


Pachychoroid disease spectrum (PDS) is a relatively new pathological category definition. Previously thought of as separate entities, PDS encompasses a range of disorders characterised by underlying hyper-permeability of dilated choroidal vessels. As well as mimicking a range of other macular diseases, the ocular and systemic management and visual prognoses can vary markedly within the spectrum. As a result, it is critical to accurately differentially diagnose the specific conditions within PDS to optimise both visual and healthrelated outcomes. This is greatly enhanced by the application of multimodal imaging and a multidisciplinary approach.
In this article, Helene Ly steps us through a case of pachychoroid spectrum disease to highlight characteristic clinical features and their role in guiding clinical management.
CASE STUDY: VISIT ONE
A 44-year-old East Asian male was referred to the Centre for Eye Health (CFEH) for macular assessment in 2014 due to pigmentary changes at both maculae. He previously saw an ophthalmologist for an acute episode of central serous chorioretinopathy (CSC), which resolved without intervention at the time. He works in a high-stress job.
His best-corrected visual acuities were 6/4.8 right eye and 6/4.8 left eye with a moderate myopic prescription. Intraocular pressures were 17mmHg right eye and 15mmHg left eye. Slit lamp examination revealed healthy anterior segments. The posterior eye findings are illustrated in Figure 1.
CSC AND THE PACHYCHOROID SPECTRUM
Pachychoroid disease (PDS) is thought to arise from choroidal vascular hyperpermeability whereby venous overload and difficulty removing excess fluid from the subretinal space via the horiocapillaris and retinal pigment epithelium (RPE) leads to fluid accumulation.1,2
Since the introduction of the term in 2013 by Warrow and colleagues, pachychoroid has been classified into separate disease entities, thought to occur along a spectrum of disease progression.2 These include: peripapillary pachychoroid syndrome (PPS), pachydrusen, pachychoroid pigment epitheliopathy (PPE), CSC, pachychoroid neovasculopathy (PNV), polypoidal choroidal vasculopathy (PCV) (also known as type 1 aneurysmal neovascularisation), and focal choroidal excavation (FCE).2 It has been postulated that CSC can evolve to PNV, to PCV, and to FCE, however progression may not be linear.3
This case presented with a classical historical risk profile for CSC; a young to middle aged male with tendency for psychological stress.4 Other risk factors of CSC include: high levels of cortisol hormones (e.g., in Cushing syndrome, systemic exogenous or endogenous corticosteroids, etc.), hyperaldosteronism, pregnancy, systemic hypertension, poor sleep patterns (related to shift work or sleep apnoea), infection with helicobacter (H.) pylori or use of phosphodiesterase-6 inhibitors (e.g., Sildenafil for erectile dysfunction).3,4 Though the proposed pathophysiology varies among authors, it is thought that these factors may predispose the retina to inflammation and oxidative stress.4 As CSC is on the spectrum of PDS, these risks are important when taking a multidisciplinary approach in PDS patient care, as they help direct further testing or recommendations for general practitioners.
Multimodal imaging is inherent to the accurate diagnosis and management of PDS.5 In optometric practice, this involves fundus autofluorescence (FAF), optical coherence tomography (OCT), and OCT angiography (OCTA). In ophthalmological care, this may also include fundus fluorescein angiography (FFA) and indocyanine green angiography (ICGA).
Common features observed in PDS in optometric practice are described in Table 1, and typical disease appearances are outlined in Table 2. Briefly, different FAF patterns can present from acute or chronic changes in the RPE and photoreceptor outer segments. OCT allows non-invasive assessment of sub-retinal fluid, intra-retinal fluid, and RPE changes, as well as choroidal abnormalities with enhanced depth imaging (EDI). OCTA, in conjunction with OCT B-scans, show excellent sensitivity and are specific for detecting choroidal neovascularisation (CNV).3,6
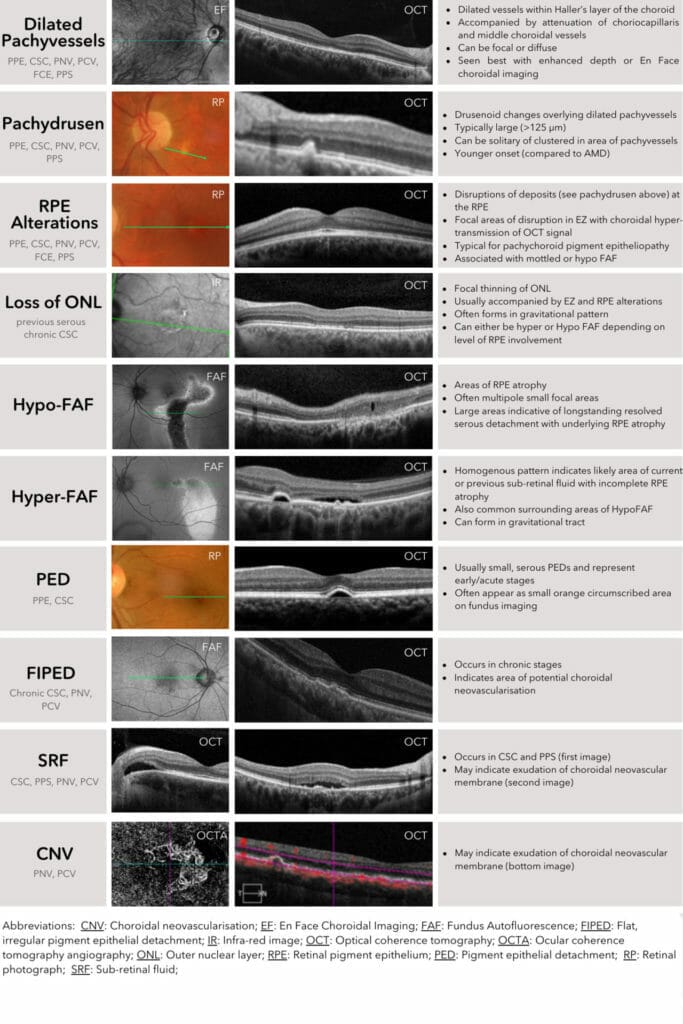
Abbreviations for Tables I and 2: AMD – Age-related macular degeneration; CNV – Choroidal neovascularisation; CSC – Central serous chorioretinopathy; EF – En Face choroidal imaging; EZ – ellipsoid zone; FAF – Fundus autofluorescence; FCE – Focal choroidal excavation; FIPED – Flat, irregular pigment epithelial detachment; ICGA – Indocyanine green angiography; IR – Infrared image; OCT – Optical coherence tomography; OCTA – Optical coherence tomography angiography; ONL – Outer nuclear layer; PCV – Polypoidal choroidal vasculopathy; PED – Pigment epithelial detachment; PNV – Pachychoroid neovasculopathy; PPE – Pachychoroid epitheliopathy; PPS – pachychoroid syndrome; RP – Retinal photography; RPE – Retinal pigment epithelium; SRF – Sub-retinal fluid.
Table 1 (above). Multimodal imaging features in PDS.3,7
Table 2 (below). PDS and different presentations.

Returning to our patient, Figure 1 illustrates the posterior ocular health findings for our case at his first visit to CFEH. Following this comprehensive assessment, the clinical picture in this case was consistent with a previous, simple CSC in the right eye and PPE in the left eye.

Figure 1: Colour fundus photography shows (A) mixed hypo- and hyperpigmentation superior to the fovea right eye, and at the fovea left eye. (B) Fundus autofluorescence highlights the areas of mottled pigmentation as mainly hypo-autofluorescent. (C) OCT line scans show a flat, irregular pigmented epithelial detachment (FIPED) shown by the arrow over dilated choroidal pachyvessels (shown by bracket) in the right eye. The left eye has focal EZ/RPE disruption at the fovea highlighted by increased choroidal transmission.
There are currently a number of classification systems used for CSC typically including acute, chronic, and recurrent depending on the longevity of subretinal fluid (up to six months for chronic).3 Recently the terms simple (FAF abnormalities <2disc diameters) and complex (FAF abnormalities>2Disc diameters) have also been proposed.7 The patient was advised on optimisation of his risk factors, and a referral was sent on to his general practitioner to assist as appropriate.
The patient’s right eye also showed a subfoveal flat, irregular pigmented epithelial detachment (FIPED), also known as a ‘double layer sign’.8 This is highlighted by the blue arrow in Figure 1, and is seen as an irregularly contoured separation of the hyper-reflective RPE from the hyper-reflective Bruch’s membrane. FIPEDs are usually seen with more complex/chronic CSC, with reviews stating that 22.7% may be vascularised.3 There was no evidence of exudation, i.e. sub-retinal, intra-retinal, and sub-retinal epithelial fluid was absent. Hence, a review was set for six months. OCTA was unavailable at this visit.
CASE STUDY: FIVE YEARS LATER
The patient was seen on a six monthly basis for two years, with no changes of note. Unfortunately, he was later lost to followup and returned to the clinic in 2019. He now had complaints of distortion, blur, and flashing lights in his right eye vision. His bestcorrected visual acuities were 6/7.5-1 right eye and 6/4.8-1 left eye. He was also recently diagnosed with systemic hypertension.
Imaging and clinical assessment revealed changes in the right eye shown in Figure 2. There was diffuse, homogenous hyperautofluores ence on FAF at the right macula consistent with the presence of sub-retinal fluid. This was confirmed with OCT showing sub-retinal fluid overlying the FIPED, as well as development of thumb-shaped pigmented epithelial detachment (PED) temporally. Fundoscopically, the right macula appeared hypopigmented and slightly elevated. The left eye appeared similar to baseline in all modalities.

It is thought that more complicated forms of PDS arise from changes of the RPE over a longer period of active disease. Initial stages are generally non-neovascular, as in PPE and CSC. Secondary CNV occurs in 24–39% of patients with chronic CSC and is almost always type 1 (sub-RPE).3 OCTA for this patient at this visit revealed a hyperfluorescent tangled vascular network consistent with active type 1 choroidal neovascularisation in the right eye (Figure 3).

Figure 3. Outer retina/choriocapillaris slab on OCT angiography on the Heidelberg Spectralis showing hyper-fluorescent type 1 choroidal neovascular network and subretinal fluid in B-scans.
The patient was promptly referred to an ophthalmologist for further investigation and management with a diagnosis of likely PCV, with exudative PNV as a differential diagnosis, in the right eye and stable PPE in the left eye.
PCV is a variant of type I CNV with aneurysmal changes (resembling polyps) in the vascular lesion, and more commonly diagnosed in Asian populations.9 The classical OCT signs of PCV include sharp-peaked PED, sub-RPE ring like lesions, en face complex, multilobular PED and double layer sign.10 The gold standard for diagnosing PCV remains ICGA and this was performed and confirmed by the treating ophthalmologist.
FINAL COMMENTS
Our case illustrates the importance of multimodal imaging when faced with the plethora of presentations in the pachychoroid disease spectrum. Ultimately, as primary eye care practitioners, it is vital that optometrists maintain a high standard of evidence-based care including initiating multidisciplinary care when necessary. Patients with PDS and in particular CSC require careful risk assessment and systemic investigations when needed with their general practitioner, including but not limited to, investigation of sleep quality (including sleep apnoea), hypertension, stress, and gastro-oesophageal disease.
Helene Ly B.Optom B.Vision Sci (Hons 1) is a staff optometrist at the Centre for Eye Health (CFEH) in Sydney. She received her Bachelor of Optometry and Vision Science from The University of New South Wales, receiving the Specsavers Prize for Excellence in Patient Management and the BOC Ophthalmic Instruments Prize. She has worked in corporate optometric practices and joined CFEH in 2022. Ms Ly is interested in giving affordable and accessible eye care to people from culturally and linguistically diverse backgrounds, especially in western Sydney.
References
1. Brown, R.B, Mohan, S., Chhablani, J., Pachychoroid spectrum disorders: An updated review. J Ophthalmic Vis Res. 2023;18(2):212–29.
2. Warrow, D.J., Hoang, Q.V., Freund, K.B., Pachychoroid pigment epitheliopathy. Retina. 2013;33(8):1659–72.
3. Fung, A.T., Yang, Y., Kam, A.W., Central serous chorioretinopathy: A review. Clin Exp Ophthalmol. 2023;51(3):243–70.
4. Semeraro, F., Morescalchi, F., Russo, A., et al., Central serous chorioretinopathy: Pathogenesis and management. Clin Ophthalmol. 2019;13:2341–52.
5. Ng, D.S., Ho, M., Chen, L.J., et al., Optical coherence tomography angiography compared with multimodal imaging for diagnosing neovascular central serous chorioretinopathy. Am J Ophthalmol. 2021;232:70–82.
6. Bonini Filho, M.A., de Carlo, T.E., Ferrara, D., et al., Association of choroidal neovascularization and central serous chorioretinopathy with optical coherence tomography angiography. JAMA Ophthalmol. 2015;133(8):899–906.
7. Chhablani, J., Cohen, F.B., Multimodal imaging-based central serous chorioretinopathy classification. Ophthalmol Retina. 2020;4(11):1043–6.
8. Sheth, J., Anantharaman, G., Chandra, S., Sivaprasad, S., ‘Double-layer sign’ on spectral domain optical coherence tomography in pachychoroid spectrum disease. Indian J
Ophthalmol. 2018;66(12):1796–801.
9. Cheung, C.M.G., Lai, T.Y.Y., Ruamviboonsuk, P., et al. Polypoidal choroidal vasculopathy: definition,
pathogenesis, diagnosis, and management. Ophthalmology. 2018;125(5):708–24.
10. Cheung, C.M.G., Lai, T.Y.Y., Teo, K., et al., Polypoidal choroidal vasculopathy: Consensus nomenclature and non-indocyanine green angiograph diagnostic criteria from the Asia-Pacific Ocular Imaging Society PCV Workgroup. Ophthalmology. 2021;128(3):443–52.





