
Atropine is an effective treatment for myopia. The key is to personalise treatment with a dosage that effectively slows myopia progression while minimising side effects.
The increasing prevalence of myopia is a worldwide concern, as is the rise in younger children with high or pathological myopia.1,2
the LAMP studies have cemented the idea that low dose atropine retards myopia progression
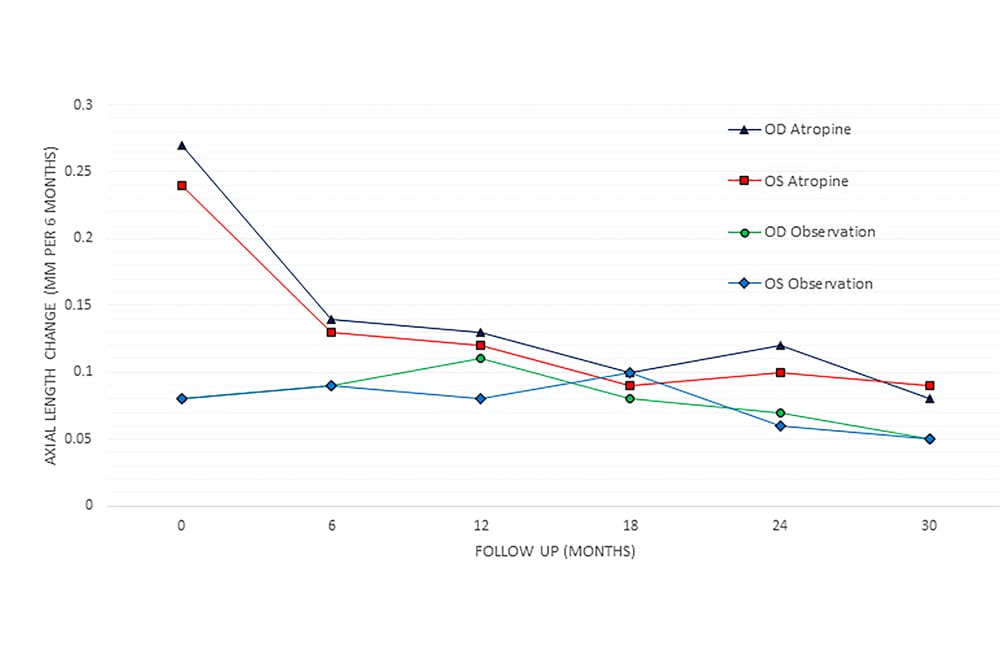
Figure 1. Graph showing the change in axial length in the observation and atropine 0.01% group, over each six months.
Pathological myopia, defined as -5.0D or greater by the World Health Organisation (WHO), comes with an increased risk of sight-threatening diseases, such as glaucoma, retinal detachment and macular disease.3,4 Bullimore and Brennan recently reported a 67% increased risk of myopic macular degeneration with each increase of 1D of myopia, and stated that, “even a 0.25D reduction in myopia (equivalent to about 0.1mm) yields close to a 10% reduction in risk”.5
Progressive juvenile myopia is characterised by an increased rate of axial length growth.6 Axial growth is a normal process in the emmetropisation of a newborn eye, which should result in emmetropia. However, genetic and external influences can lead to the growth of the eye beyond emmetropisation, thus becoming too long, resulting in myopia.
EFFECT OF ATROPINE
Early small studies using atropine 1% found reduced myopia progression in children.7-10 However, common side effects included photophobia, near blur and poor compliance.
In 2006, the ATOM study solidified the use of atropine to retard myopia progression in children.11 The ATOM 2 study further established that atropine slowed the rate of myopia progression in children.12,13 These studies randomised the use of different concentrations of atropine and noted that myopia progression was significantly retarded with even the lowest dose of atropine (0.01%).12 This dose was well-tolerated, as the known side effects of glare and near blur were minimal. The five-year follow-up, which included two years with treatment and one year without, and with treatment reinitiated if fast progression was observed, demonstrated that 0.01% achieved the best reduction in myopia progression overall. This included the year rebound occurred when treatment was ceased.14
More recently, the LAMP studies have cemented the idea that low dose atropine retards myopia progression.15,16 The effect is dose-responsive, meaning that the higher the dose, the greater the effect on myopia progression, as seen in refraction and axial length change. The side effect profile is also dose-dependent, with greater dilation at higher doses. The side effects are important in the Australian setting, as pupil dilation with low dose atropine is greater in populations with lighter iris pigmentation. A previous trial found that atropine 0.02% was the cut-off for most tolerability of symptomatic blur and glare.17
We now await the third phase of the LAMP study, where subjects will receive no treatment with low dose atropine, allowing rebound in this period to be compared. In the meantime, various international studies – in the US,18 in Europe,19 and a metaanalysis looking at the effect on axial length20 – have demonstrated a reduction in myopia progression with the use of atropine 0.01%. Review papers have further concluded the benefit of a low dose treatment, with two Cochrane reviews (2011 and 2020)21,22 and the American Academy of Ophthalmology, finding solid evidence that atropine effectively slows myopia progression.23
The focus now should lie on the lowest dose that will retard myopia sufficiently for the patient, while reducing their side effects. Additionally, when to start and stop treatment, and measure the treatment’s effectiveness, is paramount to best patient care.
MYOPIA IN THE AUSTRALIAN CONTEXT
Most of the major studies cited here were conducted in the Asian population with darker iris pigmentation and they documented faster myopia progression in general.24 In Australia, demographics include a mixed ethnicity which is important to take into account when extrapolating patient response and treatment tolerability.
Additionally, Australia has different lifestyle influences, such as higher exposure to natural light and less near work rates. Extensive research has found that myopia progression increased with less sunlight exposure25-29 and increased near work.30-34 Recent reports suggest the effects of sunlight and near work are significant; children on atropine 0.01% treatment, with stable myopia, increased their myopia progression during current COVID-19 lockdown restrictions, despite being older and previously assessed as stable.35,36
THE SHIFT TO AXIAL LENGTH MEASUREMENT
Management of myopic children has been to review dioptric progression to gauge when to treat and assess treatment success. However, more current publications have questioned refraction accuracy and its bias, with a clear preference to documenting axial length growth rather than base treatment on refraction for myopia management.37,38 Historically, data suggests that the average childhood axial length growth is 0.1mm per six months, with faster progression, in under nineyear- olds.6,11,39 There is ethnic variability, with greater progression in axial length documented in the Asian population.16,40,41
Figure 2. Graph showing the change in the spherical equivalent in the observation and atropine 0.01% group, over each six months.
The consensus regarding myopia control trials is that progression must be measured in axial growth.42 In one recent review, the use of axial length for treatment analysis in clinical practice and trials was extensively argued as the most appropriate method to analyse myopia control’s efficiency.37 Various reviews have considered fast myopia progression, greater than -0.5D progression per year, equating to 0.2mm growth per year.19,43 The measurement of axial growth in a six-month interval can demonstrate the rate of progression, as long as the patient can have the measurement performed accurately. In clinical practice, this is possible at four years and with a good fixation for measurement reproducibility using optical interferometric biometry, such as the Zeiss IOLMaster.
A recent Australian study44 put this hypothesis to the test. Children presenting with myopia were measured for a baseline of refraction and axial length, and reviewed six months later. Children who progressed faster than 0.1D per six months were given drops of atropine 0.01% nightly. At six months, their progression was compared. The study demonstrated that atropine 0.01% can retard progression measured in axial length in children in Australia.
The group of children who did not progress fast, termed slow progressors, were monitored. In the fast progressor group (treated with atropine 0.01%), the rate of progression was reduced by 50% in both axial length growth and refraction parameters compared to the pre-treatment growth rate (Figures 1 and 2). This effect was maintained on treatment, for up to two years in the study, and longer in clinical practice. The slow progressors maintained their slow growth, with an axial length growth rate that did not change significantly out to two years and a change of less than -0.5D annually.
Another important finding in this study was that slow and faster progressors included all ages and ethnic groups tested. There was a slight skew, with the younger and Asian ethnicity more likely to be fast progressors. However, there were children in their teens and non-Asian in the fast growth treatment group as well.
PERSONALISED TREATMENT ESSENTIAL
If we are to treat our myopic children accurately and safely, we need to personalise their treatment paradigm. Measurement of axial length before, during and after treatment allows the children to be identified and treatment effect to be measured over time. Analogous to glaucoma management, intraocular pressure measurement allows treatment goals to be set and response to be reviewed.
Measurement of axial length before initiating treatment with atropine can assist in identifying patients that require better myopia control, and guide the treatment regimen. Axial length progression can monitor and delay atropine drops as an intervention, with some children progressing very small amounts over many years. In comparison, some children increase their progression later in early adolescence, and treatment can be initiated then.
Starting at the lowest dose is logical to have a significant effect on axial growth and maximum tolerance. Monitoring the axial length change during treatment will allow the treatment effect to be noted with clarity, and guide consideration of a further increase in atropine concentration.
Interestingly, an atropine concentration dose change was required for some previously stable children who were increasing their axial elongation during the recent Sydney lockdown. While not all of my patients needed to increase their low dose atropine concentration, the ones who did were easily identified.
Axial growth measurements over time help indicate when a child may be nearing their natural reduction in myopic progression. Continued review of axial length during atropine weaning, and following cessation of therapy, may also prove useful to ensure minimal rebound.
AN EXCITING FUTURE
The future of myopia control is exciting. Our armament to combat the charge of myopia in our young population is increasing – new therapies, including glasses and contact lens designs, provide further potential. Combination therapies continue to add possibilities, yet these are still to be fully understood and tested.
In summary, low dose atropine is an effective treatment for myopia, and axial length measurement should be a mainstay in patient management to monitor myopia progression. It provides an accurate measure of myopic change and treatment effects in children.
To earn your CPD hours from this article, visit mieducation.com/low-dose-atropine-its-role-inmyopia- control.
Dr Loren Rose BSc (Hons I), MBBS (Hons), PhD, FRANZCO completed her medical degree from the University of Sydney, graduating with MBBS (Honours). Prior to that, she completed a Bachelor of Science from the University of Sydney, graduating with Honours (Class I) in Visual Neuroscience.
Dr Rose completed her ophthalmic training at the Royal Eye and Ear Hospital in Victoria. Following this, she underwent a fellowship in paediatric ophthalmology at the Royal Children’s Hospital, Melbourne. Now based in Sydney, she is a clinical senior lecturer at Macquarie University, and she practises privately at PersonalEyes Burwood, Sydney. In 2021, she completed her PhD, titled Myopia in Children, at Macquarie University.
References
- Wu PC, Chuang MN, Choi J, Chen H, Wu G, Ohno- Matsui K, et al. Update in myopia and treatment strategy of atropine use in myopia control. Eye (Lond). 2019;33(1):3-13.
- Grzybowski A, Kanclerz P, Tsubota K, Lanca C, Saw SM. A review on the epidemiology of myopia in school children worldwide. BMC Ophthalmol. 2020;20(1):27.
- Saw SM, Gazzard G, Shih-Yen EC, Chua WH. Myopia and associated pathological complications. Ophthalmic Physiol Opt. 2005;25(5):381-91.
- Mitchell P, Hourihan F, Sandbach J, Wang JJ. The relationship between glaucoma and myopia: the Blue Mountains Eye Study. Ophthalmology. 1999;106(10):2010-5.
- Bullimore MA, Brennan NA. Myopia Control: Why Each Diopter Matters. Optom Vis Sci. 2019;96(6):463-5.
- Tideman JWL, Polling JR, Vingerling JR, Jaddoe VWV, Williams C, Guggenheim JA, et al. Axial length growth and the risk of developing myopia in European children. Acta Ophthalmol. 2018;96(3):301-9.
- Bedrossian RH. The effect of atropine on myopia. Ophthalmology. 1979;86(5):713-9.
- Brenner RL. Further observations on use of atropine in the treatment of myopia. Ann Ophthalmol. 1985;17(2):137-40.
- Dyer JA. Role of cyclopegics in progressive myopia. Ophthalmology. 1979;86(5):692-4.
- Kennedy RH, Dyer JA, Kennedy MA, Parulkar S, Kurland LT, Herman DC, et al. Reducing the progression of myopia with atropine: a long term cohort study of Olmsted County students. Binocul Vis Strabismus Q. 2000;15(3 Suppl):281-304.
- Chua WH, Balakrishnan V, Chan YH, Tong L, Ling Y, Quah BL, et al. Atropine for the treatment of childhood myopia. Ophthalmology. 2006;113(12):2285-91.
- Chia A, Chua WH, Cheung YB, Wong WL, Lingham A, Fong A, et al. Atropine for the treatment of childhood myopia: safety and efficacy of 0.5%, 0.1%, and 0.01% doses (Atropine for the Treatment of Myopia 2). Ophthalmology. 2012;119(2):347-54.
- Chia A, Chua WH, Wen L, Fong A, Goon YY, Tan D. Atropine for the treatment of childhood myopia: changes after stopping atropine 0.01%, 0.1% and 0.5%. Am J Ophthalmol. 2014;157(2):451-7 e1.
- Chia A, Lu QS, Tan D. Five-Year Clinical Trial on Atropine for the Treatment of Myopia 2: Myopia Control with Atropine 0.01% Eyedrops. Ophthalmology. 2016;123(2):391-9.
- Yam JC, Li FF, Zhang X, Tang SM, Yip BHK, Kam KW, et al. Two-Year Clinical Trial of the Low-Concentration Atropine for Myopia Progression (LAMP) Study: Phase 2 Report. Ophthalmology. 2019.
- Yam JC, Jiang Y, Tang SM, Law AKP, Chan JJ, Wong E, et al. Low-Concentration Atropine for Myopia Progression (LAMP) Study: A Randomized, Double-Blinded, Placebo-Controlled Trial of 0.05%, 0.025%, and 0.01% Atropine Eye Drops in Myopia Control. Ophthalmology. 2019;126(1):113-24.
- Cooper J, Eisenberg N, Schulman E, Wang FM. Maximum atropine dose without clinical signs or symptoms. Optom Vis Sci. 2013;90(12):1467-72.
- Clark TY, Clark RA. Atropine 0.01% Eyedrops Significantly Reduce the Progression of Childhood Myopia. J Ocul Pharmacol Ther. 2015;31(9):541-5.
- Sacchi M, Serafino M, Villani E, Tagliabue E, Luccarelli S, Bonsignore F, et al. Efficacy of atropine 0.01% for the treatment of childhood myopia in European patients. Acta Ophthalmol. 2019;97(8):e1136-e40.
- Zhao Y, Feng K, Liu RB, Pan JH, Zhang LL, Xu ZP, et al. Atropine 0.01% eye drops slow myopia progression: a systematic review and Meta-analysis. Int J Ophthalmol. 2019;12(8):1337-43.
- Walline JJ, Lindsley K, Vedula SS, Cotter SA, Mutti DO, Twelker JD. Interventions to slow progression of myopia in children. The Cochrane database of systematic reviews. 2011(12):CD004916.
- Walline JJ, Lindsley KB, Vedula SS, Cotter SA, Mutti DO, Ng SM, et al. Interventions to slow progression of myopia in children. The Cochrane database of systematic reviews. 2020;1:CD004916.
- Pineles SL, Kraker RT, VanderVeen DK, Hutchinson AK, Galvin JA, Wilson LB, et al. Atropine for the Prevention of Myopia Progression in Children: A Report by the American Academy of Ophthalmology. Ophthalmology. 2017;124(12):1857-66.
- Ma Y, Zou H, Lin S, Xu X, Zhao R, Lu L, et al. Cohort study with 4-year follow-up of myopia and refractive parameters in primary schoolchildren in Baoshan District, Shanghai. Clin Exp Ophthalmol. 2018;46(8):861-72.
- Rose KA, Morgan IG, Smith W, Burlutsky G, Mitchell P, Saw SM. Myopia, lifestyle, and schooling in students of Chinese ethnicity in Singapore and Sydney. Arch Ophthalmol. 2008;126(4):527-30.
- Sherwin JC, Hewitt AW, Coroneo MT, Kearns LS, Griffiths LR, Mackey DA. The association between time spent outdoors and myopia using a novel biomarker of outdoor light exposure. Invest Ophthalmol Vis Sci. 2012;53(8):4363-70.
- French AN, Ashby RS, Morgan IG, Rose KA. Time outdoors and the prevention of myopia. Exp Eye Res. 2013;114:58-68.
- Wu PC, Chen CT, Lin KK, Sun CC, Kuo CN, Huang HM, et al. Myopia Prevention and Outdoor Light Intensity in a School-Based Cluster Randomized Trial. Ophthalmology. 2018;125(8):1239-50.
- Wu PC, Chen CT, Chang LC, Niu YZ, Chen ML, Liao LL, et al. Increased Time Outdoors Is Followed by Reversal of the Long-Term Trend to Reduced Visual Acuity in Taiwan Primary School Students. Ophthalmology. 2020;127(11):1462-9.
- Mutti DO, Mitchell GL, Moeschberger ML, Jones LA, Zadnik K. Parental myopia, near work, school achievement, and children’s refractive error. Invest Ophthalmol Vis Sci. 2002;43(12):3633-40.
- Saw SM, Chua WH, Hong CY, Wu HM, Chan WY, Chia KS, et al. Nearwork in early-onset myopia. Invest Ophthalmol Vis Sci. 2002;43(2):332-9.
- Ip JM, Saw SM, Rose KA, Morgan IG, Kifley A, Wang JJ, et al. Role of near work in myopia: findings in a sample of Australian school children. Invest Ophthalmol Vis Sci. 2008;49(7):2903-10.
- Morgan IG, Rose KA. Myopia and international educational performance. Ophthalmic Physiol Opt. 2013;33(3):329-38.
- Lin Z, Vasudevan B, Mao GY, Ciuffreda KJ, Jhanji V, Li XX, et al. The influence of near work on myopic refractive change in urban students in Beijing: a three-year follow-up report. Graefes Arch Clin Exp Ophthalmol. 2016;254(11):2247-55.
- Aslan F, Sahinoglu-Keskek N. The effect of home education on myopia progression in children during the COVID-19 pandemic. Eye (Lond). 2021.
- Zhang X, Cheung SSL, Chan HN, Zhang Y, Wang YM, Yip BH, et al. Myopia incidence and lifestyle changes among school children during the COVID-19 pandemic: a population-based prospective study. Br J Ophthalmol. 2021.
- Brennan NA, Toubouti YM, Cheng X, Bullimore MA. Efficacy in myopia control. Prog Retin Eye Res. 2021;83:100923.
- Flitcroft DI, He M, Jonas JB, Jong M, Naidoo K, Ohno- Matsui K, et al. IMI – Defining and Classifying Myopia: A Proposed Set of Standards for Clinical and Epidemiologic Studies. Invest Ophthalmol Vis Sci. 2019;60(3):M20-M30.
- Hou W, Norton TT, Hyman L, Gwiazda J, Group C. Axial Elongation in Myopic Children and its Association With Myopia Progression in the Correction of Myopia Evaluation Trial. Eye Contact Lens. 2018;44(4):248-59.
- Wei S, Li SM, An W, Du J, Liang X, Sun Y, et al. Safety and Efficacy of Low-Dose Atropine Eyedrops for the Treatment of Myopia Progression in Chinese Children: A Randomized Clinical Trial. JAMA Ophthalmol. 2020;138(11):1178-84.
- Yi S, Huang Y, Yu SZ, Chen XJ, Yi H, Zeng XL. Therapeutic effect of atropine 1% in children with low myopia. J AAPOS. 2015;19(5):426-9.
- Wolffsohn JS, Kollbaum PS, Berntsen DA, Atchison DA, Benavente A, Bradley A, et al. IMI – Clinical Myopia Control Trials and Instrumentation Report. Invest Ophthalmol Vis Sci. 2019;60(3):M132-M60.
- Wu PC, Yang YH, Fang PC. The long-term results of using low-concentration atropine eye drops for controlling myopia progression in schoolchildren. J Ocul Pharmacol Ther. 2011;27(5):461-6.
- Rose LVT, Schulz AM, Graham SL. Use baseline axial length measurements in myopic patients to predict the control of myopia with and without atropine 0.01. PloS one. 2021;16(7):e0254061.





