
Findings from a study examining the clinical validity of Melbourne Rapid Field (MRF) vision test, by comparing this technology with existing devices, have been presented as a Poster by Associate Professor George Kong at the World Glaucoma Congress 2023 (WGC23) in Rome.
Vision testing is essential to detect and manage glaucoma, however standard perimetry is neither widely available or easily accessible. This means patients often do not perform visual field tests frequently enough to allow early detection of progressing disease.
MRF was developed to make perimetry inexpensive, easy to do, readily accessible, and to potentially allow patients to perform the test at home.
A recent study showed a good level of agreement between MRF Web-browser software and the clinical gold standard Humphrey Field Analyzer (HFA) 24-2 SITA Standard.1 However, this study did not compare the MRF Web-browser (MRFweb) software with the newer 24-2 SITA-Faster (SITAfr) algorithm.
Assoc Prof Kong and colleagues, Professor Algis Vingrys and PhD candidate Selwyn Prea, undertook a further study to examine clinical validity of the MRF-web. Using the MRF-web browser application with a desktop computer interfaced to an LG 27-inch screen as the display, the study compared outcomes from tests with the same patients performed in clinic using a Humphrey Field Analyser 24-2 SITAfr, typically six months prior.
Participants were introduced to the MRF test procedure with a 30 second practice run. To test peripheral locations, audio instructions requested that patients fixate centrally and follow the fixation target to the corners of the screen as the test progressed. Patients were asked to respond to the presence of a spot by tapping the laptop keyboard.
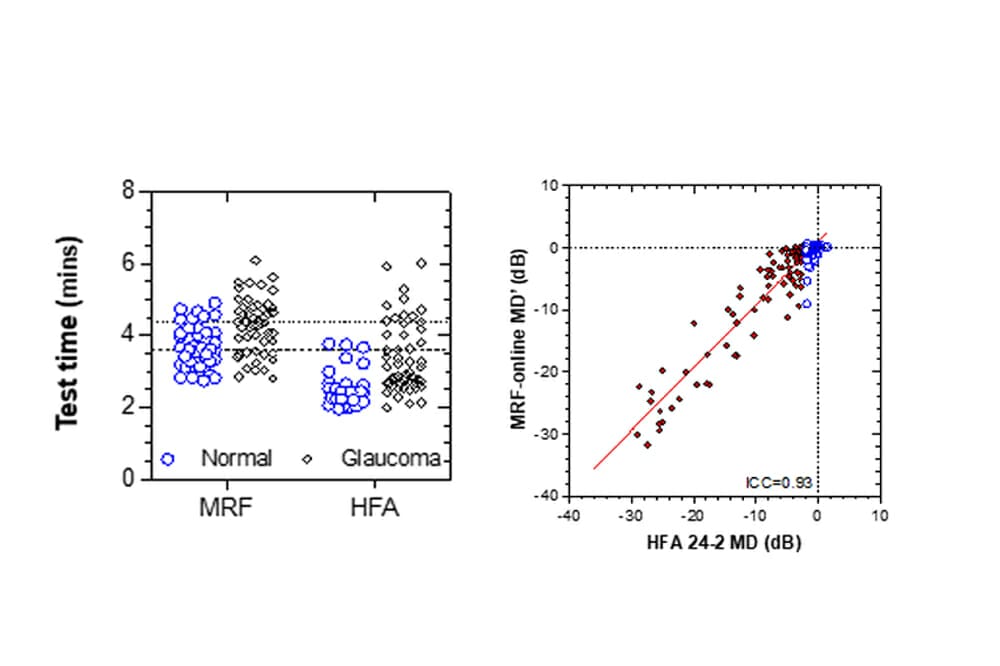
“We tested 90 glaucoma or glaucoma suspect patients (178 eyes). Participants had an average age of 60.5 (range 21 to 92 years). Seventy-two eyes had normal HFA mean deviation (MD) (>-2 decibels [dB]); 66 had early loss (-2<MD>-6 dB) and 40 had moderate (-6>MD<-12, n=13), advanced (-12>MD<-20, n=13) or severe defects (-20>MD, n=14) at the last SITAfr result. MRF MD values were expressed as a HFA equivalent MD (MD’) by correcting for spot size differences.
Assoc Prof Kong and his team reported that both MRF-web and HFA SITAfr took approximately one minute longer to test glaucoma patients compared with normal patients. Additionally, MRF-web needed about one minute longer due to the fact that it tests for patient reliability.
A high level of concordance was found between MRF MD’ and the MD of HFA SITAfr (ICC = 0.93). After allowing for spot size differences, the MRF returned MD outcomes that aligned very closely with those of HFA SITAfr.
Assoc Prof Kong concluded that while slower, the MRF-web application can be used in the clinical setting with high agreement with SITAfr to provide reliable and accurate visual field thresholds.
“It is easy to use, requires minimal clinical space, is affordable, and scalable across multiple devices and across multiple clinics,” commented Assoc Prof Kong.
He said the potential of the MRF-web to enable home monitoring of visual fields by patients with glaucoma is now being actively examined, supported by a research fund from the auDA foundation.
Reference
1. Aslam T.M., Murray I.J., Lai M.Y., et al., An assessment of a modern touch-screen tablet computer with reference to core physical characteristics necessary for clinical vision testing. J R Soc Interface. 8 May 2013;10(84):20130239.


