at three years (Figure 15).19
Sizing of the ICL is critical to safety and remains the more difficult aspect to get perfect. The myopic/myopic astigmatic lens comes in sizes from 12.1mm to 13.7mm in four increments. A lens that is too large will crowd the AC, reducing the corneal clearance and potentially narrowing the angle. Too small and there may be contact with the crystalline lens with an increased risk of cataract formation. While many techniques are described for predicting correct lens size, including sophisticated sulcus to sulcus ultrasound, our indirect extrapolation using the white-to-white measurement is equally predictive of lens vault (the space between the ICL and crystalline lens: ideal range 200 to 1000μm).20 In around 1% of patients, the ICL may need to be exchanged if the size is too large.
Endothelial Cell Density Change

Figure 18. Defocus curve for EDOF ICL, showing a 1D expansion of depth of focus. (Packer et al 2020).
Endothelial cell density change for the current ICL design is close to the physiological background rate of natural attrition with 0.5% (+/- 5.4) change at five years,19 (up to 8% for older lens styles21). This is contrasted with the change in endothelial cell density observed with iris supported phakic IOLs (Artisan), with a 10% decline at five years and 21% at 10 years.
Cataract Formation
Cataract formation is a potential risk with posterior chamber pIOLs. Surgical trauma can cause early lens opacity, but it is pICLlens touch and disturbed aqueous flow that results in later cataract formation. Anterior subcapsular is the typical appearance of pIOL induced cataract (Figure 16). While early versions of the Visian ICL had up to a 9.6% incidence of cataract formation,22 altered lens design and the introduction of a central hole (a 380μm port allowing more physiological flow of aqueous) has reduced the incidence to 0% (Figure 17).19
Glaucoma and Pigment Dispersion
Glaucoma and pigment dispersion are not associated with correctly sized ICL implants.20
Viva EDOF ICL

Table 1. Minimum endothelial cell density required for implantation of Artisan pIOL.
Viva, an extended depth of focus (EDOF) ICL, will become available for clinical use in 2021. Under development for several years, the EDOF version uses existing ICL refractive properties, combined with aspheric optics, to give a theoretical 2D expansion of depth of focus. The EDOF ICL can treat up to -18D myopia. Results from a recent multicentre trial showed 91% of implanted patients seeing better than 6/12 and N6 unaided binocularly, with no complaints of dysphotopsia. The mean increased range of focus was 1D, with more benefit observed in subjects with greater pre-existing presbyopia (Figure 18).
While the EDOF ICL offers a welcome new option for treating myopia and presbyopia with high patient satisfaction, a functional range of vision with spectacle independence and reversibility,23 more clinical data is needed to be confident that there are no unexpected compromises in visual quality. In the clinical study, 14% of patients had a transient decrease in corrected distance visual acuity, and there were significantly increased glare symptoms from baseline (assessed using a vision-related quality of life questionnaire).
The presbyopia correcting IPCL takes a different approach, being a full diffractive trifocal optic. Visual results are similar to those seen with trifocal IOLs, but there is inadequate data to assess the incidence of unwanted visual phenomena known to occur with diffractive multifocality. Endothelial cell safety is also not yet established, with one study showing a 9.9% decline in endothelial cell density at two years.24
CONCLUSION
Laser vision correction is synonymous with refractive surgery – patients all know and expect this and surgeons are familiar and comfortable with laser corneal reshaping. Phakic IOLs are gaining in popularity as the safety profile is understood and patients appreciate the additive and reversible nature of the procedure. The trend is toward increased use of phakic IOLs for a wider range of refractive treatments. EDOF and multifocal pIOLs offer a new intervention allowing older patients spectacle independence with a reversible procedure allowing for future cataract surgery. The Visian ICL (Staar) is a popular option for its small wound size, optical predictability and corneal endothelial safety profile.
Seven Advantages of Phakic Lens Implants
- The crystalline lens function and structure is maintained; accommodation is preserved and vitreoretinal complications are minimised,25
- Enhanced optical quality: pIOLs allow for a larger entry pupil and reduce higher order aberrations. This, rather than the two to three times increase, observed with laser corneal reshaping,7
- Reversibility: pIOLs can be removed, restoring the eye to its original condition. This is particularly useful because we know that most of these myopes will come to cataract surgery,
- Refractive predictability: The refractive outcome is not dependent upon corneal wound healing,
- The ocular surface is largely undisturbed, so dry eye / ocular surface disease is not a feature of ICL surgery,
- A wide range of refractive error can be treated (myopia up to -18, hyperopia up to +6 and astigmatism up to 6D), and
- As an additive and non-weakening procedure, corneal thickness and shape do not exclude patients from treatment.
To earn your CPD points from this article visit mieducation.com/refractive-correction-with-phakicintraocular-lenses.
Dr Patrick Versace is a cataract and refractive surgeon in both private and public hospital practice in Sydney, Australia. He holds a position at the Prince of Wales/ Sydney Eye Hospital where he is involved in registrar surgery training and also a position as Senior Lecturer at the University of New South Wales. Dr Versace consults at Bondi Junction in Sydney.
References
- Strampelli, B., [Tolerance of acrylic lenses in the AC in aphakia and refraction disorders]. Ann Ottalmol Clin Ocul, 1954. 80(2): p. 75-82.
- Holden, B.A., et al., Global Prevalence of Myopia and High Myopia and Temporal Trends from 2000 through 2050. Ophthalmology, 2016. 123(5): p. 1036-42.
- Bjerrum, S.S., K.L. Mikkelsen, and M. La Cour, Risk of pseudophakic retinal detachment in 202,226 patients using the fellow nonoperated eye as reference. Ophthalmology, 2013. 120(12): p. 2573-2579.
- Assad, M., et al., [Small Incision Lenticule Extraction (SMILE) for correction of myopic astigmatism]. J Fr Ophtalmol, 2020.
- Solomon, K.D., et al., LASIK world literature review: quality of life and patient satisfaction. Ophthalmology, 2009. 116(4): p. 691-701.
- FDA. LASIK Quality of life Collaboration Project www. fda.gov/MedicalDevices/ProductsandMedicalProcedures/ SurgeryandLifeSupport/LASIK/ucm190291. htm?source=govdelivery&utm_medium=email&utm_ source=govdelivery.
- Sarver, E.J., D.R. Sanders, and J.A. Vukich, Image quality in myopic eyes corrected with laser in situ keratomileusis and phakic intraocular lens. J Refract Surg, 2003. 19(4): p. 397-404.
- Barraquer, J., Anterior chamber plastic lenses. Results of and conclusions from five years’ experience. Trans Ophthalmol Soc U K, 1959. 79: p. 393-424.
- TGA, AcrySof Cachet phakic lens – update. Hazard alert and withdrawal from market www.tga.gov.au/alert/acrysofcachet- phakic-lens-update.
- Bras, J.F., Review of Binkhorst intraocular lenses. Br J Ophthalmol, 1977. 61(10): p. 631-3.
- BInkhorst, C.D., Use of the Pupillary Lens (Iris clip lens) in Aphakia. Brit.J.Ophthal, 1962. 46: p. 343.
- Worst, J.G., G. van der Veen, and L.I. Los, Refractive surgery for high myopia. The Worst-Fechner biconcave iris claw lens. Doc Ophthalmol, 1990. 75(3-4): p. 335-41.
- Jonker, S.M.R., et al., Long-Term Endothelial Cell Loss in Patients with Artisan Myopia and Artisan Toric Phakic Intraocular Lenses: 5- and 10-Year Results. Ophthalmology, 2018. 125(4): p. 486-494.
- Garcia-Feijoo, J., et al., Ultrasound biomicroscopy of silicone posterior chamber phakic intraocular lens for myopia. J Cataract Refract Surg, 2003. 29(10): p. 1932-9.
- Hoyos, J.E., M. Cigales, and J. Hoyos-Chacon, Zonular dehiscence two years after phakic refractive lens (PRL) implantation. J Refract Surg, 2005. 21(1): p. 13-7.
- Barsam A, A.B., Excimer laser refractive surgery versus phakic intraocular lenses for the correction of moderate to high myopia. Cochrane database of systematic reviews, 2014. issue 6.
- Wei, R., et al., Comparison of objective and subjective visual quality early after implantable collamer lens V4c (ICL V4c) and small incision lenticule extraction (SMILE) for high myopia correction. Acta Ophthalmol, 2020. 98(8): p. e943-e950.
- Ganesh, S., S. Brar, and A. Pawar, Matched population comparison of visual outcomes and patient satisfaction between 3 modalities for the correction of low to moderate myopic astigmatism. Clin Ophthalmol, 2017. 11: p. 1253- 1263.
- Shimizu, K., et al., Long-Term Comparison of Posterior Chamber Phakic Intraocular Lens With and Without a Central Hole (Hole ICL and Conventional ICL) Implantation for Moderate to High Myopia and Myopic Astigmatism: Consort- Compliant Article. Medicine (Baltimore), 2016. 95(14): p. e3270.
- Packer, M., Meta-analysis and review: effectiveness, safety, and central port design of the intraocular collamer lens. Clin Ophthalmol, 2016. 10: p. 1059-77.
- Alfonso, J.F., et al., Posterior chamber collagen copolymer phakic intraocular lenses to correct myopia: five-year followup. J Cataract Refract Surg, 2011. 37(5): p. 873-80.
- Chen, L.J., et al., Metaanalysis of cataract development after phakic intraocular lens surgery. J Cataract Refract Surg, 2008. 34(7): p. 1181-200.
- Packer, M., et al., Performance and Safety of the Extended Depth of Focus Implantable Collamer((R)) Lens (EDOF ICL) in Phakic Subjects with Presbyopia. Clin Ophthalmol, 2020. 14: p. 2717-2730.
- Bianchi, G.R., Initial Results From a New Model of Posterior Chamber Implantable Phakic Contact Lens: IPCL V2.0. Med Hypothesis Discov Innov Ophthalmol, 2019. 8(2): p. 57-63.
- Hernandez-Rodriguez, C.J. and D.P. Pinero, A systematic review about the impact of phakic intraocular lenses on accommodation. J Optom, 2020. 13(3): p. 139-145.





