

In this mivision spotlight, Dr Ben Ashby explains the prevalence, incidence, insights, and trends of patients with myopia, as seen in Specsavers practices over the past five years. He also discusses the challenges that the industry will tackle in the future as it aims to support patients with the condition.
The prevalence of myopia (defined as spherical equivalent refraction of less than -0.50D in one or two eyes)1 is thought to be increasing worldwide. It is estimated that in 2000, 1.4 billion people were myopic, and by 2050 that number will rise to 4.8 billion.2
Modern lifestyles and living environments seem rife for the development of a generation of myopes who don’t spend enough time outside in fresh air, over-indexing on activities requiring near vision
Figure 1. Myopia rates among children (≤18 years) at Specsavers’ Australian practices.
Relatively few studies have investigated myopia prevalence in Australia in detail. In a study of 4,365 socioeconomically disadvantaged children published in 2020, Fu et al. found a prevalence of myopia of 3.4% and 4.4% from 2014 to 2018.3 This prevalence is significantly lower than that seen in non-disadvantaged populations.
In 2013, French et al. found an overall prevalence of 13% to 14.4% in urban children aged six to 12. Among Caucasian children, myopia prevalence ranged from 4.4% to 8.3%, and from 38.5% to 42.7% among children with an East Asian background.4 In an earlier study, Junghans et al. found an overall prevalence of 6.5% to 8.4% among four to 12 year old children.5 Each of these studies found that myopia prevalence increased with age, though none included children older than 15.
To date, no large epidemiological studies have been conducted in New Zealand. It is reasonable to assume that myopia prevalence in New Zealand is, broadly, not dissimilar to Australia, though there may be differences given New Zealand’s different cultural populations and its lack of funded eye care contributing to a complex range of access issues. Specsavers offers all children under 16 years free eye tests and is also supportive of the work of the eye health coalition, Eye Health Aotearoa, in lobbying the government for a national eye health survey. This aims to uncover a clearer picture of the state of New Zealand’s eye health, including the frequency of causes of vision loss and impairment such as myopia, so that appropriate strategies and policies can be formed to best care for New Zealanders both diagnosed and at risk.
For the purposes of this article, I examined Australian data and we hope to uncover more about the eye health of New Zealanders in due course.
CHILDREN’S EYE CARE
From July 2021 to June 2022, Specsavers provided services to 3.7m patients in Australia. Nearly half a million of them were aged 18 years or younger, representing 13.3% of our total patient volume. This remained similar across every state, but as one might expect, younger patients were more commonly seen in metro and regional locations rather than in central business districts.
Over the past five years, there has been a consistent pattern of children seeking eye care during school holidays, especially in January as parents prepare their children for school.
Our data shows that COVID-19 restrictions, particularly in school holiday times and throughout the past two years, impacted eye test visitation for this patient group. Any patient backlogs are now beginning to clear, with children returning for eye tests at rates similar to those pre-COVID.
MYOPIA IN SPECSAVERS PATIENTS
Since 2017, more than 394,000 patients aged 18 or younger have received a prescription for a spherical equivalent refraction of less than -0.50D at a Specsavers practice.
The incidence of patients with myopia aged 18 and under has increased from 24.6% of all patients in the age group in 2017 to 28.3% in 2022. This is equivalent to 3.5% of all Specsavers patients in 2017 and 3.8% in 2022. Of a subset of patients aged eight to 15 in 2020, 28% were myopic, showing that the prevalence of the condition increases in older children (Figure 1).
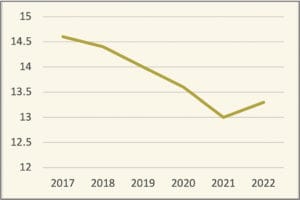
Figure 2. Average age of children (≤18 years) when first diagnosed with myopia at Specsavers’ Australian practices.
The prevalence of myopia in younger ages (eight to 11) was higher in 2020 than previous years. However, the number of patients in this age range was much greater in 2019 (134,862 patients) than in 2020 (93,887 patients). While an interesting downward trend, this is also likely a result of the COVID-19 pandemic skewing attendance rates for patients with no vision problems (e.g. emmetropes and low hyperopes) compared to those with vision problems (e.g. myopes).
Further to this, Specsavers data shows the average age of patients with myopia has decreased from 14.4 years old in 2018 to 13.3 years old in 2022 (Figure 2).
Fortunately, despite the increasing prevalence of myopia among our patients, we have not seen an increase in high myopia. More than three quarters of myopic children have a prescription in their worse eye of less than -3.00D. Just over one in five have a prescription between -3.00 and -6.00D. Unfortunately, a small percentage of children – between three and four in 100 – are high myopes, with prescriptions larger than -6.00D, though this is much lower than reported in some recent studies.
The data that we’re sharing is based on the children who have visited our practices for eye care services over the past five years. It suggests that the prevalence of myopia among children in our patient base is higher than would be expected, given the national population prevalence. However, in interpreting this data, it is important to consider potential selection bias. It is logical to assume that children with myopia are inherently more likely to visit an optometrist, due to reduced vision, than emmetropic children with no vision problems. This may lead to an artificially high prevalence of myopia among our patient base.
RECALL OF MYOPIC PATIENTS
Most (74%) patients who have myopic prescriptions are recommended by their optometrists to return for follow up care within 12-months.
While as previously mentioned there is an assumed backlog of patients who may have missed a new myopia diagnosis due to COVID-19 restrictions, it is heartening to see the average timeframe between appointments is 13 months at our Australian practices – very close to the recommended timeframe for most patients. In fact, 59% of patients who received prescriptions to treat myopia prior to June 2021 have returned for at least one follow-up appointment. This indicates that patients with known myopia are prioritising their eye health.
The rate of progression of myopia depends on many factors and can be hard to predict for an individual patient. At these review appointments, 15% of children showed no progression in either eye, and 40% had a small (less than -0.5D) progression in at least one eye. Unfortunately, just over one in three children had an increase in prescription of at least -0.5D in one or both eyes.
DISCUSSION
While we are seeing an increase in childhood myopia in our practices, and the prevalence of the condition is reportedly increasing worldwide, myopia will continue to be a hot topic in the optometric industry.
Modern lifestyles and living environments seem rife for the development of a generation of myopes who don’t spend enough time outside in fresh air, over-indexing on activities requiring near vision – especially in the past two years of pandemic-affected life.
However, it isn’t all doom and gloom. We are also living in a time of increased health literacy, of parents who pay closer attention to their children and, despite the progress still to be made, of increased access to eye care services and eyewear at a level never seen before. Due to this, unlike past generations, children with myopia in Australia and New Zealand are more likely to receive treatment leading to the condition having minimal life impact.
Specsavers is always investigating options for how its optometrists across Australia and New Zealand can best support their patients. Many Specsavers optometrists are endorsed to prescribe therapeutic agents, and several other treatment options exist for controlling progressive myopia.
As always, Specsavers is committed to industry collaboration and the sharing of its patient trends and insights to enable enhanced health outcomes for patients nationwide, so we will continue to report these through contributions to trade media including mivision, and through our data insights website www.healthhub-anz.com.
Dr Ben Ashby is the Director of Optometry Australia and New Zealand at Specsavers. He has responsibility for clinical performance, optometry professional development, professional services, and the development of clinical systems. He is actively involved in the research, development, and implementation of sustainable models of eye care delivery that improve patient outcomes and reduce avoidable blindness.
References
- Flitcroft DI, et al. IMI – Defining and classifying myopia: A proposed set of standards for clinical and epidemiologic studies. Investig Ophthalmol Vis Sci. 2019;60(3):M20-M30. doi:10.1167/iovs.18-25957
- Holden BA et al. Global Prevalence of Myopia and High Myopia and Temporal Trends from 2000 through 2050. Ophthalmology. 2016;123(5):1036-1042. doi:10.1016/j. ophtha.2016.01.006
- Fu A et al. Prevalence of myopia among disadvantaged Australian schoolchildren: A 5-year cross-sectional study. PLoS One. 2020;15(8 August):1-13. doi:10.1371/journal. pone.0238122
- French AN et al. Prevalence and 5- to 6-year incidence and progression of myopia and hyperopia in Australian schoolchildren. Ophthalmology. 2013;120(7):1482-1491. doi:10.1016/j.ophtha.2012.12.018
- Junghans BM, Crewther SG. Little evidence for an epidemic of myopia in Australian primary school children over the last 30 years. BMC Ophthalmol. 2005;5. doi:10.1186/1471-2415-5-1





