

Rodenstock has entered the market with a new myopia control lens, Rodenstock MyCon.
Launched at the beginning of April, the lens concentrates on the horizontal retina providing peripheral blur nasally and temporally to the optical centre of the lens. The peripheral blur serves to bring light to focus in front of the retina rather than behind it, reducing the reflexive eye elongation that occurs in some children.
This approach, which differs from many myopia control lenses that provide peripheral blur to all quadrants equally, has been influenced by numerous research studies.
Research-Based
Rodenstock has been a funded member of two European Union Myopia projects. Dr Anne Seidemann, the company’s research and development member, has been integral to the MyCon lens development. Dr Seidemann, who gained her PhD in myopia and peripheral refraction with Professor Frank Schaffel at Tubingen University, has a long history of myopia research. In 2002, she and Professor Schaffel showed that peripheral refraction, and assumed that peripheral eye length, varies in different parts of the retina. They published a paper suggesting, “It could even be that myopia in the periphery is a trick of nature to produce a constant inhibitory signal to prevent too much eye growth.”1
In 2013, Faria-Ribeiro et al.2 studied two groups of myopes; progressing and non-progressing. When considering the relative peripheral spherical equivalent refraction, they indicated that the progressing group had a more hyperopic peripheral refraction in the nasal hemifield, while the non-progressing group had a myopic peripheral refraction. They also noted that there was significant nasal / temporal asymmetry in the relative peripheral eye length in the non-progressing group with a longer nasal shape than temporal.
The differences between nasal and temporal retina are not limited to refraction and length. In 1990 Curcio et al.3 showed there is an anatomical asymmetry in the retina in the nasal and temporal regions. The nasal retina has a greater density of ganglion cells and greater numbers of cones. Curcio implied that this suggested a neuro-functional dominance of the nasal retina.
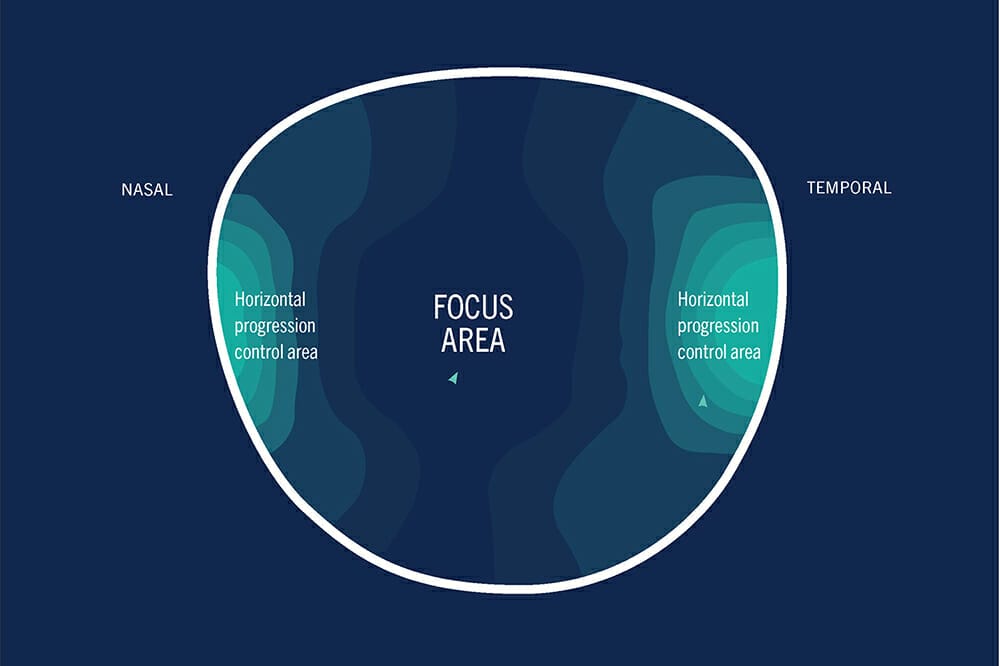
The Rodenstock MyCon lens has a central vision zone that corrects the child’s ametropia with asymmetrical nasal (+2.00D) and temporal (+2.50D) progressions, which reflect the more hyperopic nasal hemifield. (featured image).
In 2019, Tarutta et al. reported that, in a study of European children, a lens built on the same principles as MyCon4 reduced the progression of myopia by 40% over a five-year period and the axial length by 56% over two years, and 35% over five years, compared to the control group.
Lens Design
As the defocus is ground on to the surface of the MyCon lens, it is available in indexes 1.5, 1.6, 1.67, and 1.74 with an extensive power range of plano to -14.00D (combined -6.00D cyl). The lens is aspheric and so it is important for its performance that it should be fitted according to the eye rotation requirement by dropping heights by 1mm for every 2º of pantoscopic tilt.
A maximum back vertex distance of 14mm is recommended along with frame parameters that ensure that the progressions work optimally.
Leaving the superior and inferior fields without blur should make the lens easier to adapt to and the adaptation period is quoted as one to two weeks.
While there are several options for myopia management, including atropine drops and contact lenses (both soft lenses and orthokeratology), spectacle lenses remain the least invasive and often most affordable solution.
Along with the MyCon lens, Rodenstock has introduced a myopia management module to its CNXT Professional software platform. With this, it is possible to demonstrate to parents the risk of their child developing myopia based on the number of myopic parents, outdoor activities, and near vision activities conducted outside of normal school hours.
It is also possible to demonstrate how that risk will reduce if outdoor activity goes up and extra-curricular close work goes down. This is a valuable tool with which to discuss the all-important visual hygiene with both parents and children to endeavour to reduce the onset and progression of myopia.
References
1. Seidemann A., Schaeffel F., et al., Peripheral refractive errors in myopic, emmetropic, and hyperopic young subjects. J Opt Soc Am A Opt Image Sci Vis. 2002.
2. Faria-Ribeiro M., Queirós A., Lopes-Ferreira D., et al.,Peripheral refraction and retinal contour in stable and progressive myopia. Optom Vis Sci. 2013.
3. Curcio C.A., Allen K.A., Topography of ganglion cells in human retina. J Comp Neurol. 1990.
4. Tarutta E.P., Proskurina O.V., Tarasova N.A., et al., (2019) Long-term results of perifocal defocus spectacle lens correction in children with progressive myopia. Vestn Oftalmol.2019;135(5):46-53.



