

We yearn to see the sun pop through the clouds, for the end of the cold winds, and the chance to enjoy the great outdoors in a light t-shirt and shorts. But for those who suffer from allergic eye disease, the pollens, grasses, and dust mites so prevalent during this season, can make every day uncomfortable.
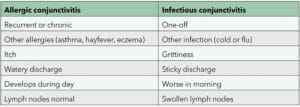
Table 1. Simple differences between allergic and infectious conjunctivitis.
With allergies affecting 20% of Australians,1 and 30–40% of New Zealanders, it comes as no surprise that there are long wait lists to see allergy specialists throughout the country.
Allergies occur when a person has a reaction to allergens, such as dust mites, pets, pollen, grasses, insects, ticks, moulds, foods, and some medications. The reaction may be in the form of hay fever, eczema, rash, vomiting, or in the worst case, anaphylaxis requiring hospitalisation. The person may also develop allergic eye disease which, like dry eye disease, is an inflammatory disease at the ocular surface.2 Affecting 10–20% of the global population,3 allergic eye disease is most common in people with atopic diseases – asthma, eczema, and rhinitis. It can be acute and recurrent, or chronic, which tends to be more persistent.
The impact of allergies on quality of life is often underestimated – when chronic, allergies can affect a person’s ability to attend school and work, discourage them or even disallow them to socialise or travel, and become a financial burden as they attend specialist appointments, try different treatments, and are forced to purchase non-allergenic foods/ products or adapt their home and work environments to avoid triggers.
ALLERGIC CONJUNCTIVAL DISEASES
Allergic conjunctival diseases (ACDs) are predominantly caused by an IgE-mediated immediate hypersensitivity response, in which contact with an antigen causes mast cells to release histamine and other factors, causing an inflammatory reaction.
There are four types of ACDs:
- Allergic conjunctivitis: An allergic response to allergens, such as pollen that typically causes mild to moderate symptoms such as red, itchy, and watery eyes; usually associated with rhinitis,
- Vernal disease keratoconjunctivitis: A relatively uncommon, seasonally recurring, and severe form of allergic eye disease that can cause severe damage to the ocular surface, leading to corneal scarring and vision loss if not properly treated,
- Atopic keratoconjunctivitis: The most severe allergic eye disease, with a genetic disposition, it is often associated with atopic dermatitis and can occur year round, and
- Giant papillary conjunctivitis: a less common condition, mostly affecting contact lens wearers and people with prosthetic eyes.1
SIGNS AND SYMPTOMS
Allergic eye disease generally affects both eyes, causing itching accompanied by watering and redness. Swelling of the conjunctiva and eyelids can be involved and patients may present with dark rings around the eyes.
In the case of vernal disease keratoconjunctivitis, patients may describe burning or stinging eyes and light sensitivity.
Patients who have giant papillary conjunctivitis will present with large papillae on the inner surface of their upper eyelid.
Patients with chronic allergic eye disease can develop more severe signs and even clinical syndromes. These can range from pain and corneal scarring to early cataracts, and in rare cases, glaucoma. Advanced disease cases can be sight threatening.5
Allergic conjunctivitis can be mistaken for infective conjunctivitis, causing unnecessary inconvenience and concern for the patient.
Table 1 summarises the main differences between the two.
TREATMENTS
With no available cure, allergies have become a significant public health issue – demonstrated by long waiting lists for patients to see allergy specialists throughout Australia and New Zealand.
Treatment to manage allergies as they occur will differ from patient-to-patient and will be based on the severity and chronicity of their disease.
Patients who live with any allergy should be counselled to do their best to avoid the relevant allergens. However, realistically this will not always be possible, which makes preparation the key to minimising the impact of reactions when they occur.
For allergic eye disease, cold compresses are an ideal place to start in the event of a reaction, along with preservative-free artificial tears.
From there, the cascade of treatment options begins with oral antihistamines, although it’s important to make patients aware that the antimuscarinic effects of medications, such as Claratyne and Zyrtec, can exacerbate dry eye disease by decreasing aqueous production.6 These medications can also cause dry mouth, tachycardia, and mucous thickening.6
Many patients prefer antihistamine or steroid based nasal sprays which are easily available at the pharmacy.
A more effective approach may be the use of topical antihistamines (preferably preservative free as preservatives such as benzalkonium chloride can disrupt corneal and conjunctival epithelium and exacerbate dry eye). Combination mast cell stabilisers and antihistamine drops are extremely effective for most patients, however acute cases may require a short course of topical steroids. For long term management, drugs like Cyclosporin A can work to suppress low grade inflammation and reduce severe episodes. Cyclosporin A – a peptide which inhibits T-cell activation to control the inflammatory cytokine production – also inhibits apoptosis and can increase conjunctival goblet cell density. Additionally, these drops work well in combination with antihistamine/mast cell stabilisers.
CONCLUSION
Unless you’ve lived with allergies or lived alongside someone who deals with them every day, it’s easy to believe that allergic reactions are overblown. However, having watched my daughter deal with allergies since she was a tiny baby, I know how very real they are, and the impact they can have on lifestyle, personal confidence, and comfort. Let’s do what we can to make every day of every patient’s life happier, more fulfilling, and more comfortable.
References
- aph.gov.au/Parliamentary_Business/ Committees/House/Health_Aged_Care_and_Sport/Allergiesandanaphylaxis/Report/section?id=committees%2 freportrep%2f024422%2f72559
- Tatsuma Kishimoto; Ken Fukuda; Waka Ishida; Atsuki Fukushima. The interaction between dry eye disease and allergic conjunctivitis in mice. Investigative Ophthalmology & Visual Science July 2018, Vol.59, 120. doi:
- Patel D S, Arunakirinathan M, Stuart A, AngunawelaR. Allergic eye disease BMJ 2017; 359: j4706 doi:10.1136/bmj.j4706
- sciencedirect.com/topics/medicine-and-dentistry/ allergic-conjunctivitis
- co.nz/eye-conditions/allergiceye- disease/
- Rayner J. Spring-is-here-is-it-allergy-dry-eye-or-both. mivision.com.au/2021/08/





