

Patients neglect to seek medical care for many reasons – culture can be one of the most influential barriers. Health care professionals with an insight into the cultural attitudes, behaviours, and beliefs of the patients who walk through their doors can adapt their management style to suit. Dr Christolyn Raj writes that when it comes to diagnosing and managing those with diabetic retinopathy and maculopathy, culturally competent support services can make a meaningful difference to visual outcomes.
The term ‘culture’ is varied in its definition. In the provision of healthcare, over the past two decades it has become the key to offering patient-centred care that returns the most positive clinical outcomes.
While we commonly think of culturally appropriate services as those meeting the needs of our diverse ethnic population, it is much more than that. Culturally competent care is defined as care that respects diversity in the patient population.1 This diversity may take the form of a different racial or ethnic background, a range of beliefs or traditions common to a subgroup, as well as cultural factors that can impact on health management, including language, communication styles, attitudes, beliefs, and behaviours.
Cultural awareness also needs to take into account all demographics, including Indigenous and non-Indigenous status, LGBTQ+ (lesbian, gay, bisexual, transgender, queer or questioning, or another diverse gender identity) and numerous refugee communities.
As optometrists and ophthalmologists in Australia and New Zealand, is this clinically relevant to our practice?
Yes. In fact, it is more relevant that we probably think.
One of the most common areas of chronic eye disease affected by the cultural divide is diabetic retinopathy (DR).
There are many studies suggesting an increased morbidity of diabetic eye disease, with irreversible adverse outcomes, in certain cultural subgroups in Australia. To reverse this trend, we all must strive to incorporate culture into our assessment and management of patients, especially those who present with chronic eye disease.
Impact On Chronic Disease
The total number of people with diabetes worldwide is projected to reach 366 million in 2030. Type 2 diabetes is fast becoming more predominant subset, estimated by the World Health Organization (WHO) to reach 300 million by 2025.2
Race and ethnicity are considered risk factors for both type 1 and type 2 diabetes.
While studies vary in their reports on disease prevalence among certain ethnic groups, there is clear evidence to support the increased prevalence of diabetic maculopathy, also known as diabetic macular oedema (DMO), in Indigenous compared to non-Indigenous patients.
Furthermore, three epidemiological Australian studies report a prevalence of DMO as high as 8.9%.3–5 Another study found that the prevalence of DMO was 1.5 times higher in this subgroup.6 In stark comparison, the estimated prevalence of DMO in non-Indigenous Australians varies in reported literature, but is estimated to be in the lower ranges from 3.3% to 5.6% (Figure 1).6,7

Figure 1. Prevalence of diabetic eye disease in Indigenous vs non-ndigenous subgroups based on epidemiological studies 2002–2010. AusDIAB(Tapp 2003) Australian diabetes, obesity and lifestyle study: non-Indigenous participants Durkin (2006),3 Landers (2010),4 Xie (2011): Indigenous participants.1
DR is more common among some ethnic groups than others. Figure 2 provides some insight into the prevalence of DR and maculopathy per ethnicity in a United States-based study.8 Vision-threatening DR was more prevalent in African Americans with type 2 diabetes, followed by Hispanic subgroups. It was noted to be lower in Asian and white subgroups. The increased prevalence and severity of the disease in some ethnicities may be explained by underlying diet, lifestyle, and systemic risk factors, as well as genetic predisposition, however the latter is poorly understood.8
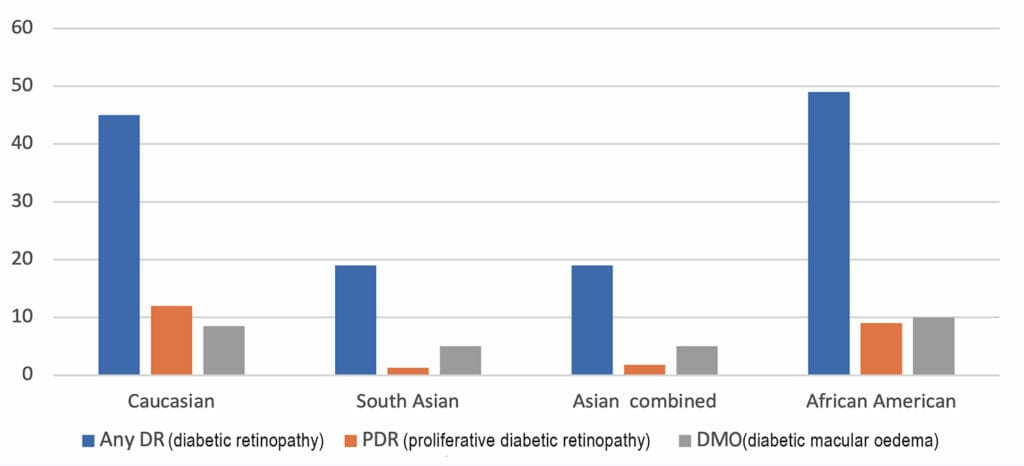
Figure 2. Prevalence of diabetic retinopathy in patients according to race/ethnicity. Percentages (95% confidence interval) for individuals with diabetes aged 20–79 years.8
There is no doubt that the uneven distribution of morbidity of diabetic eye disease in the above subgroups is due, in part, to inherent barriers to accessing culturally appropriate services. While these are numerous, several common factors identified are uncertainty about access, cultural beliefs, trust in the health system, communication/language, costs, and an inability to identify within the system (Figure 3).9 As a consequence of these barriers, patients may often present late in the disease process, even on their initial presentation.

Figure 3. Schematic representation of cultural barriers to accessing healthcare.
As a result, a complex management plan is usually required. This can be confusing to a patient’s understanding of ‘curing’ the disease. Subsequently many patients can be reluctant to complete their treatment with the unfortunate result being irreversible blindness.
Overcoming these barriers is the key to preventing disease progression in these patients.
Impact On Screening And Disease Progression
The Global Diabetic Retinopathy Project Group developed an internationally recognized classification for DR referred to as the International Clinical Disease Severity Scale (Table 1).10 In this classification scale there are five levels of DR severity: none, mild, moderate, severe, and proliferative in the presence or absence of diabetic maculopathy.10
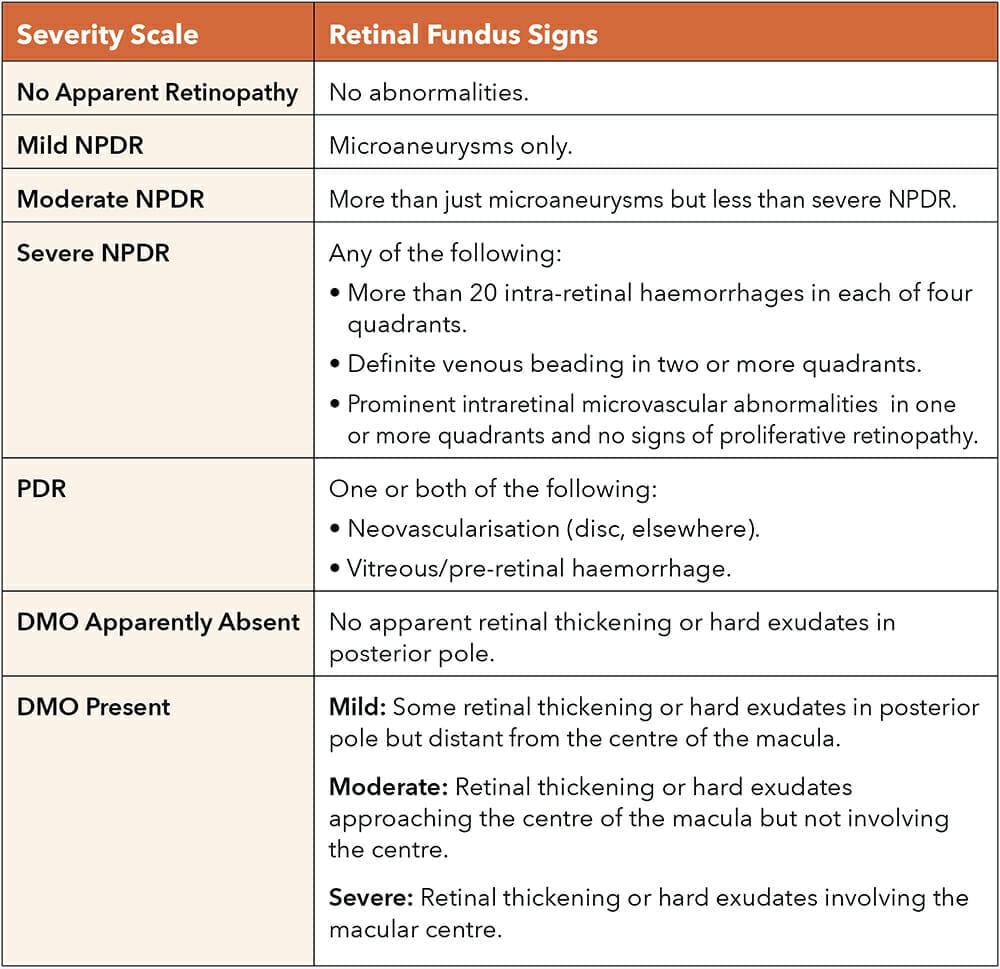
Table 1. The International Clinical Disease Severity Scale.10
While being a good universal classification, this severity scale needs to be interpreted with some caution.
This is particularly the case when assessing diabetic severity and, more importantly, the risk of progression in certain patients including those from Indigenous backgrounds, as well as some ethnic populations such as Pacific Islanders, Asian and Indian sub-continental populations.
Due to several factors, many of these patients will exhibit a spectrum of severe DR/ maculopathy on their first presentation to an eye care professional (Figure 4). We need to appreciate this, so that we can accurately triage these patients.

Figure 4. Common initial presentations of severe diabetic retinopathy in some subgroups. (A) Retinal fundus photograph (right eye) showing neovascularisation at the optic disc (NVD). (B) Retinal fundus photograph (left eye) showing NVD and regressed NVD at the optic disc in an ischemic appearing retina. (C) Fundus fluorescein angiogram (FFA) showing active vitreous haemorrhage and several areas of neovascularisation (hyperfluoresence).
We also need to appreciate that they may not follow the severity classification stages that we expect; moreover they could quickly progress from the mild non-proliferative to the proliferative phase. These patients need a timely referral for a definitive management strategy to halt disease progression.
Culture As A Clue to Severe Disease Presentation
Recent studies on the uptake of other screening programs, such as colorectal screening among various ethnicities, show the poorest uptake in ethnic minorities.11
In Indian sub-continental and some Asian cultures, screening is not a readily understood or accepted concept. Presenting for screening or routine review may also be downplayed in these cultures due to associated negative connotations, like lack of stoicism.
Consequently, patients only present when they are symptomatic which, in the case of diabetic eye disease, is often when they have developed severe vision-threatening disease.
Cultural values and beliefs can also affect disease progression in DR. In some Middle Eastern cultures for example, there is an increased reliance on breads and carbohydrates that carry a high glycaemic index. High glycaemic foods can cause fluctuations in blood sugar levels, impacting on overall diabetic control. The glycaemic control of patients with diabetes can also be detrimentally affected in cultures that observe periods of fasting. Several studies support the theory that subgroups such as Afro-Caribbean, Pacific Islander, and Indigenous Australians have inherent cardiovascular risk factors (obesity, smoking, dyslipidemia, and kidney disease), all of which can exacerbate progression of DR.12,13
Visual Requirements Transcend Culture
As eye care professionals, we are in a fortunate position in that our patients who present with compromised vision are motivated to listen and adhere to management advice.
To make the most of this valuable opportunity, we need to ensure that our management advice is provided in a manner that is culturally acceptable to them.
When it comes to managing DR, this can only be achieved with a multidisciplinary team inclusive of a patient-centred family doctor, a dietician who is well-versed on ethnic and cultural dietary requirements, and an endocrinologist who understands that glycaemic targets need to be patient specific.
Of course ongoing collaboration between the optometrist and ophthalmologist is paramount here.
It is important to be completely transparent with the facts. Patients with eye disease need to understand that they are in the ‘vision-threatening subgroup’ where, if certain changes aren’t made, they will lose valuable sight that is irretrievable. To ensure this message can be readily understood, it is useful to use pictorials, brochures and even videos that are commonly available in several languages.
One of the most challenging aspects to communicate is the goal of treatment. While in many cases we aim for some improvement in vision, in moderate to severe retinopathy only modest improvements will be possible. However, the ultimate goal is to prevent further deterioration and prevent complications.
It is also important to outline a proposed management timeline so that patients can plan and appreciate that there is an end point to treatment. This is more likely to engage patients in their management and improve attendance to appointments.
Although patients may be culturally and ethnically distinct, by employing the above methods in our initial management we can speak the same language to encourage their participation.
Further patient participation can be encouraged through ethnic community groups, local council co-operatives and Aboriginal Area Health Service Centres. Each of these groups can be a great source of information for patients, with culturally appropriate literature and multimedia, including bilingual medical booklets, bilingual recipe books and videos to optimise diabetic control, community activities and social events, as well as local support groups.14,15
The Way Forward
So what does it mean to be culturally competent?
Hopefully this article has shed some light on the factors of cultural awareness that exclusively affect us when managing patients with diabetic eye disease.
By appreciating that certain cultural subgroups are at higher risk of ‘vision-threatening’ disease than others and that they require more cautious triage, we can institute timely management. In doing so, we can make a real difference to improving the morbidity of this disease.
Importantly, this type of management needs to be patient specific and can only truly be achieved through a well-connected health network.
Current studies in DR are now looking at protective factors to prevent the onset of diabetic eye disease. We can only hope that future studies will further investigate how culture plays an important part in this scenario, in an attempt to reduce the prevalence of this debilitating condition in our community.
Dr Christolyn Raj MBBS(Hons) MMED MPH FRANZCO is a Melbourne-based ophthalmologist with a special interest in retinal disease. She is a published author and peer reviewer for several scientific journals. Dr Raj heads a retinal injection clinic at Camberwell, Blackburn, and Coburg, and is responsible for the surgical management of patients with cataract and comorbid retinal disease. She is currently undertaking active research projects in affiliation with her retinal clinics and the University of Melbourne, in surgical management of patients presenting with cataract in the context of diabetic eye disease.
References
1. White, J., Plompen, T., Tao, L., et al., What is needed in culturally competent healthcare systems? A qualitative exploration of culturally diverse patients and professional interpreters in an Australian healthcare setting. BMC Public Health 19, 1096 (2019). doi.org/10.1186/s12889-019-7378-9.
2. Wild, S., Roglic, G., Green, A., et al. Global prevalence of diabetes, estimates for the year 2000 and projections for 2030. Diabetes Care 27:1047–1053, 2004.
3. Durkin, S.R., Casson, R., Newland, H.S., Selva D., 2006, Prevalence of trachoma and diabetes- related eye disease among a cohort of adult Aboriginal patients screened over the period 1999-2004 in remote South Australia. Clin Experiment Ophthalmol; 34: 329–334.
4. Landers, J., Henderson, T., Abhary, S., Craig, J., 2010. Prevalence and associations of diabetic retinopathy in Indigenous Australians within central Australia: The Central Australian Ocular Health Study. Clin Experiment Ophthalmol 38: 393–397.
5. Xie, J., Arnold, A.L., Keeffe, J., et al. 2011, Prevalence of self-reported diabetes and diabetic retinopathy in Indigenous Australians: The National Indigenous Eye Health Survey. Clinical & Experimental Ophthalmology 39: 487–493.
6. Kaidonis, G., Mills, R., Landers, J., et al. 2014, Review of the prevalence of diabetic retinopathy in Indigenous Australians, Clinical & Experimental Ophthalmology.
7. Dirani, M., Shaw, J., Crowston, J., 2013, Out of sight: A report into diabetic eye disease in Australia, A report for Baker IDI.
8. Yau, J.W., Rogers, S.L., Kawasaki, R., et al. 2012, Global prevalence and major risk factors of diabetic retinopathy. Diabetes Care 35:556–564.
9. Australian Institute of Health and Welfare, 2015. Risk factors, diseases and deaths in diabetes among populations of interest. Canberra: AIHW. aihw.gov.au/diabetes/populations-of-interest.
10. Wilkinson, C.P., Ferris, F.L., Klein, R.E., et al. Global diabetic retinopathy project group, 2003. Proposed international clinical diabetic retinopathy and diabetic macular edema disease severity scales. Ophthalmology. 110(9):1677–82.
11. Sekhon, H.K., Lal, N., Majeed, A., et al. Ethnic disparities in the uptake of colorectal cancer screening: An analysis of the West London population. Colorectal Dis. 2021 Jul;23(7):1804–1813.
12. Jaross, N., Ryan, P., Newland, H., 2005, Incidence and progression of diabetic retinopathy in an Aboriginal Australian population: Results from the Katherine Region Diabetic Retinopathy Study (KRDRS). Report no. 2. Clinical & Experimental Ophthalmology. 33(1):26–33.
13. Simmons, D., Clover, G., Hope, C., 2007, Ethnic differences in diabetic retinopathy. Diabet Med 24: 1093–1098.
14. Livingston, P.M., McCarty, C.A., Wood, C.A., et al., Use of focus groups to identify health promotion strategies for the early detection of diabetic retinopathy. Aust NZ J Public Health. 22(2):220–2.
15. Diabetes Qualified Pty Ltd 2022: diabetesqualified.com.au/resource/fact-sheets [accessed 10 May 2023].





