

Identifying drusen phenotypes on optical coherence tomography (OCT), and other retinal imaging modalities, is becoming increasingly important due to emerging treatments for the early stages of age-related macular degeneration (AMD).
Researchers at the Centre for Eye Research Australia (CERA) are seeking individuals with non-neovascular AMD to participate in research they hope will improve the outlook for those affected by this potentially devastating condition.
One in seven Australians aged 50 years or older have the early stages of AMD.1 Over five years, 15% of these individuals with the usually asymptomatic, early stages will develop late, vision-threatening complications including geographic atrophy (GA) and/or choroidal neovascularisation (CNV).2 Drusen, the hallmark feature of the early stages of AMD,2,3 are seen as yellow/white deposits on colour fundus photography (CFP) and as areas of retinal pigment epithelium (RPE) elevation on OCT.4 The utilisation of OCT, which allows for cross-sectional viewing of retinal structures,5 has enabled the characterisation of additional features of drusen, such as their internal reflectivity and homogeneity.6
…results from our cohort suggest that individuals with iAMD, who also have concomitant cuticular drusen or HCD, have a similar prognosis for progression and level of visual function as those with conventional drusen
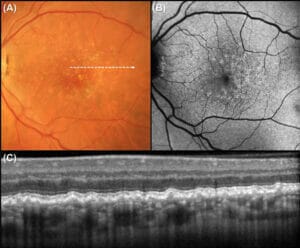
Figure 1. Multimodal imaging characteristics of cuticular drusen, as seen on (A) colour fundus photography, with multiple yellow, uniform deposits; (B) fundus autofluorescence, with focal spots of hypoautofluorescence; and (C)
OCT, with a B-scan corresponding to location indicated by the dashed white arrow in (A). In (C), cuticular drusen are visualised as blunted triangular elevations in a sawtooth configuration, with associated signal hypertransmission into the choroid.
AMD is defined by the presence of drusen, and staged by its size,2 yet the term ‘drusen’ encompasses many different phenotypes, which may each confer unique risks for progression. Drusen phenotypes include cuticular drusen,7 hyporeflective cores within drusen (HCD),8 large colloid drusen,9 and pachydrusen.10 High-resolution OCT has also allowed for easier differentiation of conventional drusen, which form under the RPE, from reticular pseudodrusen (RPD), which are located above the RPE.11 RPD are independently associated with an increased risk of progression to late AMD in individuals with CNV in the fellow eye.12,13 These deposits are also associated with an increased risk of progression to late AMD in those with the early signs of AMD,14 but this relationship with disease progression has not been observed in all longitudinal studies.15-17
Phenotyping drusen and other deposits such as RPD is important, especially with emerging treatments for earlier stages of AMD, as treatment efficacy may depend on particular disease phenotypes. In a recent interventional trial of sub-threshold nanosecond laser, aiming to slow progression of intermediate AMD (iAMD), the coexistence of RPD modified the response.18 In a post-hoc analysis, sub-threshold nanosecond laser appeared to have a possible beneficial treatment effect for those without RPD, but not so for those with RPD in individuals with bilateral large drusen.18 This indicates that there may be different and specific interventions required, dependent upon the type of deposit present in an eye.19
Cuticular drusen and HCD are two drusen phenotypes that are of great interest to both clinicians and researchers, and as such, have been the subject of two recent studies conducted by our group.8,20 In this article, we describe how they can be identified and, in light of our findings, their prognostic significance in individuals with iAMD.
CUTICULAR DRUSEN
What are They and How Can They be Identified?
Cuticular drusen were first described by Gass in 1977, who noted numerous, small, round, yellow nodules scattered throughout the fundus that were best visualised on fluorescein angiography, showing a ‘starsin- the-sky’ hyperfluorescence appearance.7,21 They are considered to be an early-onset drusen phenotype22,23 and can be seen in individuals younger than 50-years that do not fit the usual definition of AMD.2
On CFP, cuticular drusen appear as multiple yellow/pale, small, uniform, round deposits (Figure 1A) corresponding to a series of RPE elevations on OCT, often in a sawtooth configuration (Figure 1C).7,24,25 There is occasional thinning of the overlying RPE at the peak of each elevation, which is associated with hypertransmission of the OCT signal into the choroid, producing a characteristic ‘barcoding’ appearance (i.e., a series of small regions of signal hypertransmission alternating with normal transmission).26 On fundus autofluorescence, cuticular drusen have been reported to correspond to focal spots of hypoautofluorescence27,28 (Figure 1B), which can be surrounded by a rim of hyperautofluorescence.24,25
Why are They Important and What Did We Find?
Cuticular drusen have been reported to be associated with a high prevalence of CNV, one of the main late complications of AMD.2 Boon et al22 reported that 56% of 198 individuals with cuticular drusen seen at their tertiary referral centre had CNV, and Cohen et al29 suggested that those with cuticular drusen may require “close follow up” due to the “high prevalence of CNV”. However, individuals were included in these studies based solely on the presence of cuticular drusen, regardless of the coexistence of conventional drusen. These studies have also included participants as young as 23-years-of-age,24 who would therefore not fall into the diagnosis of typical AMD.2 As such, based on previous studies, it is not possible to draw any conclusions about the progression risk to vision-threatening complications in individuals with AMD who also have cuticular drusen.
In our study of cuticular drusen in AMD, recently published in Ophthalmology, we found that 25% of the 140 individuals in our cohort had cuticular drusen at baseline, which were always present bilaterally.20 Over a three-year study period, 48 out of 280 eyes progressed to late AMD when defined on OCT. The presence of cuticular drusen at baseline was not associated with the rate of progression to late AMD, both without adjustment for the confounders of age, drusen volume and the presence of pigmentary abnormalities, and also when these confounders were included in an adjusted analysis.20
We also investigated the impact of cuticular drusen on visual function (as assessed using microperimetry) and found that the presence of cuticular drusen was not associated with lower visual sensitivity at baseline, nor with a faster rate of visual sensitivity decline prior to the development of late AMD.20
HYPOREFLECTIVE CORES WITHIN DRUSEN
What are They and How Can They be Identified?
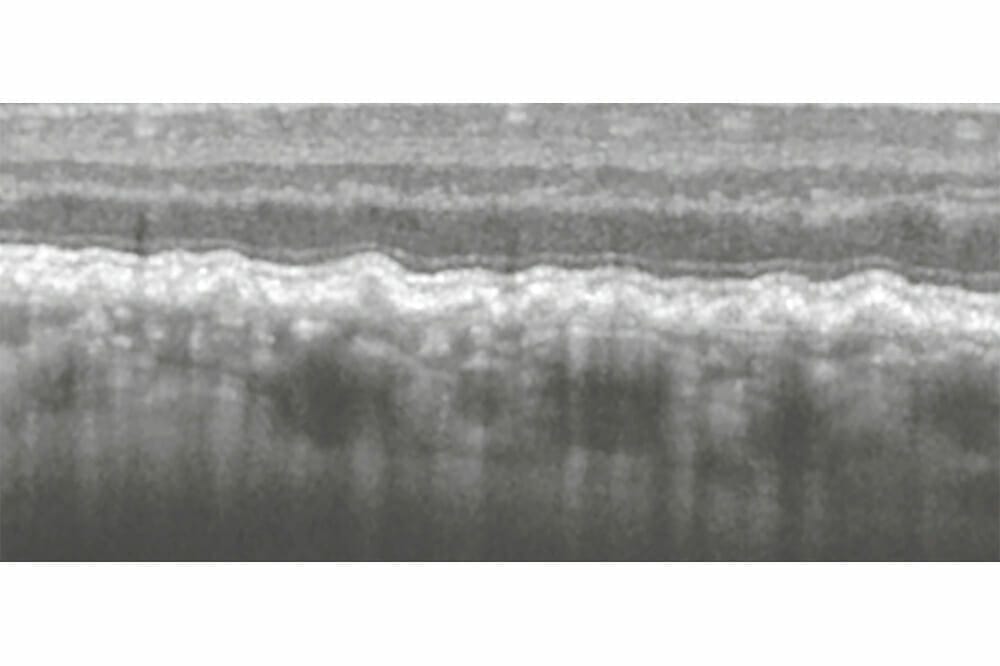
HCD is another drusen phenotype of interest. The term ‘hyporeflective core’ is used to describe the internal contents of a druse that is more hyporeflective than a typical druse (i.e. the core has less signal and thus appears more black), as seen in Figures 1B and 1C. HCD can only be determined on cross-sectional OCT imaging, as their en face fundus appearance is often indistinguishable from drusen without hyporeflective cores.

Figure 2. (A) Colour fundus photograph with OCT B-scans in (B) and (C). These OCT B-scans correspond to the dashed white arrows I and II respectively in (A), and show hyporeflective cores within drusen (HCD).
Why are They Important and What Did We Find?
Several previous studies have identified HCD or lesions including HCD as a risk factor for AMD progression,30,31 although different terminologies have been used to describe this feature. Their presence has been associated with an increased risk of developing local RPE atrophy30 and late AMD.31 However, even though this association has been established, it is still not known whether the presence of HCD is an independent risk factor for individuals with iAMD. This is because key risk factors for progression, including drusen volume, the presence of pigmentary abnormalities, and late AMD in the fellow eye, were not accounted for in prior analyses.
In our study of HCD, published in Ophthalmology Retina, we found that in a cohort of 280 eyes from 140 individuals, 20 (7%) eyes from 12 (9%) individuals had HCD present at baseline, which was associated with a non-significantly increased rate of progression to late AMD in unadjusted analysis.8 In contrast, the extent of HCD was significantly associated with an increased rate of progression to late AMD and lower visual sensitivity at baseline, in unadjusted analyses. However, these associations regarding the extent of HCD on progression and visual function, were no longer significant after adjusting for known risk factors for AMD progression (age, presence of pigmentary abnormalities and drusen volume). HCD extent was also not associated with a faster rate of visual sensitivity decline prior to the development of late AMD, with and without adjustment.8
PROGNOSTIC SIGNIFICANCE OF CUTICULAR DRUSEN AND HYPOREFLECTIVE CORES
We found that in a cohort of individuals with bilateral large drusen, the presence of cuticular drusen and the presence/extent of HCD were not independently associated with progression to late AMD over three years. Additionally, the presence of cuticular drusen and the presence/extent of HCD were both not associated with baseline visual sensitivity, or the rate of visual sensitivity decline prior to the development of late AMD, after adjusting for key risk factors of disease progression (age, drusen volume and pigmentary abnormalities).
This indicates the importance of considering all known risk factors in an eye when assessing progression risk. The results from our cohort suggest that individuals with iAMD, who also have concomitant cuticular drusen or HCD, have a similar prognosis for progression and level of visual function as those with conventional drusen. Thus, there need not be a differentiation in their management in clinical practice. As outlined in the RANZCO Referral Pathway for AMD Management32 and Optometry Australia’s chairside reference for the diagnosis and management of age-related macular degeneration,33 these individuals with iAMD should be reviewed by an optometrist every six to 12 months depending on clinical risk modifiers, such as the presence of hyperreflective foci, nascent GA, RPD, and non-exudative macular neovascularisation. While the presence of cuticular drusen or HCD in individuals with AMD should not change optometric management, the presence of clinical risk modifiers (including other drusen phenotypes and deposits such as RPD) may. As such, it is imperative that clinicians monitoring patients with AMD familiarise themselves with various features of anatomical change seen on OCT and other imaging modalities.
Our team at CERA is currently recruiting individuals with AMD to take part in both treatment and observational studies. To do this, we are calling on the partnership of optometrists throughout Victoria to help identify individuals with non-neovascular AMD, and to offer them the opportunity to be involved in research. These study visits are conducted at the Macular Research Unit, CERA, which is located at The Royal Victorian Eye and Ear Hospital.
With the help of the optometry profession and our participants, we hope to continue to make progress towards our goal of improving the lives of the many individuals who are affected by this potentially devastating condition.
Kai Lyn Goh studied optometry at The University of Melbourne. Following graduation, she worked at an independent private practice in regional Victoria, and then at a refractive surgery clinic in Melbourne. Ms Goh is currently a PhD Candidate at CERA, where she has also worked as a Clinical Trial Coordinator in the Macular Research Unit.
Dr Carla J. Abbott is a Senior Research Fellow at CERA. She trained as an optometrist and completed her PhD at The University of Melbourne. Dr Abbott is also a clinical instructor of optometry students at the Australian College of Optometry and a practitioner member on the Optometry Board of Australia.
Professor Robyn H. Guymer AM is a Professor of Ophthalmology at The University of Melbourne and a senior retinal specialist at The Royal Victorian Eye and Ear Hospital. She is also a Deputy Director and Head of Macular Research at CERA, leading a team of researchers primarily investigating AMD.
References
- Keel S, Xie J, Foreman J, et al. Prevalence of Age-Related Macular Degeneration in Australia: The Australian National Eye Health Survey. JAMA Ophthalmol 2017;135(11):1242-9.
- Ferris FL, 3rd, Wilkinson CP, Bird A, et al. Clinical classification of age-related macular degeneration. Ophthalmology 2013;120(4):844-51.
- Bird AC, Bressler NM, Bressler SB, et al. An international classification and grading system for age-related maculopathy and age-related macular degeneration. The International ARM Epidemiological Study Group. Surv Ophthalmol 1995;39(5):367-74.
- Hee MR, Baumal CR, Puliafito CA, et al. Optical Coherence Tomography of Age-related Macular Degeneration and Choroidal Neovascularization. Ophthalmology 1996;103(8):1260-70.
- Drexler W, Morgner U, Ghanta RK, et al. Ultrahighresolution ophthalmic optical coherence tomography. Nat Med 2001;7(4):502-7.
- Khanifar AA, Koreishi AF, Izatt JA, Toth CA. Drusen ultrastructure imaging with spectral domain optical coherence tomography in age-related macular degeneration. Ophthalmology 2008;115(11):1883-90.
- Gass JDM. Stereoscopic Atlas of Macular Diseases: Diagnosis and Treatment, Fifth ed. St. Louis, MO: Mosby, 1977.
- Goh KL, Abbott CJ, Hadoux X, et al. Hyporeflective Cores within Drusen: Association with Progression of Age-Related Macular Degeneration and Impact on Visual Sensitivity [published online December 2, 2021]. Ophthalmol Retina 2021. doi:10.1016/j.oret.2021.11.004.
- Guigui B, Leveziel N, Martinet V, et al. Angiography features of early onset drusen. Br J Ophthalmol 2011;95(2):238-44.
- Spaide RF. Disease Expression In Nonexudative Age- Related Macular Degeneration Varies With Choroidal Thickness. Retina 2018;38(4):708-16.
- Zweifel SA, Spaide RF, Curcio CA, et al. Reticular pseudodrusen are subretinal drusenoid deposits. Ophthalmology 2010;117(2):303-12 e1.
- Finger RP, Wu Z, Luu CD, et al. Reticular pseudodrusen: a risk factor for geographic atrophy in fellow eyes of individuals with unilateral choroidal neovascularization. Ophthalmology 2014;121(6):1252-6.
- Hogg RE, Silva R, Staurenghi G, et al. Clinical characteristics of reticular pseudodrusen in the fellow eye of patients with unilateral neovascular age-related macular degeneration. Ophthalmology 2014;121(9):1748-55.
- Domalpally A, Agron E, Pak JW, et al. Prevalence, Risk, and Genetic Association of Reticular Pseudodrusen in Agerelated Macular Degeneration: Age-Related Eye Disease Study 2 Report 21. Ophthalmology 2019;126(12):1659-66.
- Sleiman K, Veerappan M, Winter KP, et al. Optical Coherence Tomography Predictors of Risk for Progression to Non-Neovascular Atrophic Age-Related Macular Degeneration. Ophthalmology 2017;124(12):1764-77.
- Thiele S, Nadal J, Pfau M, et al. Prognostic Value of Retinal Layers in Comparison with Other Risk Factors for Conversion of Intermediate Age-related Macular Degeneration. Ophthalmol Retina 2020;4(1):31-40.
- Wu Z, Fletcher EL, Kumar H, et al. Reticular pseudodrusen: A critical phenotype in age-related macular degeneration. Prog Retin Eye Res 2021:101017.
- Guymer RH, Wu Z, Hodgson LAB, et al. Subthreshold Nanosecond Laser Intervention in Age-Related Macular Degeneration: The LEAD Randomized Controlled Clinical Trial. Ophthalmology 2019;126(6):829-38.
- Guymer RH. Splitting the Lumps: The Importance of Phenotyping Drusen. Ophthalmology 2018;125(1):6-7.
- Goh KL, Chen FK, Balaratnasingam C, et al. Cuticular Drusen in Age-Related Macular Degeneration: Association with Progression and Impact on Visual Sensitivity [published online February 1, 2022]. Ophthalmology 2022. doi:10.1016/j.ophtha.2022.01.028.
- Gass JDM, Jallow S, Davis B. Adult vitelliform macular detachment occurring in patients with basal laminar drusen. Am J Ophthalmol 1985;99(4):445-59.
- Boon CJ, van de Ven JP, Hoyng CB, et al. Cuticular drusen: stars in the sky. Prog Retin Eye Res 2013;37:90-113.
- Russell SR, Gupta RR, Folk JC, et al. Comparison of color to fluorescein angiographic images from patients with early-adult onset grouped drusen suggests drusen substructure. Am J Ophthalmol 2004;137(5):924-30.
- Balaratnasingam C, Cherepanoff S, Dolz-Marco R, et al. Cuticular Drusen: Clinical Phenotypes and Natural History Defined Using Multimodal Imaging. Ophthalmology 2018;125(1):100-18.
- Sakurada Y, Parikh R, Gal-Or O, et al. CUTICULAR DRUSEN: Risk of Geographic Atrophy and Macular Neovascularization. Retina 2020;40(2):257-65.
- Jaffe GJ, Chakravarthy U, Freund KB, et al. Imaging Features Associated with Progression to Geographic Atrophy in Age-Related Macular Degeneration: Classification of Atrophy Meeting Report 5. Ophthalmol Retina 2021;5(9):855-67.
- Spaide RF, Curcio CA. Drusen characterization with multimodal imaging. Retina 2010;30(9):1441-54.
- Meyerle CB, Smith RT, Barbazetto IA, Yannuzzi LA. Autofluorescence of basal laminar drusen. Retina 2007;27(8):1101-6.
- Cohen SY, Meunier I, Soubrane G, et al. Visual function and course of basal laminar drusen combined with vitelliform macular detachment. Br J Ophthalmol 1994;78(6):437-40.
- Ouyang Y, Heussen FM, Hariri A, et al. Optical coherence tomography-based observation of the natural history of drusenoid lesion in eyes with dry age-related macular degeneration. Ophthalmology 2013;120(12):2656-65.
- Tan ACS, Pilgrim MG, Fearn S, et al. Calcified nodules in retinal drusen are associated with disease progression in age-related macular degeneration. Sci Transl Med 2018;10(466).
- The Royal Australian and New Zealand College of Ophthalmologists. RANZCO: Referral Pathway for AMD Management. 2018.
- Hart KM, Abbott C, Ly A, et al. Optometry Australia’s chairside reference for the diagnosis and management of age-related macular degeneration. Clin Exp Optom 2020;103(3):254-64.





