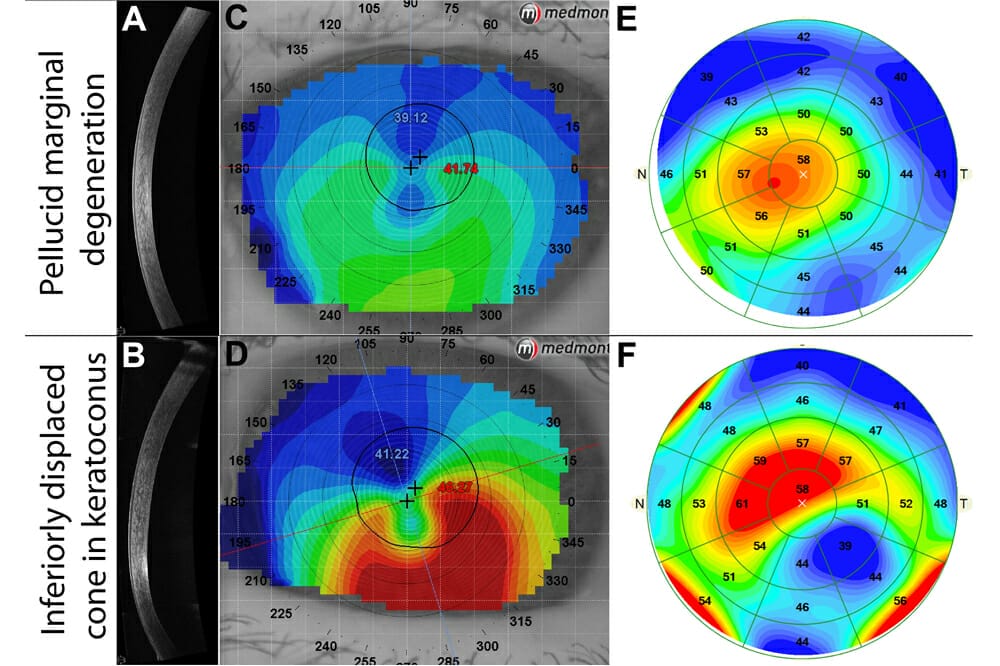
Figure 1. An example of a patient with early pellucid marginal degeneration (top) and a patient with keratoconus (bottom). (A–B) Single vertical AS-OCT line scans. (C–D) Corneal topography using the Medmont E300 topographer. (E–F) Epithelial thickness maps derived from AS-OCT.
Optical coherence tomography (OCT) provides non-invasive, high-resolution, cross-sectional visualisation of anterior and posterior structures.1 While this unique capability has made it an integral component of eye examinations for common clinical presentations, such as glaucoma or macular disease,2 the technology also offers other advantages in less conventional applications.
In this article, Henrietta Wang discusses three practical but ‘unconventional’ OCT applications and provides real-life scenarios where unconventional use of OCT can help guide optometric management of patients.
Unconventional Use #1: Qualitative and Quantitative Epithelium Examination
Although OCT was initially developed to provide an extra dimension to evaluation of the posterior segment,1 in more recent years there has been a proliferation of OCT applications for the anterior segment.3
Anterior segment applications of OCT can be broadly broken down into two categories: qualitative and quantitative. As anterior segment OCT (AS-OCT) outputs are highly comparable to tissue histology,4 AS-OCT offers a non-invasive method for qualitatively evaluating ocular structures.
For example, despite being histologically distinguishable, differentiating ocular surface squamous neoplasia (OSSN) from pterygium using slit lamp biomicroscopy alone is extremely challenging.5 By reviewing AS-OCT line scans through the lesion and assessing for features diagnostic of OSSN, such as the presence of hypo-reflective spaces associated with reduced epithelium reflectivity, or increased thickness of the epithelium as well as a steep transition zone from affected to normal epithelium, clinicians can more accurately differentiate between the two clinical entities.5,6
While qualitative AS-OCT can assist in the diagnosis of ‘lesion-based’ corneal disease, its utility is limited when it comes to corneal disease without distinguishing features, such as the various phenotypes of corneal ectasia. In these instances, imaging modalities that characterise the corneal profile using quantitative outputs, such as Placido disc or Scheimpflug principle corneal topography, may be more appropriate.7–9
More recently, there has been emerging evidence for the use of quantitative ASOCT outputs, such as full pachymetric or epithelial thickness maps in evaluating corneal ectasia.10,11 For example, the differentiation of pellucid marginal degeneration and inferior keratoconus can be difficult when relying on topography or qualitative OCT alone.12 Although these both fall under the category of corneal ectasia, they carry very different prognoses whereby keratoconus progression typically ceases in the 30–40s,13 while pellucid marginal degeneration remains progressive.14 In keratoconus, there is epithelial remodeling overlying the region of ectasia, which manifests as epithelial thinning on AS-OCT epithelial thickness maps.15 On the other hand, epithelial thickness is typically normal in pellucid marginal degeneration.16
Figure 1 contrasts a patient with inferior keratoconus and one with pellucid marginal degeneration. Vertical qualitative AS-OCT line scans through the cornea show inferior thinning of the cornea in both patients (Figures 1A and B). Both corneal topography maps show an inferior ‘crab-claw’-like pattern (Figures 1C and D), however the epithelial thickness maps show normal epithelial thickness overlying the area of ectasia in the patient with pellucid marginal degeneration (Figure 1E), while marked epithelial thinning is noted overlying the region of ectasia in the patient with keratoconus (Figure 1F). These case examples highlight the value of obtaining epithelial thickness maps using AS-OCT when examining patients with corneal ectasia.
In addition to differentiating between topographically-similar corneal ectasia, AS-OCT epithelial thickness maps can also be used in detecting sub-clinical or early keratoconus.10 This is of particular importance as a pre-screening tool for refractive surgery to identify patients at risk of developing iatrogenic post-LASIK ectasia. While qualitative AS-OCT can help clinicians with diagnosing patients with ‘lesion-based’ corneal disease,3 quantitative AS-OCT can also be applied to help clinicians phenotype and identify sub-clinical cases of corneal ectasia.16
Unconventional Use #2: Looking Beyond Visible Angle Structures
While gonioscopy remains the gold standard for evaluating the anterior chamber angle, AS-OCT has gained increasing popularity as it offers a non-invasive method for visualising the anterior chamber and angle.17
Despite the development of several AS-OCT parameters for characterising the angle, a major limitation of AS-OCT in guiding management of narrow angle patients is its inability to visualise the pigmented trabecular meshwork, a key structure in assessing for iridotrabecular contact.18
Unlike subjective reporting of gonioscopic findings, AS-OCT provides a snapshot of the interactions between the iris, ciliary body, and cornea, which is particularly relevant in narrow angles.19 In particular, this allows for prediction of angle morphology and assessment of the iris contour.20 For example, although the formal diagnosis of plateau iris configuration is dependent on ultrasound biomicroscopy, AS-OCT offers high-resolution viewing of the iris root, surface, and angle structures that can provide a clue regarding risk of plateau.21 Careful differentiation between plateau and non-plateau iris configuration is key for determining the most appropriate form of intervention to maximise treatment success (i.e. laser peripheral iridotomy versus iridectomy).22 An example of a plateau iris configuration is shown in Figure 2A.
In addition to characterising angle morphology, AS-OCT can also be used to examine the iris-lens relationship. For example, lens vault is an emerging new AS-OCT-based parameter in assessing narrow angles.23,24 Lens vault is defined as the distance between the plane of the scleral spur and the most anterior point of the lens.23 Previous work has shown the phacomorphic phenotype of glaucoma to be associated with a greater lens vault.25 Similar to differentiating between plateau and non-plateau iris configurations, it is also important for clinicians to be able to distinguish between phacomorphic and non-phacomorphic angle closure as patients with a phacomorphic component may benefit from lens extraction as first-line therapy instead of starting with a laser peripheral iridotomy.26 An example of a patient with a phacomorphic angle configuration is shown in Figure 2B.

Figure 2. An example of (A) a patient with plateau iris configuration, and (B) a phacomorphic configuration.
In addition to understanding the angle configuration, new novel AS-OCT parameters, such as the iris shape or concavity can also help predict treatment success following laser peripheral iridotomies.27 As the iris tends to flatten following laser peripheral iridotomy, greater initial iris concavity has been associated with a greater chance of success following treatment.28 Beyond allowing for binarised classification of angle status (i.e. open versus closed),29 examining the iris-lens in conjunction with the iris-cornea relationship using AS-OCT can be used to phenotype narrow angles and guide recommendations for appropriate treatment options.
Unconventional Use #3: Assessing the Peripheral Retina
Traditionally, the peripheral retina is evaluated in an en face manner using funduscopy or binocular indirect ophthalmoscopy.30 A major limitation of assessing the peripheral retinal funduscopically is the lack of a three-dimensional view as pathologies with very different prognoses can present similarly funduscopically.31 It is also well known that stereopsis32 and field of view33 are significantly reduced when examining the periphery using clinical techniques.
Peripheral OCT can add an extra dimension to assessment of the peripheral retina in several ways. Firstly, management of peripheral retinal pathology is often based on the presence or absence of prognostic features.34 One such example is the detection of a fluid cuff around a retinal hole. Figure 3A shows an example of a patient with an operculated retinal hole that was noted to have an associated fluid cuff based on ultra-widefield imaging. Interestingly, as peripheral OCT line scans through the hole showed no associated fluid around the hole (Figure 3B), this patient could be safely monitored with biannual dilated fundus examinations and onward referral for prophylactic laser retinopexy was not indicated.

Figure 1. An example of a patient with early pellucid marginal degeneration (top) and a patient with keratoconus (bottom). (A–B) Single vertical AS-OCT line scans. (C–D) Corneal topography using the Medmont E300 topographer. (E–F) Epithelial thickness maps derived from AS-OCT.
Secondly, in addition to guiding risk stratification in patients with peripheral pathology, OCT can also be used to detect features that cannot be funduscopically visualised. For example, previous work has shown microstructural changes, such as marked vitreoretinal traction or subretinal fluid associated with lattice degeneration may benefit from prophylactic laser photocoagulation.35 An example of a patient with lattice degeneration and both these prognostic features is shown in Figures 3C–E. These case examples highlight the benefit of performing peripheral OCT through peripheral lesions to help determine the optimum management. As peripheral OCT is time and skill-intensive, it is not practical to use peripheral OCT as a screening tool and instead should be applied in a targeted and supportive manner, based on funduscopic assessment.
Summary
Although OCT is most commonly used to supplement ocular examinations by characterising the optic nerve and macula, its applications extend beyond the posterior pole. OCT can supplement ocular health examinations from front-to-back including phenotyping of corneal ectasia, guiding treatment decision making for patients with narrow angles and risk stratification as well as management of patients with peripheral retinal pathology.
Henrietta Wang BOptom (Hons) BSc MPH FAAO is a senior staff optometrist and Lead Clinician (Glaucoma) at the Centre for Eye Health at the University of New South Wales with clinical interests in optic nerve and retinal pathology. She became a Fellow of the American Academy of Optometry in 2019 and has been regularly invited as a speaker at both national and international conferences.
References
1. Huang, D., Swanson, E.A., Lin, C.P., et al., Optical coherence tomography. Science. 1991;254(5035):1178–81.
2. Ly, A., Phu, J., Katalinic P., Kalloniatis, M., An evidence-based approach to the routine use of optical coherence tomography. Clin Exp Optom. 2019;102(3):242–59.
3. Shan, J., DeBoer, C., Xu, B.Y., Anterior Segment Optical Coherence Tomography: Applications for Clinical Care and Scientific Research. Asia Pac J Ophthalmol (Phila). 2019.
4. Dada, T., Sihota, R., Gadia, R., et al., Comparison of anterior segment optical coherence tomography and ultrasound biomicroscopy for assessment of the anterior segment. J Cataract Refract Surg. 2007;33(5):837–40.
5. Ong, S.S., Vora, G.K., Gupta, P.K., Anterior Segment Imaging in Ocular Surface Squamous Neoplasia. J Ophthalmol. 2016;2016:5435092.
6. Tran, A.Q., Venkateswaran, N., Galor, A., Karp, C.L., Utility of high-resolution anterior segment optical coherence tomography in the diagnosis and management of sub-clinical ocular surface squamous neoplasia. Eye Vis (Lond). 2019;6:27.
7. Karabatsas, C.H., Cook, S.D., Topographic analysis in pellucid marginal corneal degeneration and keratoglobus. Eye (Lond). 1996;10 ( Pt 4):451–5.
8. Koster, H.R., Wagoner, M.D., Topographical analysis of keratoconus. Int Ophthalmol Clin. 1993;33(2):261–9.
9. Stefano, V.S., Melo Junior, L.A., Mallmann, F., Schor, P., Interchangeability between Placido disc and Scheimpflug system: quantitative and qualitative analysis. Arq Bras Oftalmol. 2010;73(4):363–6.
10. Li, Y., Chamberlain, W., Tan, O., et al., Subclinical keratoconus detection by pattern analysis of corneal and epithelial thickness maps with optical coherence tomography. J Cataract Refract Surg. 2016;42(2):284–95.
11. Ostadian, F., Farrahi, F., Mahdian Rad, A., Comparison of corneal epithelial thickness map measured by spectral domain optical coherence tomography in healthy, subclinical and early keratoconus subjects. Med Hypothesis Discov Innov Ophthalmol. 2019;8(2):85–91.
12. Koc, M., Tekin, K., Inanc, M., et al., Crab claw pattern on corneal topography: pellucid marginal degeneration or inferior keratoconus? Eye (Lond). 2018;32(1):11–8.
13. Ferdi, A.C., Nguyen, V., Gore, D.M., et al., Keratoconus natural progression: A systematic review and ,eta-analysis of 11 529 eyes. Ophthalmology. 2019;126(7):935–45.
14. Das, A.V., Pillutla, L.N., Chaurasia, S., Clinical profile and demographic distribution of pellucid marginal corneal degeneration in India: A study of 559 patients. Indian J Ophthalmol. 2021;69(12):3488–93.
15. Yang, Y., Pavlatos, E., Chamberlain, W., et al., Keratoconus detection using OCT corneal and epithelial thickness map parameters and patterns. J Cataract Refract Surg. 2021;47(6):759–66.
16. Ertan, A., Differentiating keratoconus and pellucid marginal degeneration. J Refract Surg. 2007;23(3):221–2; author reply 2.
17. Maslin, J.S., Barkana, Y., Dorairaj, S.K., Anterior segment imaging in glaucoma: An updated review. Indian J Ophthalmol. 2015;63(8):630–40.
18. Desmond, T., Tran, V., Maharaj, M., et al., Diagnostic accuracy of AS-OCT vs gonioscopy for detecting angle closure: a systematic review and meta-analysis. Graefes Arch Clin Exp Ophthalmol. 2022;260(1):1–23.
19. Riva, I., Micheletti, E., Oddone, F., et al., Anterior chamber angle assessment techniques: A review. J Clin Med. 2020;9(12).
20. Salim, S., The role of anterior segment optical coherence tomography in glaucoma. J Ophthalmol. 2012;2012:476801.
21. Verma, S., Nongpiur, M.E., Oo, H.H., et al., Plateau iris distribution across anterior segment optical coherence tomography defined subgroups of subjects with primary angle closure glaucoma. Invest Ophthalmol Vis Sci. 2017;58(12):5093–7.
22. Stefan, C., Iliescu, D.A., Batras, M., et al., Plateau iris – Diagnosis and treatment. Rom J Ophthalmol. 2015;59(1):14–8.
23. Kim, Y.K., Yoo, B.W., Kim, H.C., et al., Relative lens vault in subjects with angle closure. BMC Ophthalmol. 2014;14:93.
24. Moghimi, S., Vahedian, Z., Zandvakil, N., et al., Role of lens vault in subtypes of angle closure in Iranian subjects. Eye (Lond). 2014;28(3):337–43.
25. Mansouri, M., Ramezani, F., Moghimi, S., et al., Anterior segment optical coherence tomography parameters in phacomorphic angle closure and mature cataracts. Invest Ophthalmol Vis Sci. 2014;55(11):7403–9.
26. Moraru, A., Pînzaru, G., Moţoc, A., Costin, D., Functional results of cataract surgery in the treatment of phacomorphic glaucoma. Rom J Ophthalmol. 2017;61(3):202–6.
27. Koh, V., Keshtkaran, M.R., Hernstadt, D., et al., Predicting the outcome of laser peripheral iridotomy for primary angle closure suspect eyes using anterior segment optical coherence tomography. Acta Ophthalmol. 2019;97(1):e57–e63.
28. Amini, R., Whitcomb, J.E., Prata, T.S., et al., Quantification of iris concavity. J Ophthalmic Vis Res. 2010;5(3):211–2.
29. Phu, J., Wong, B., Lim, T., Kalloniatis, M., Assessment of angle closure spectrum disease as a continuum of change using gonioscopy and anterior segment optical coherence tomography. Ophthalmic Physiol Opt. 2020;40(5):617–31.
30. Quinn, N., Csincsik, L., Flynn, E., et al., The clinical relevance of visualising the peripheral retina. Progress in Retinal and Eye Research. 2019;68:83–109.
31. Raevis, J., Hariprasad, S.M., Shrier, E., The depressing part of retina: A review of scleral depression and scleral indentation. Ophthalmic Surg Lasers Imaging Retina. 2021;52(2):58–60.
32. Choudhry, N., Duker, J.S., Freund, K.B., et al., Classification and guidelines for widefield imaging: Recommendations from the International Widefield Imaging Study Group. Ophthalmol Retina. 2019;3(10):843–9.
33. Midena, E., Marchione, G., Di Giorgio, S., et al. Ultra-wide-field fundus photography compared to ophthalmoscopy in diagnosing and classifying major retinal diseases. Sci Rep. 2022;12(1):19287.
34. Li, H., Chen, L., Wu Ma, Zheng B., Spectral-domain optical coherence tomography characteristics of cystic retinal tuft. BMC Ophthalmology. 2022;22(1):412.
35. Tsai, C.Y., Hung, K.C., Wang, S.We, et al., Spectral-domain optical coherence tomography of peripheral lattice degeneration of myopic eyes before and after laser photocoagulation. J Formos Med Assoc. 2019;118(3):679–85.