
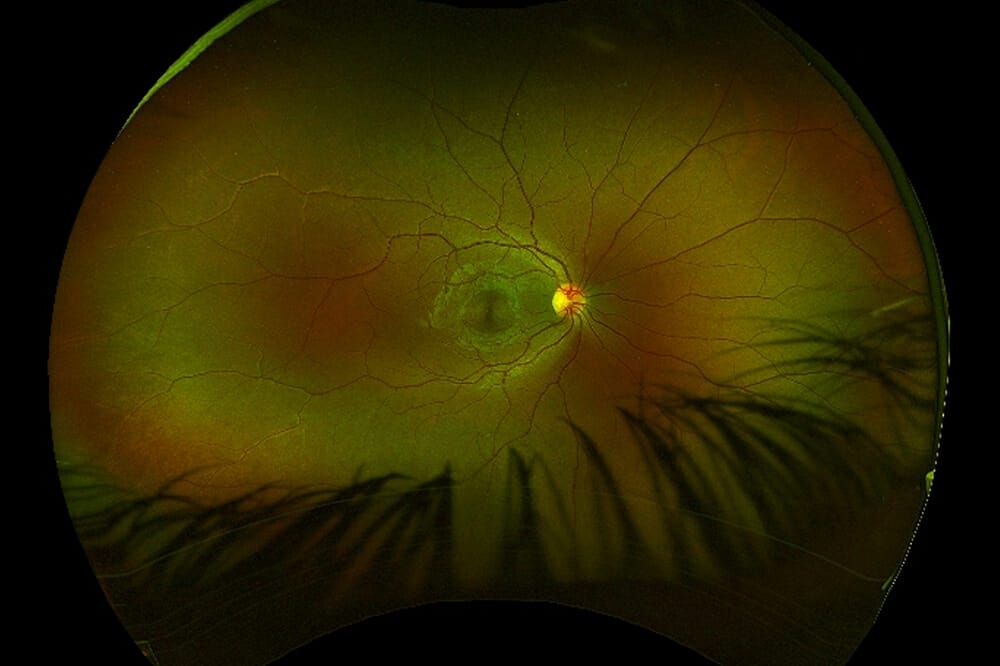
Figure 1. Optos images of bilateral fundus highlighting temporal optic disc pallor
Optic neuritis (ON) associated with multiple sclerosis (MS) has been recorded throughout history. In this article Dr Rushmia Karim discusses the prevalence of ON associated with MS, the symptoms you may observe in clinic, necessary considerations, and the required action.
In 1917, C.A. Veasey published two isolated cases. In one, a 60-year-old, post cataract surgery, was found to have a swollen optic nerve with the patient given the usual treatment together with mercury plus iodides.1 In 1924, L. Buchanan documented four cases of monocular optic neuritis, commenting on the localised non-suppurative inflammation that typically occurs in the retrobulbar attack.2 While we have come a long way from mercury poisoning over the past century, optic neuritis frequently poses a diagnosis challenge.
Data on the prevalence of ON and MS is also challenging regarding global incidence. Braithwaite et al. reviewed The Health Improvement Network (THIN) data set from 1 January, 1995 to 1 September, 2019,3 concluding an incidence of 3.74 per 100,000 person-years for 22 years.3 A nationwide optic neuritis study in South Korea mimicked similar results to Western countries for the paediatric population, but found a lower incidence in the adult population. The diagnosis of MS in this population was estimated to be 10.6%.4 Cumulative conversion to MS was estimated to be 13.8% in the paediatric group.4
FEATURES OF OPTIC NEURITIS IN MULTIPLE SCLEROSIS
Overall, ON is an idiopathic condition with inflammation, with or without demyelination associated with MS. Atypical optic neuritis can result from an inflammatory, infectious, or autoimmune disorder.5
Optometrists and ophthalmic health professionals play a critical role in a patient’s journey through the disease. It is important to carefully counsel them about MS and offer appropriate diagnostic evaluation, despite most of the ON presenting as a sporadic condition with an excellent visual prognosis.
Interestingly, ocular inflammation is the most common presentation in those diagnosed with MS, with approximately 50% of patients with MS experiencing ON.6 Most of those seen with ON are young females.7 The classic presenting features include unilateral, subacute, and painful visual loss without systemic or other neurological symptoms.7
What is distressing to patients is the recurrent relapses and the unpredictability of these episodes. Patients are often well, and atypical features can delay prompt investigation and referral. These features may include optic nerve pallor, complete visual impairment, and bilateral disease presentation. It is important to consider differentials including infection, auto-immune conditions, external toxicity, and genetic disorders. ON with associated MS and/or neuromyelitis optica (NMO) must be excluded.
Kale et al. described clinically isolated syndrome (CIS) as “a clinical demyelinating event that is isolated in time and mostly is the initial attack of MS”.7 These patients can present with an array of neurological symptoms besides ON, including pyramidal tract, brainstem symptoms, cerebellar involvement, and transverse myelitis.7
In the optometry setting, clinical characteristics that should be assessed include history regarding visual problems with both light and colours, periorbital pain, and vision loss. Simple questions can be asked regarding fatigue, change in bladder and bowel function, co-ordination/balance and numbness. This helps triage severity and prompt referral. The severity of vision loss can be minimal, from 6/6 to gross changes associated with optic atrophy and no light perception. Over 90% of patients complain about pain on eye movements, which is a sensitive symptom for ON but not specific.7 It is important to perform visual field testing as a range of visual field defects, including centrocecal scotomas, may be the only presenting symptom in the sub-acute setting. Altitudinal defects are rare, which warrants considering other differentials.
Spending considerable time evaluating the pupil for a relative afferent pupillary defect (RAPD) is crucial. Paradoxical dilation in the affected eye during the swinging light test can be seen in unilateral ON. It is important to note that if there is an eye with previous optic neuropathy and a fixed non-reactive pupil, a swinging light test can still be performed. Observation of the other eye needs to be conducted when flashing the light on the neuropathic eye. Retrobulbar ON can also present with an initial normal assessment. In certain acute cases, optic disc swelling is seen and can be evaluated.
In classic ON, visual field defects progress for the first 14 days then gradually recover. Optic atrophy and pallor are a late sign. Simple contrast sensitivity tests can be performed in the optometry setting showing abnormalities in low contrast letter acuity, changes in light saturation, and red saturation. Asking the patient whether there is any difference between the two eyes when viewing a red tip or object often results in patients noting a muted, less vibrant colour in the affected eye. Monocular and binocular visual function testing should be performed.
LANDMARK TRIAL
The 1991 Optic Neuritis Treatment Trial (ONTT) was a landmark study, the findings from which are still used in clinical practice for counselling and treatment of patients with ON. It is important to take time to understand this study.
The trial enrolled 457 patients between 1988 and 1991. The objectives were to evaluate the efficacy of corticosteroids and the relationship between ON and MS.8
Participants were aged from 18–46 years and all presented with unilateral ON. Additionally, they all had a relative afferent pupillary defect and visual field defect in the affected eye with no previous episode of ON and no previous treatment of corticosteroids.
Patients were assigned to oral prednisolone at 1mg per kg for 14 days, or placebo, or intravenous methyl prednisolone sodium succinate (250mg, four times a day for three days) followed by oral prednisolone 1mg per kg for 11 days. Visual acuity, contrast sensitivity, and colour vision were tested.
Results showed that patients in the oral prednisolone plus intravenous group had accelerated visual recovery but no long-term benefit to vision. This group also had a reduced rate of MS development, however by three years this affect subsided. The oral prednisolone-only group showed an increased rate of new attacks compared with placebo.8
The ONTT evaluated the risk of developing MS based on findings on initial magnetic resonance imaging (MRI). The conclusion was that should a patient have one episode of ON without pathology on MRI, their risk of MS was reduced to 25% over 15 years. If one or more lesions were seen, their risk would increase to 72% over 15 years. This finding is still used in clinics to gauge prognosis for patients coming with initial ON, although more current studies give further accuracy in prognosis.8
BIOMARKERS
Biomarkers for NMO spectrum disorders have now been established, including aquaporin-4 (AQP4) antibody and immunoglobin G (IgG). Myelin oligodendrocyte glycoprotein (MOG) IgG was recognised for a central demyelinating disease with characteristic ON, disc oedema, and perineural optic nerve enhancement on MRI. These are important biomarkers to test for in all ON patients due to the variation in treatment between closely related but differing disease entities.9 Classic NMO can be either bilateral or unilateral, is often recurrent/ severe and associated with transverse myelitis (vertebra).9 Patients with MOG autoimmunity present with a diverse phenotype, which can include ON, transverse myelitis, acute demyelinating encephalomyelitis, and brainstem encephalitis.5,9
Spending considerable time evaluating the pupil for a relative afferent pupillary defect (RAPD) is crucial
In the United States, NMO is more common in females with a mean age of 41, and can present more commonly in Asian or African populations. T1-weighted MRI nerve enhancement, as well as vertebra enhancement, is seen in those with transverse myelitis. A critical review of both typical and atypical ON by Abel et al. summarised diagnostic criteria for seropositive NMO spectrum disorder (SD). It stated, “the patient must test positive for serum AQP4-IgG and present with at least one of the six core clinical characteristics: (1) optic neuritis, (2) acute myelitis, (3) area postrema syndrome (unexplained intractable hiccups or nausea and vomiting), (4) acute brainstem syndrome, (5) symptomatic narcolepsy or acute diencephalic syndrome with NMOSD-typical diencephalic MRI lesions, or (6) symptomatic cerebral syndrome with NMOSD-typical brain lesions.”5
It is important to consider auto immune diseases, such as systemic lupus erythematosus, Sjogren’s syndromes, autoimmune thyroiditis, and myasthenia gravis. All of these have been associated with NMOSD; simple biochemistry testing during the diagnostic process should be performed.5
Additionally, it is important to understand a separate entity, which is chronic relapsing inflammatory optic neuritis (CRION). This is a steroid dependent ON showing enhancement of the optic nerve on MRI in conjunction with seronegative AQP4. Patients have good visual prognosis but may need longer-term corticosteroids. CRION is a diagnosis of exclusion of all other vasculitis and MOG-Ig ON, with relevant lab work proving no other findings.5
EVALUATION AND DIAGNOSIS OF OPTIC NEURITIS IN MULTIPLE SCLEROSIS
Optical Coherence Tomography
Optical coherence tomography (OCT) has changed the way we diagnose and evaluate patients in optometry and its use for ON is no different. This quick noninvasive test has excellent reproducibility and easy image transfer. Evaluation of the retinal nerve fibre layer (RNFL) is used to highlight axonal loss secondary to previous ON. Availability of ganglion cell layer (GCL) and inner plexiform layer (IPL) segmentation with spectral domain OCT can highlight thinning sub-acutely in patients with ON.5,10
Walter et al. showed the macular RNFL and ganglion cell layer-inner plexiform layer (GCL IPL) were significantly decreased in MS versus control eyes, and in MS ON versus non-ON eyes. Peripapillary RNFL, macular RNFL, GCL-IPL, and the combination of macular RNFL, GCL-IPL were significantly correlated with visual acuity (VA).11 Similar studies highlight the use of OCT in MS and ON, noting statistically significant changes in RNFL thickness in both groups, with no changes in colour vision and visual fields (VFs) detected.12 OCT was also found to be a useful marker for assessment of MS progression, correlating with disability and reduced quality of life.12
The S Noval investigator group published a letter to the editor and also reported their study which concluded, “Scores for low-contrast letter acuity and contrast sensitivity correlate well with RNFL thickness as a structural biomarker, supporting validity for these visual function tests as secondary clinical outcome measures for MS trials. These results also suggest a role for ocular imaging techniques such as OCT in trials that examine neuroprotective and other disease-modifying therapies.”13
This was also supported by the Fisher et al. study, which showed scores for low contrast letter acuity correlated well with RNFL thickness and in MS patients “for every one-line decrease in low-contrast letter acuity or contrast sensitivity score, the mean RNFL thickness decreased by 4m”.15
Magnetic Resonance Imaging
MRI is now considered a gold standard in the diagnosis and monitoring of both ON and associated MS. Brain and spinal cord lesions are characteristic demyelinating lesions located in the periventricular area of the white matter and radiating into the ventricular spaces. Generally, they are approximately 3mm and ovoid in shape.7 Imaging of acute lesions can be enhanced with gadolinium, hence MRI with contrast (GAD) should be ordered appropriately in suspected ON.5 While there is currently no single test for MS, MRI findings show a high predictability and additional spinal cord MRI imaging can highlight additional MS lesions. Hence, MRI should always be ordered if any brain lesions are found.
Multifocal Pattern Visual Evoked Potential and Lumbar Puncture
While predominantly performed in the neurology setting, it is important to understand the importance of multifocal pattern visual evoked potential (MVEP) and lumbar puncture (LP) in diagnosis and management for ON. MVEP with LP testing was found to be a sensitive and specific tool for ON showing considerable latency.15 The amplitude of the VEPs is believed to reflect the number of functional optic nerve fibres.15
A multi-disciplinary approach towards ON is needed, especially in cases where the diagnosis is uncertain from ophthalmic findings. Neurologist use of MVEPs and further LP could be warranted. LP looking for oligoclonal bands can further aid in the diagnostic criteria for MS, but this is an invasive test that needs careful consideration.
VISUAL FUNCTION IN OPTIC NEURITIS
Although long-term visual function is generally good, Gal et al. showed reduced NEI-VFQ (National Eye Institute Visual Function Questionnaire) scores in patients with ON.16 Most patients’ visual recovery is rapid, however the extent of visual loss can depend on the initial severity of visual disturbance.16,17 In summary, patients who experience an attack of acute idiopathic or demyelinating ON can be advised that the long-term visual prognosis is favourable, even if MS develops.16
DIAGNOSIS OF MULTIPLE SCLEROSIS
MS characteristically affects those under 50-years-old and can affect the paediatric population. Symptoms need to last more than 24 hours. Diagnosis is a combination of history, examination, MRI, and laboratory results. Despite there being no cure for MS, diagnosis is important because there are now excellent treatment modalities.
The National Institute for Health and Care Excellence (NICE) in the United Kingdom published its management guidelines of MS in 2022, highlighting key diagnostic symptoms being loss/reduction of vision, double vision, gait/balance disturbances, and sensory disturbance/weakness.18
MRI lesions with varying enhancement, as well as oligoclonal bands with established neurological deficit, are outlined in the McDonald criteria.19 Studies by Arnold et al. in 2005 and Abel et al. in 2019 contradicted the NICE guidelines regarding MRI findings alone for diagnosis of MS. They concluded that to diagnose MS, it is sufficient to find a combination of clinical latent MRI lesions and new enhancing lesions in at least two of the four following areas: periventricular, cortical and juxtacortical, infratentorial, and spinal cord.5,20
Risk With MRI playing a significant role in diagnosis, many cases of MS are now being discovered by ophthalmologists, general practitioners, and/or optometrists. Patients in the clinical setting often find a diagnosis of ON distressing due to its association with MS. It is, therefore, important to take a sensitive approach and to ensure they understand the prognosis and risk of developing MS.5,18,19,20
Once diagnosis is established, it is important to encourage patients to exercise, give up smoking, and advise that vaccinations should be updated, to ensure they are eligible for available treatment options. Careful counselling in a sensitive manner is key. We need to acknowledge the societal stigma of the condition and help patients understand its non-hereditary nature.
CONSIDERATIONS
Optic Neuritis and Vaccinations
CoroCase series have reported on the association between ON and vaccinations for infective pathogens such as hepatitis, and influenzas. A 2022 survey reviewed ophthalmology publications potentially highlighting an association between ON and vaccinations for DTaP-IPV, hepatitis A, influenza (quadrivalent, inactivated), influenza NIH1, influenza (trivalent, inactivated), measles, typhoid fever, rabies, TDaP; typhoid fever and zoster (live-attenuated).21 While there were several studies looking at vaccines and ON, all found no statistically significant increase in the risk of developing MS. Furthermore, United States military studies found no association with vaccines including anthrax, small-pox, hepatitis B or influzena.21 Investigators have hypothesised that optic neuropathies occurring within hours of a booster vaccination implicate an immediate hypersensitivity reaction, while those presenting two to three weeks after exposure are consistent with a B- or T-cell mediated reaction.22
Coronavirus
As of 13 February, 2021, there were 46 reports of ocular- and adnexa-related side effects from coronavirus. Of these, a majority (34 [74%]) involved eyelid or conjunctiva. Other anatomic areas (optic nerve, retina, uveal tract, and anterior segment) were each reported four times (< 9%) or less. There is insufficient information to comment on trends or establish causal association, especially for ON.22
A 2019 study looking at ocular events after coronavirus found that “The matched cohort analysis found an increased risk for the composite outcome after the second dose; however, the SCCS (self-controlled case series) analysis showed no increased risk. Considering that the SCCS can cancel out time-invariant confounders, the current results suggest that COVID-19 vaccination is unlikely to causally increase the risk of ocular adverse events.”22
Immune Checkpoint Inhibitors
Immune checkpoint inhibitors (ICI) have revolutionised cancer therapy and assisted in longer-term survival with targeted therapy. It is important to take a medication history in the clinical setting and to consider whether these drugs are causing visual impairment.
These drugs include monoclonal antibodies that block and inhibit cytotoxic T-lymphocyte associated antigen 4 (ipilimumab and tremelimumab), programmed cell death protein 1 (nivolumab, pembrolizumab, and cemiplimab), and programmed cell death ligand 1 (atezolizumab, avelumab, and durvalumab). Generally, ICIs potentiate the T-lymphocyte response, including reactivity against tumour cells.23
These medicines can also target normal cell lines, including causing inflammatory events like ON. Inflammatory ophthalmic conditions occur in 1% of patients receiving ICIs and can impact almost any aspect of the ophthalmic system.23
Only case reports have been published on ICI associated ON, so further evidence is needed. Close collaboration between oncologist and ophthalmic provider is required to ensure quality of vision while balancing prolonging life with these treatment modalities. The Francis group has published the largest study to date of 18 eyes with ICI-associated ON in 11 patients diagnosed at three centres.23 It reported that ICI-ON had clinical features that were not entirely consistent with the classic triad (unilateral decreased vision, dyschromatopsia 92%, and pain >90%) making diagnosis and monitoring challenging.23
CASE STUDIES
Case One: Incidental Finding
A 20-year-old woman was referred by her optometrist for incidental bilateral optic disc pallor. This was a routine assessment, and the patient was asymptomatic. A detailed history revealed immense fatigue over the past two years, which she attributed to the stress of educational exams. She reported no changes in bladder and bowel function, but some recent numbness down her left leg and associated pins and needles. There was nil history of trauma or regular medications, and she had no significant family history. Her visual acuity was maintained at 6/6 in both eyes over the course of investigation and treatment.
Clinical assessment showed bilateral optic atrophy on slit lamp assessment and confirmed on Optos (Figures 1–3). OCT RNFL showed temporal thinning associated with the optic disc temporal pallor and visual fields of 24/2 were outside normal limits with left arcuate scotoma.
T2 MRI sequences / contrast with gadolinium showed extensive periventricular white matter lesions with spinal extension. The patient has been started on treatment after varicella vaccination.

Figure 1. Optos images of bilateral fundus highlighting temporal optic disc pallor.
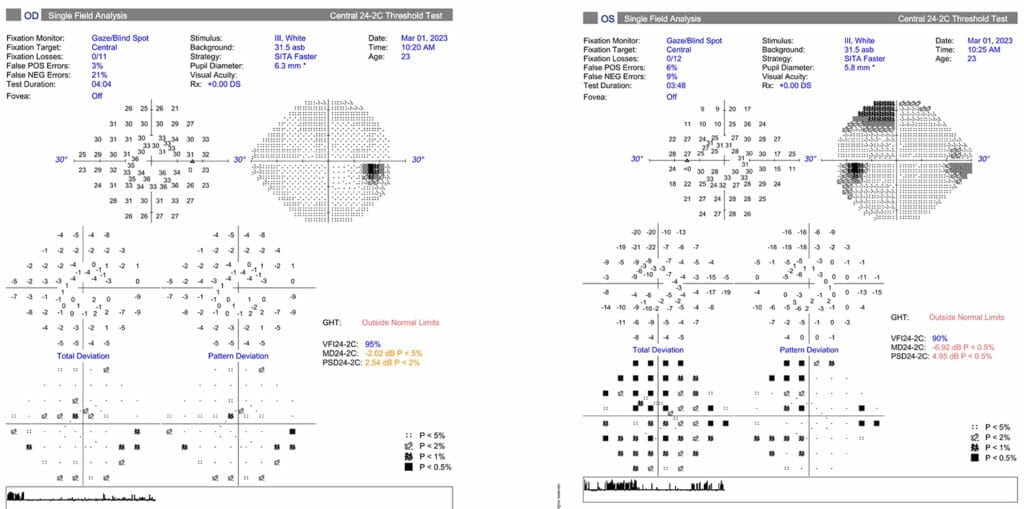
Figure 2. Bilateral 24/2 visual fields with patches of visual field loss outside normal limits, and left superior field defect in the absence of dermatochalasis. Note the good fixation but few false positive and false negative errors

Figure 3. OCT of the optic nerve showing RNFL thinning on the macular cube and RNFL thinning on the optic disc cube
MRI is now considered a gold standard in the diagnosis and monitoring of both ON and associated MS
Case Two: Onset Post-Vaccination
A 30-year-old female government worker was referred by her optometrist. Otherwise healthy, she had no history of trauma or regular medications, and no family history. She had developed pain on eye movements five to seven days post-COVID vaccination.
Her visual acuity was noted to be 6/6 in both eyes throughout previous and current assessments. She had been seen at a tertiary hospital and started on pulsed meth prednisolone. An initial computed tomography (CT) scan was normal, as was the eye assessment performed by the on-call ophthalmology registrar. Outpatient OCT imaging showed normal RNFL one to two weeks post initial steroid treatment. The patient continued with light sensitivity and photophobia.
She was seen months later in the neuro ophthalmology clinic with gross optic atrophy from presumed optic neuritis (Figure 4). Her visual acuity, OCT, and visual fields remained stable (Figure 5), but the photosensitivity had persisted. Vaccination causality was hard to establish, and evidence showed no statistical significance in the current published data. Given the acute onset and history of good health, the patient was awarded damages associated with vaccine instillation.

Figure 4. OCT of the macular cube showing some RNFL thinning in the left eye

Figure 5. OCT of the optic disc with gross RNFL thinning in all quadrants highlighting chronicity
Case Three: Atypical Correlation of Signs and Symptoms
A 28-year-old engineer with a 12-month history of headaches presented with acute pain on eye movements and loss of visual fields over 24 hours. Visual acuity from previous optometry records were 6/5 in both eyes and this dropped to 6/9 in the left eye. The patient was otherwise well with no history of trauma and nil regular medications. Visual fields showed global and peripheral visual loss (Figure 6). Optic nerves showed some physiological high cup disc ratio and OCT revealed atypical superior NFL thinning (Figure 7). Due to the typical history of optic neuritis, the patient was sent for MRI / blood screening and pulsed methyl prednisolone treatment was initiated over three days in the hospital emergency/ambulatory care.

Figure 6. OCT of the macula and optic nerve with atypical RNFL thinning superior, seen in physiological large cups or atypical normal tension glaucoma

Figure 7. Visual field showing peripheral field but no typical central scotoma
Serial MRI with contrasts have been normal to this date, however visual field changes have improved with resolution of symptoms. A second opinion was sought with another neuro-ophthalmologist, and both decided presumed optic neuritis.
Case Four: Asymptomatic with Extensive MRI Changes
A 55-year-old female presented with horizontal double vision and a suspected sixth cranial nerve palsy. She had a previous history of seventh cranial nerve palsy. A non contrast MRI was performed elsewhere, with a few white nonspecific foci noted. Clinical assessment showed no RAPD, normal optic nerve, full visual fields, and normal OCT (Figures 8 and 9). No sixth nerve palsy was found, but history highlighted fluctuating double vision with normal cover testing and no fatigability. An MRI contrast brain was ordered, along with bloods, including thyroid function and Ach receptor antibody / anti-musk antibody for myasthenia gravis.

Figure 8. Normal OCT macular cube and RNFL

Figure 9. Normal OCT optic disc and RNFL
The MRI report showed dozens of extensive white matter lesions with six lesions showing contrast enhancement, indicating established and new lesions. Spinal MRI showed further lesions. The patient is currently being treated with Fingolimod and remains asymptomatic.
The MRI report stated, “Dozens of white matter track lesions distributed in place around the brain including corpus callosum, pericallosal/periventricular white matter, central white matter, juxta-cortical and within the pons. Six lesions show contrast enhancement indicating a mix of established and more recent lesions. These lesions fulfil the MRI imaging diagnostic criteria for demyelination/multiple sclerosis.”
Dr Rushmia Karim BSc MBBS MMed (Ophthsc) MMed (Clinical Epidemiology) Hons Genomics (PG Cert) FRCOphth FRANZCO is a UK-trained ophthalmologist with over 10 years of experience. She specialises in children’s eye health and is a skilled surgeon, performing cataract, lens, and strabismus surgery in both adults and children. She also has a special interest in neuro-ophthalmology. Dr Karim has an extensive research portfolio. She has performed and published systematic reviews including Cochrane reviews, randomised controlled studies and observational studies. Dr Karim consults at Vision Eye Institute in Chatswood, Drummoyne, and Tuggerah Lakes (Central Coast) in New South Wales.
References
1. Veasey C., Unilateral optic neuritis, 1917 Spokan Washington.
2. Buchanan L., Monocular optic neuritis. Br J Ophthalmol. 1923 Apr;7(4):170-4. doi: 10.1136/ bjo.7.4.170. PMID: 18168281; PMCID: PMC513632. 3. Braithwaite T., Subramanian A., Petzold A., Galloway J., et al. Trends in optic neuritis incidence and prevalence in the UK and association with systemic and neurologic disease. JAMA Neurol. 2020 Dec 1;77(12):1514.
4. Lee J.Y., Han J., Yang M., Oh S.Y., Population-based incidence of pediatric and adult optic neuritis and the risk of multiple sclerosis. Ophthalmology. 2020 Mar 1;127(3):417–25.
5. Abel A., McClelland C., Lee M.S., Critical review: Typical and atypical optic neuritis. Vol. 64, Survey of Ophthalmology. Elsevier USA; 2019. p. 770–9.
6. McIlwaine G., Csincsik L., Coey R., Wang L., et al., Reduced cone density is associated with multiple sclerosis. Ophthalmology Science. 2023 Sep 1;3(3).
7. Kale, N., Optic neuritis as an early sign of multiple sclerosis. Vol. 8, Eye and Brain. Dove Medical Press Ltd.; 2016. p. 195–202.
8. Beck R.W., Trobe J.D., What we have learned from the optic neuritis treatment trial. Ophthalmology. 1995;102(10):1504–8.
9. Chen J.J., Pittock S.J., Flanagan E.P., Lennon V.A., Bhatti M.T., Optic neuritis in the era of biomarkers. Vol. 65, Survey of Ophthalmology. Elsevier USA; 2020. p. 12–7.
10. Pujari A,. Bhaskaran K. Sharma P., Singh P., et al., Optical coherence tomography angiography in neuro-ophthalmology: Current clinical role and future perspectives. Vol. 66, Survey of Ophthalmology. Elsevier Inc.; 2021. p. 471–81.
11. Walter S.D., Ishikawa H., Galetta K.M., Sakai RE, et al., Ganglion cell loss in relation to visual disability in multiple sclerosis. Ophthalmology. 2012 Jun;119(6):1250–7.
12. Garcia-Martin E., Ara J.R., Martin J., Almarcegui C., et al., Retinal and optic nerve degeneration in patients with multiple sclerosis followed up for 5 years. Ophthalmology. 2017 May 1;124(5):688–96.
13. Noval S., Contreras I., Rebolleda G., Muñoz-Negrete F., Optical coherence tomography in optic neuritis. Dear Editor: Ophthalmology. 2007 Jan;114(1):200–200.
14. Fisher J.B., Jacobs D.A., Markowitz C.E., Galetta S.L., et al., Relation of visual function to retinal nerve fiber layer thickness in multiple sclerosis. Ophthalmology. 2006 Feb;113(2):324–32.
15. You Y., Klistorner A., Thie J., Graham S.L., Latency delay of visual evoked potential is a real measurement of demyelination in a rat model of optic neuritis. Investigative Ophthalmology and Visual Science. 2011 Aug 29;52(9):6911.
16. Gal R.L., Brodsky M., Nazarian S., et al. Visual function 15 years after optic neuritis. A final follow-up report from the Optic Neuritis Treatment Trial. Ophthalmology. 2008 Jun 1;115(6):1082.e5.
17. Beck R.W., Cleary P.A., Backlund J., et al., The course of visual recovery after optic neuritis: Experience of the Optic Neuritis Treatment Trial. In: Ophthalmology. Elsevier Inc.; 2020. p. S174–81.
18. Multiple sclerosis in adults: management NICE guideline [Internet]. 2022. Available from: www.nice.org. uk/guidance/ng220.
19. Thompson A.J,. Banwell B.L., Barkhof F., et al., Diagnosis of multiple sclerosis: 2017 revisions of the McDonald criteria. Lancet Neurol. 2018 Feb;17(2):162–73.
20. Arnold A.C., Evolving management of optic neuritis and multiple sclerosis. Am J Ophthalmol. 2005;139(6).
21. Cheng J.Y., Margo C.E., Ocular adverse events following vaccination: overview and update. Vol. 67, Survey of Ophthalmology. Elsevier Inc.; 2022. p. 293–306.
22. Hashimoto Y., Yamana H., Iwagami M., et al., Ocular adverse events after coronavirus disease 2019 mRNA vaccination: Matched cohort and self-controlled case series studies using a large database. Ophthalmology. 2023 Mar 1;130(3):256–64.
23. Francis J.H., Jaben K., Santomasso B.D., Canestraro J., et al., Immune checkpoint inhibitor-associated optic neuritis. Ophthalmology. 2020 Nov 1;127(11):1585–9





