

The need to aero-medically evacuate injured service personnel from war zones inspired an Australian collaboration to develop a new approach to repairing retinal detachments. The approach, which will undergo clinical trial in 2023, is expected to improve vision outcomes and enhance quality of life.
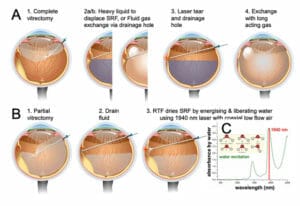
Figure 1. A. Existing rhegmatogenous retinal detachment repair requires the use of tamponade. B. The retinal thermofusion approach involves a short dehydration step to remove sub-retinal fluid using a laser for targeted excitement and liberation of water molecules at key water absorption peaks (1940nm).
A new method for rhegmatogenous retinal detachment (RRD) repair, called retinal thermofusion (RTF),1 can seal retinal tears intraoperatively with the potential for faster visual rehabilitation. In doing so, patients will enjoy an earlier return to normal activities, including flying. Additionally, the approach has potential to prevent reductions in central vision that can accompany retinal detachment repair.
INSPIRED BY NEED
It was the inability to aero-medically evacuate injured service personnel from war zones that prompted the United States Army Medical Research and Materiel Command to fund development of a surgical approach and device to facilitate translation of the RTF method into clinical care. The project involved a collaboration between the Department of Optometry and Vision Sciences, University of Melbourne, and the Centre for Eye Research Australia (CERA). Together, they have developed a new device that has been validated in a rabbit retinal detachment model. Their method will be evaluated in a clinical trial at the Royal Victorian Eye and Ear Hospital Melbourne in early 2023.
DEHYDRATING THE SUBRETINAL SPACE
For over a century, retinal detachment repair has been based on the principle established by Jules Gonin,2 3 which is to identify and thermally injure the causal retinal tear(s). However, for wound healing to create a seal, both tissues must be in contact until a stable bond develops, which can take days to weeks.
Currently, the most common approach to retinal detachment repair is vitrectomy, laser retinopexy and intraocular tamponade – either gas or a liquid (usually silicone oil) (Figure 1). Although highly successful at reattaching the retina, this procedure requires subretinal fluid (SRF) to be drained intraoperatively followed by laser photocoagulation to repair the retinal tear. Finally, a gas or oil tamponade is introduced to support the formation of a tight bond between the retina and the underlying tissue. However, the use of tamponade is increasingly recognised as a cause of reduced quality of vision. Randomised trials comparing macular off detachment cases treated with vitrectomy or pneumatic retinopexy (which promotes spontaneous reattachment), have confirmed that the vitrectomy group had worse visual acuity, more metamorphopsia, and retinal fold formation or macular displacement.4,5 The ideal retinopexy method should seal the tear intraoperatively and allow the retina to reattach itself by its own physiological mechanisms to remove fluid, which involves retinal pigment epithelial (RPE) pumping and the oncotic gradient between the vitreous and the choroid.6-8

Figure 2. A. It is very difficult to draw out water as the adhesion of water to surfaces is stronger than the cohesion forces within water. B. Without removing water, tissues cannot be photocoagulated together. This is like frying two
eggs: they remain independent if there is fluid between them during heating, however, when all fluid is removed so that they are in direct contact, they will be integrated (coagulated) upon cooking. This is the key concept of the
retinal thermofusion technique.
The key concept introduced by the RTF method is a preliminary step of dehydrating the subretinal space (SRS) under the retinal tear margin prior to photocoagulation. This was validated using a room temperature airstream in a sheep eye ex vivo model.1
The key problem overcome by the RTF method is that current surgery leaves a very thin layer of subretinal fluid. Current suction approaches cannot remove this water because water-to-water cohesion forces are less than water-to-surface adhesion, which is why water drips from a tap (Figure 2A), such that some water will always adhere to the retina and RPE. This water layer prevents effective photocoagulation (using 810nm or 532nm lasers) of the RPE/choroid/retina, and although laser energy is absorbed by pigment in the RPE and choroid, the SRF keeps the retina separate. Much like cooking eggs; when separated they coagulate individually but if in contact when heated, they make an integrated coagulum (Figure 2B). To remove SRF fluid, the physical properties of water are leveraged, whereby near infrared wavelengths (with absorption peaks at 1490nm and 1940nm) are absorbed and directly energise the oxygen:hydrogen bonds so that liquid phase water molecules are liberated into air at below coagulation temperatures9 (Figure 1C). This ‘photodehydration’ is associated with the formation of microdroplets of condensation without a coaxial airflow. The addition of a coaxial low-rate airstream significantly speeds the dehydration and limits tissue temperature rise.
In laboratory testing using a retinal detachment model, it was shown that the current approach of fluid removal by suction, followed by laser photocoagulation, did not produce a watertight bond between the retina and underlying RPE and choroid. On the other hand, dehydrating the subretinal fluid before photocoagulation created a strong water-tight bond between the retina and the underlying RPE and choroid.
A prototype console, incorporating a 1940nm laser diode with a coaxial airflow, delivered via a unique coaxial intraocular laser probe, was developed for preclinical testing. When evaluated in vivo in the pigmented rabbit lensectomy/vitrectomy/retinal detachment model, it showed that the RTF approach achieved stable retinal reattachment at the two-week endpoint.
NEXT STEPS
The team now has funding to support translation of this method to clinical care with i) the development of a precommercial laser/air stream console, ii) the development of a photodehydration method training module for participating surgeons, and iii) a preclinical trial recruiting 10 patients with ‘macula off ’ rhegmatogenous retinal detachment from the Royal Victorian Eye and Ear Hospital (East Melbourne, Victoria).
ADVANTAGES FOR SURGEON AND PATIENT
The key advantage offered by the laser-based RTF method is that retinal tears can be sealed intraoperatively with a short dehydrating laser preparation of the retinal tear margin and should offer the quality of vision advantages of pneumatic retinopexy for rhegmatogenous retinal detachment repair. The photodehydration method is intuitive for retinal surgeons accustomed to laser photocoagulation of tears and should not significantly add time to the operation because the need to introduce the tamponade has been eliminated. There should be significant quality of life advantages because the absence of gas means a much faster return to normal activities while offering a better visual outcome. Additionally, the ability to seal inferiorly located tears should minimise the need for silicone oil with the obligatory second procedure for its removal. Also, by creating an instantaneous seal, the RTF approach may help to prevent retina slip and folds, potentially reducing the risk of vision loss.
The basic principles established by Gonin a century ago are still relevant today, but the ability to seal tears without tamponade to support the wound healing reaction offers exciting advantages for retinal detachment repair in the future.
Associate Professor Wilson Heriot, Centre for Eye Research Australia, Department of Surgery, Ophthalmology, and the Department of Optometry & Vision Sciences, University of Melbourne.
Associate Professor Bang Bui, Department of Optometry & Vision Sciences, University of Melbourne.
Associate Professor Andrew Metha, Department of Optometry & Vision Sciences, University of Melbourne. Ms Anh Hoang, Department of Optometry & Vision Sciences, University of Melbourne.
References
- Heriot W. Thermofusion of the retina with the RPE to seal tears during retinal detachment repair. Graefe’s Archives for Clinical & Experimental Ophthalmology 2016;254(4):691-96. doi: 10.1007/s00417-016-3295-0.
- Rumpf J. Jules Gonin. Inventor of the surgical treatment for retinal detachment. Survey of Ophthalmology 1976;21(3):276-84.
- Wolfensberger T. Jules Gonin. Pioneer of retinal detachment surgery. Indian Journal of Ophthalmology 2003;51(4):303-08.
- Brosh K, Francisconi CLM, Qian J, et al. Retinal displacement following pneumatic retinopexy vs pars plana vitrectomy for rhegmatogenous retinal detachment. JAMA Ophthalmology 2020 doi: 10.1001/ jamaophthalmol.2020.1046
- Hillier RJ, Felfeli T, Berger AR, et al. The pneumatic retinopexy versus vitrectomy for the management of primary rhegmatogenous retinal detachment outcomes randomized trial (PIVOT). Ophthalmology 2019;126(4):531- 39. doi: https://doi.org/10.1016/j.ophtha.2018.11.014.
- Bill A, Phillips CI. Uveoscleral drainage of aqueous humour in human eyes. Exp Eye Res 1971;12(3):275-81. [published Online First: 1971/11/01].
- Marmor MF. Control of subretinal fluid: Experimental and clinical studies. Eye 1990;4(2):340-44. doi: 10.1038/ eye.1990.46.
- Heriot WJ, Metha AB, He Z, et al. Optimizing retinal thermofusion in retinal detachment repair: achieving instant adhesion without air tamponade. Ophthalmology Science 2022:100179.
- Bertie JE, Lan Z. Infrared intensities of liquids xx: the intensity of the oh stretching band of liquid water revisited, and the best current values of the optical constants of H2O(l) at 25°C between 15,000 and 1 cm−1. Applied Spectroscopy 1996;50(8):1047-57. doi: 10.1366/0003702963905385.





