

Eye care professionals (ECPs) are well placed to spot the signs of mental health challenges in patients, some of which will be associated with ocular manifestations.
As such, it is an ECP’s duty of care to take a holistic approach to providing patient care, by proactively working to identify signs of declining mental health, then recommending and advising on appropriate care and support services.
In this article, optometrists Neil Retallic and Sheena Tanna-Shah explore how we can easily adopt our best practice approach to achieve these aims as effectively as possible.
The World Health Organization (WHO) acknowledges that mental health conditions are increasing worldwide – mainly because of demographic changes – and can have a “substantial effect on all areas of life”.1 The National Study of Mental Health and Wellbeing reported that around one in five Australian adults (21.4%) experienced symptoms of a mental disorder within the past 12 months and more than two fifths (43.7%) experienced a mental disorder at some point during their lifetime.2 A New Zealand based study published similar findings, revealing that around a quarter of New Zealanders have poor health and wellbeing.3
What Is Wellbeing?
The Oxford Dictionary defines wellbeing as being ‘happy, comfortable or healthy’.4
This may be further broken down into four categories of wellbeing as follows:
• Emotional,
• Physical,
• Social, and
• Workplace.
Maslow’s theory (Figure 1), suggests basic needs must be satisfied before higher level physiological needs if we are to achieve self-fulfilment and ‘happiness’.5
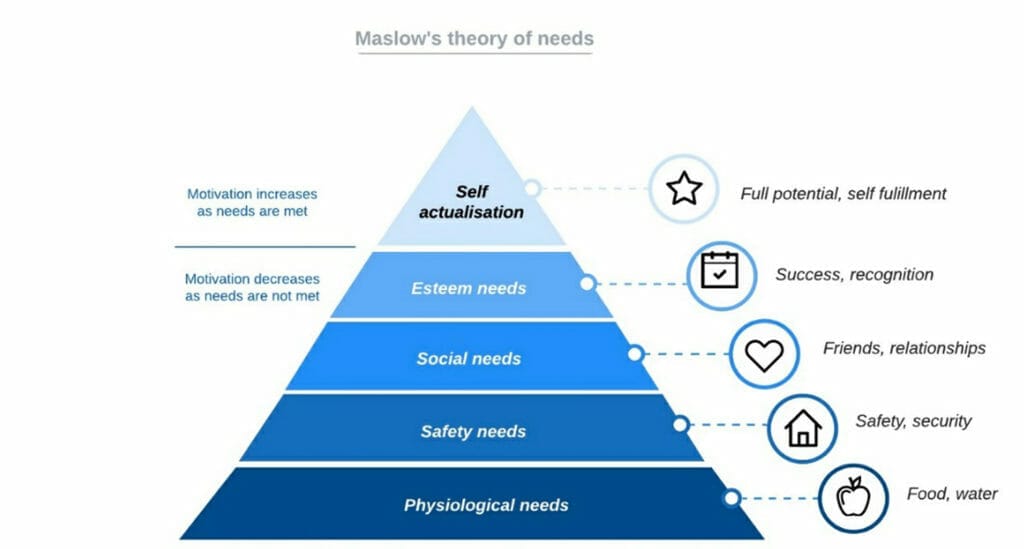
Figure 1. Maslow’s theory of needs.
A mental illness can be defined as “a clinically diagnosable disorder that significantly interferes with an individual’s cognitive, emotional, behaviour or social abilities, usually associated with distress or impairment in important areas of functioning”.1
Importantly, a person does not need to meet the criteria for a mental disorder to be negatively affected by their mental health.
Mental Health and Ocular Issues
Most emotional issues influence physical health issues, some of which (heart problems, stroke, diabetes, high blood pressure, raised cholesterol to name a few) can lead to eye problems.
Additionally, many medications used to manage depression and anxiety have been associated with ocular changes, such as tear film disruption, mydriasis, accommodative insufficiency, and increased intraocular pressure and glaucoma risk.7 The latter impact is especially important to identify in patients with narrow anterior chamber angles.
One study found a strong association of mental health issues with dry eye, with nearly half (47%) of those with dry eye reporting mental health issues.8
The ocular effects of some commonly prescribed drugs for mental health management are outlined in Table 1.
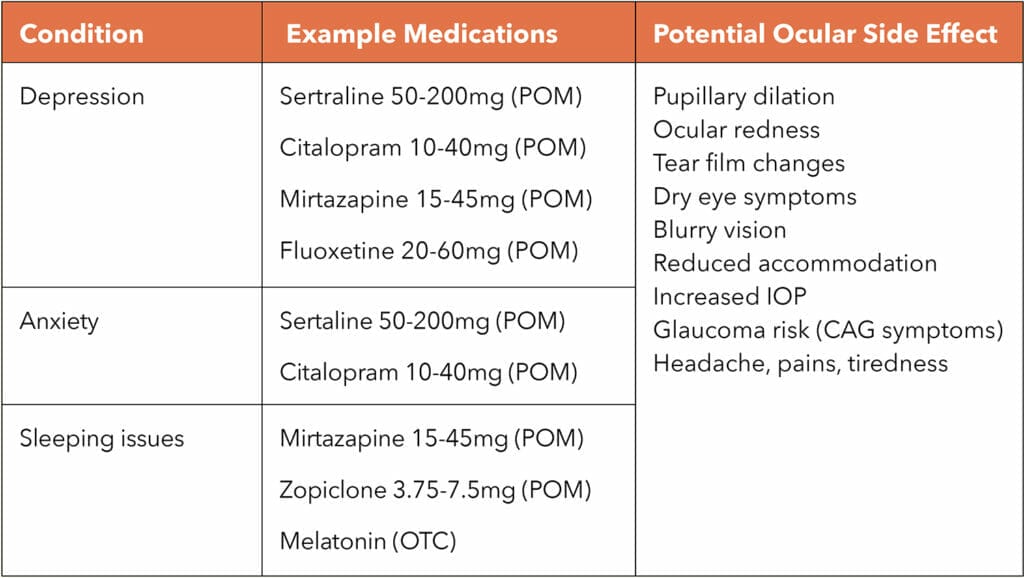
Table 1. Ocular adverse effects of some medications used for mental health.6
Identifying Signs of Poor Mental Health
As ECPs, we should avoid diagnosis, management, and treatment for conditions beyond the scope of our skill and experience. That said, as health care practitioners, we should be able to spot signs and symptoms of mental health and recommend appropriate care.
Identifying signs of compromised wellbeing starts even before the patient enters the consulting room. Careful awareness and observation of appearance, body language, posture, and the way a person generally presents themselves is useful. This is something all staff members should be comfortable undertaking as it may give vital clues as to how somebody may be feeling. Consider, for example, the following when identifying anxiety:
• Is the patient avoiding eye contact?
• Is the patient’s head hung low?
• Is the patient walking slowly or nervously?
• Is the patient fidgeting with their hands, or sweating unduly?
Communication is Key
Sometimes, all that is needed to confirm signs of compromised wellbeing is to take a couple of minutes to listen. But how do you ensure the patient in front of you feels comfortable to speak? After all, this may be the first time they have spoken to an independent professional about what they are going through.
Researchers have found that a single, quick glance of a person’s face (just 33 to 100ms) is sufficient for the viewer to form an initial impression of that person.9 This is worth remembering as patients will quickly form an opinion of you as their ECP, perhaps picking up on your mood, making a judgement of your confidence, professionalism, or authority.
To make a positive impression from the start, always greet the patient by their name and welcome them into your consulting room with a smile. Staff and practice presentation also contribute to this initial impression and help reinforce a sense of trust.
Throughout any consultation there are further opportunities to build rapport with your patients.
Things to support this include:
• Talking directly to the patient,
• Maintaining appropriate eye contact and considering your own body language,
• Actively listening and using patient-friendly language to avoid jargon or alarmist terminology,
• Mirroring tactics: for example, if the patient is using a lot of hand movements to communicate, try to do the same. If they use certain words repeatedly, then use those same words back, and
• Give encouragement throughout the consultation – but obviously avoid any implication of mimicry or mockery.
Unfortunately, we will not always be in a face-to-face consult with our patients. Telephone consultations should focus on using strong listening and questioning skills, whereas video consultations give the opportunity for body language observation.
History Taking – Identifying Risk Factors
General questions about the patient’s health and medication are an important part of history taking. Any changes since their last appointment may be reflected in low emotional or physical health.
Often, it’s possible to gauge patient wellbeing with a few simple questions, such as ‘how are you today?’ or ‘how are you feeling?’
Tailoring questions to each patient, can help you to identify further signs. For example, you could ask whether they have been able to get out much, whether they are struggling with anything, and whether they have family or other support nearby?
Asking whether your patient has been in contact with many other people is a useful question that can easily be introduced later in the history taking, for example, when asking about their occupation. If a patient with signs of declining mental health is working, ask how they are managing. If they have lost their job, ask them how they have been coping, how they are feeling about it, and whether they have any support. Changes in hobbies that reflect a resistance to socialise or interact with others can also be useful indicators of declining wellbeing.
Once a patient has been identified as experiencing mental health challenges, our role as ECPs should be concerned with prevention before cure. We can gently advise them that feelings of stress and anxiety can lead to problems with general health and eye health.
Specific advice, given confidently and based on evidence, might address healthier eating, reducing alcohol intake, improving water intake, maintaining appropriate exercise levels, connecting better with friends, family, and those with similar interests or concerns, or even the taking up of a new hobby.
We can also recommend relevant resources or provide contact details for support groups.
Importantly, we should not tell them what to do but rather, having listened to their story, we should offer ideas and resources that they may adopt and ultimately benefit from. Using phrases like, ‘I understand’ or ‘I know someone in a similar situation’ will usually help the patient feel they are understood and not alone in their circumstance or situation. This may also help them feel more confident about taking up some of your suggestions.
Figure 2 presents opportunities to identify and discuss issues related to wellbeing at various stages of the eye examination.
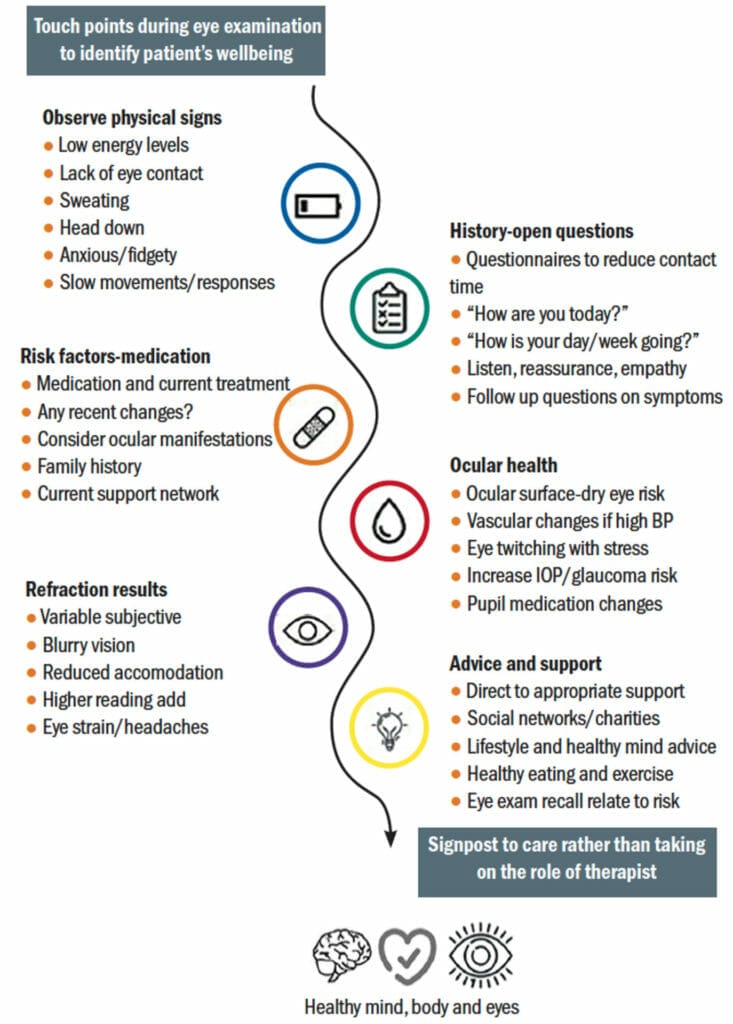
Figure 2. Touch points during a routine eye examination for consideration of mental wellbeing.10
Management Options
The mind and body are intricate and complicated yet interlinked. Each can impact on the other. As ECPs, we cannot directly treat mental health conditions, but we can support patients by offering suitable recommendations, resources, and options. An overview of management strategies is presented in Figure 3.

Figure 3. Management options for health and wellbeing.10
Understanding what mental health specific services are available in your area is useful. The Health Direct website (healthdirect.gov.au/australian-mental-health-services) and the Mental Health Foundation of New Zealand website (mentalhealth.org.nz/) provide an overview of support services and pathways, where appropriate, to funded care.
Case Scenarios
The following two cases demonstrate the difference an ECP can make to a patient’s life with appropriate intervention.
Case One
When a young mother presented for an eye examination, her constant avoidance and lack of eye contact suggested she was feeling withdrawn and lacked confidence. She mentioned she was struggling with her work/life balance and greatly missed socialising since having her baby. She admitted to being constantly stressed, tired, and feeling a ‘lack of support’. She had spoken to a pharmacist about sleeping problems and since then, had been taking sleeping tablets most evenings, with mixed success. She was experiencing sporadic headaches but had no visual or ocular signs upon examination.
Management: In this case, the priority was to listen, give encouragement, offer lifestyle recommendations and general support. Starting with small steps, such as setting simple goals, can be a useful motivator to change habits and develop new routines.
Outcome: The patient’s mood appeared elevated after being able to discuss her problems in a safe, independent environment. She left feeling more positive. At a follow-up contact lens appointment a few weeks later, she thanked the ECP and said she was now managing to make time for exercise and better nutrition. Using a fitness app, that she had downloaded free on her phone and linked to her watch, she was enjoying monitoring her progress.
Mental Health organisations available to support young adults in Australia and New Zealand are:
• Orygen: www.orygen.org.au
• Beyond Blue: beyondblue.org.au
• Lifeline: lifeline.org.au and lifeline.org.nz
• R U OK?: ruok.org.au and areyouok.org.nz
• Black Dog Institute: blackdoginstitute.org.au
• ReachOut: au.reachout.com
• Headspace: headspace.org.au
• Gather My Crew: gathermycrew.org.au
• Youthline NZ: www.youthline.co.nz
• Anxiety NZ: anxiety.org.nz
Case Two
During his eye examination, a vulnerable 80-year-old man with diabetes mentioned that he was feeling quite alone and isolated. He no longer went out (today was a first for a long time) and had minimal contact with his family. His vision was reduced, dry eye was observed, and he had a background of diabetic retinopathy.
Management: After discussing the relevant local support and resources available, the ECP took the opportunity to discuss nutrition, the importance of stability for diabetes control, some general points about eye health and retinal screening, and dry eye management. He set a daily target of going for a short walk.
Outcome: The patient left feeling more self-confident and looking forward to doing some ‘extra healthy’ food shopping. He also planned to contact some of the support networks available, with the aim of becoming involved in local activities and to increase his social circle. A follow-up call confirmed he had maintained going for short regular walks and started a food diary. His efforts had resulted in an improvement in his diabetic control.
Available support services for this patient include:
• Diabetic online support groups (New Zealand) Diabetes New Zealand
• Diabetic support group (Australia) www.diabetesaustralia.com.au
• Community Support Groups / Mental Health Foundation
• Mental health services and programs for older people – Services and programs (nsw.gov.au)
Predicting Patients With Poor Wellbeing
Although the prevalence of poor wellbeing increases with certain risk factors, it can also impact those who are extremely fit and healthy. A meta-analysis found the mental health symptoms and disorders in current elite athletes ranged from 19% for distress to 34% for anxiety/depression, and for former elite athletes from 16% for distress to 26% for anxiety/depression.11
While The National Health Survey revealed that children had the lowest prevalence of mental or behaviour conditions, the incidence was still 13% for Australian children in the age group 0–14 years old.2
Recently, paediatricians have reported a rise in children presenting with health-related issues, some of which have ocular manifestations. Ocular signs in children can include new ocular tics (short infrequent bursts of involuntary uncontrolled eye movements), of which an underlying neurological cause can be ruled out by the absence of other typical indicators of neurological disease.
These cases are likely to be induced by a heightened emotional state, for example stress or anxiety. Ocular symptoms in children, such as headaches with or without visual disturbance, may also become manifest. Identifying potential triggers, such as bullying at school, adopting a reassuring communication style that involves both the child and parent/carer, and highlighting (where appropriate), available community support services, can make a real difference beyond simply providing the usual visual correction eyewear solutions.12
To help gauge a child’s emotional state, a simple traffic light system can be applied (where red represents feeling angry, yellow is bothered and green is calm). Another self-monitoring tool is measuring healthy days throughout the month (Figure 4). Recording their emotional state each day using emojis (healthy day, unhealthy day-physical or unhealthy day-mental) on a calendar, can help build a picture of their mental status over time. ‘Healthy days’ estimate the number of recent days when a person’s physical and mental health was good (or better) and is calculated by subtracting the number of unhealthy days from 30 days.
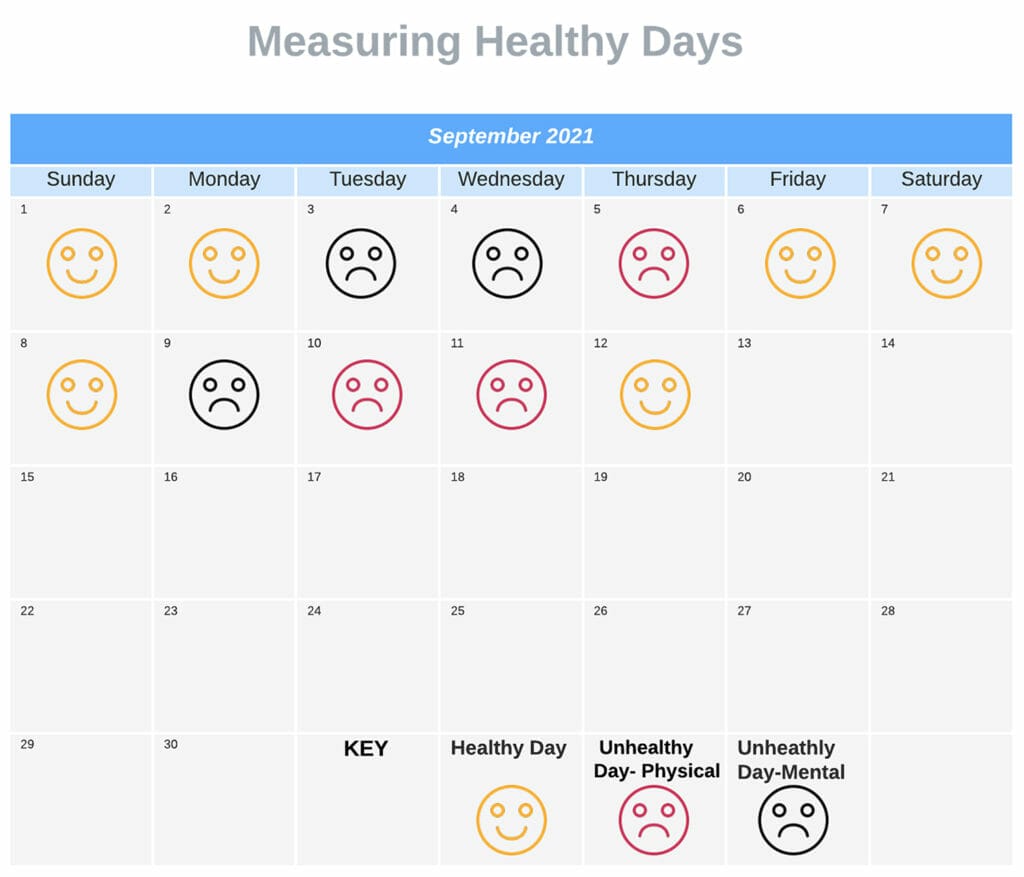
Figure 4. Simple self-monitoring assessment.
Maintaining Our Own Mental Health
As well as looking out for symptoms of mental health issues in patients, it is important that we remain alert to our own health and wellbeing, and to that of our colleagues. A recent survey found that nearly a third of Australian optometrists are struggling with their mental health. One in four practitioners had taken the brave step to consult a health professional about their mental health issue and one in five (21%) had actively received medication and/or counselling. In fact, mental health conditions and burnout among Australian optometrists were higher than other health professionals and the general population.13
Conclusion
Initially, it may seem easier to avoid asking patients questions about their wellbeing for fear of opening ‘a can of worms’. However, if you can change your mindset to view these questions as an essential service in the best interest of the patient, you may become more open to it.
Like all new things, it can seem a bit daunting but by embracing this as your new routine, you may find your role as an eye care professional becomes even more rewarding.
We should also reflect on our own wellbeing and consider how we come across to others.
If there is an opportunity to support and be the difference in a patient’s life, why would you not take it?
This article is adapted from an article originally published in Optician.
 Neil Retallic is an optometrist with experience working in practice, education, industry, and head office roles. He currently works for Specsavers and the College of Optometrists in the United Kingdom. He has been involved with various organisations across the sector and is currently President of the British Contact Lens Association
Neil Retallic is an optometrist with experience working in practice, education, industry, and head office roles. He currently works for Specsavers and the College of Optometrists in the United Kingdom. He has been involved with various organisations across the sector and is currently President of the British Contact Lens Association

Sheena Tanna-Shah is an optometrist working in practice. She is also an author, rapid transformation therapy practitioner, life coach, mindfulness, meditation, NLP practitioner, and nutritionist.
References
1. World Health Organization, Mental Health, who.int/health-topics/mental-health#tab=tab_1 [accessed19 March 2023].
2. Australian Bureau of Statistics, National Health and Wellbeing Study (2022), available at: abs.gov.au/statistics/health/mental-health/national-study-mental-health-and-wellbeing/latest-release [accessed 19 March 2023].
3. Mental Health Foundations, Wellbeing amongst New Zealanders (2021), available at: mentalhealth.org.nz/resources/resource/well-being-amongst-new-zealanders [accessed 19 March 2023].
4. Oxford English Dictionary 3rd edition: Oxford University Press, 2010.
5. Maslow, A.H., (1943). A theory of human motivation. Psychological Review. 50 (4): 370–96.
6. Richa S., Yazbek J.C., Ocular adverse effects of common psychotropic agents. CNS Drugs. 2010;24(6):501–26.
7. Gherghel D., Ocular side effects of system drugs 3 – central nervous system agents. Optician, 22 May 2020;18–22.
8. Hossain P., et al., 2021 Patient-reported burden of dry eye disease in the UK: a cross-sectional web-based survey. BMJ Open 2021.
9. South Palomares J.K., Young A.W., Facial first impressions of partner preference traits: trustworthiness, status, and attractiveness. Social Psychological and Personality Science. 2018;9(8):990–1000.
10. Retallic N., Shah S., Health and well-being in eye care practice. Optician.15 Jan 2021; 17-21.
11. Gouttebarge V., et al., Occurrence of mental health symptoms and disorders in current and former elite athletes: a systematic review and meta-analysis. Br J Sports Med. 2019 Jun;53(11):700–706.
12. Raj C. Paediatric eye care in the post-pandemic era. Mivision. February 2023; (186): 69–72.
13. Bentley S.A., et al. The mental health and wellbeing survey of Australian optometrists. Ophthalmic Physiol Opt.2021 Jul;41(4):798–807.





