
Geographic atrophy (GA), a late form of age-related macular degeneration (AMD), until now has been untreatable, leading to progressive loss of central vision. In early 2023, the first treatment for GA , Pegcetacoplan (Syfovre, Apellis Pharmaceuticals), was approved in the United States and has been used in clinical practice for several months. In August, a second treatment, avacincaptad pegol (Izervay, Iveric Bio), also received approval in the US. Other jurisdictions are expected to gain approval in the not too distant future.
How do we ensure that we are in the best position to manage GA when treatments become available to slow vision loss? Longitudinal multi-modal imaging of the retina and upskilling to identify biomarkers influencing growth will help in the management of GA in this new era.
What can we do now to be in the best position to counsel and advise our patients when treatment options arrive on our shores?
Patients with age-related macular degeneration (AMD) who have progressed to the late stage of GA, are often managed by community-based eye care professionals.
Current management, in line with Royal Australian and New Zealand College of Ophthalmologists (RANZCO) AMD referral guidelines and Optometry Australia’s Chairside Reference for AMD, is to explain their disease, identify and improve risk factors, counsel on the use of an Amsler grid, optimise spectacles, refer to low vision and other support services as appropriate, and plan to review in six to 12 months, depending on individual circumstances.1,2 However, this is all about to change as we fast approach a world that will have treatments for GA.
What does this mean then for our management of these patients? Unlike neovascular AMD (nAMD), where treatment is required urgently and in virtually everyone, treatment decisions for those with GA will not be so straightforward. Who should we be discussing these new treatments with and who should be considered for referral for treatment? What can we do now to be in the best position to counsel and advise our patients when treatment options arrive on our shores?
About Geographic Atrophy
GA is one of two late forms of AMD, and in people of European descent its prevalence is about equal to that of the other late form of AMD – nAMD.2 In Australia, it is estimated that around 1.3 million people have AMD, (14% of the 9.3 million over the age of 50), all with a potential risk of progressing to GA. Estimates suggest 1–2% of the population over the age of 50 have late stage AMD, or 100–200,000 people, with half having currently untreatable GA.3
When considering the impact of GA on an individual’s visual function and their overall quality of life, not all GA lesions are equal. For example, the location of the atrophic lesions and their direction of growth vary, meaning that the imminent threat to the fovea and central vision differs considerably.
Lesion growth shows significant heterogeneity, with one study reporting that while the median overall growth rate of GA lesions was 1.78 mm2/year, the range was from 0.53 to 2.6 mm2/year.4
Knowing the rate of growth in an individual is paramount to understanding the imminent threat to the fovea and with it, fine detailed central vision. There is now intense interest to understand characteristics, or biomarkers, that help predict an individual’s growth rate as this impacts their outcome and will need to be considered when discussing whether or not to treat.
Imaging Geographic Atrophy
Determining the extent of GA within an eye, as well as identifying many of these growth biomarkers, is best achieved by imaging the retina, particularly with optical coherence tomography (OCT) and fundus auto-fluorescence (FAF). Using these imaging techniques, researchers have uniformly found that slower growth rates are seen when baseline lesions are small, rather than big, unifocal compared to multifocal, and when the lesions are located at the fovea compared to extra-foveally.4,5
The direction of growth is also an important consideration, with growth toward the fovea appearing slower than progression toward the periphery.6
The status of both eyes is also important, with growth rates appearing to be faster when the fellow eye also has GA.7
Identifying and documenting these characteristics in each case of GA will certainly help frame a discussion on treatment options.
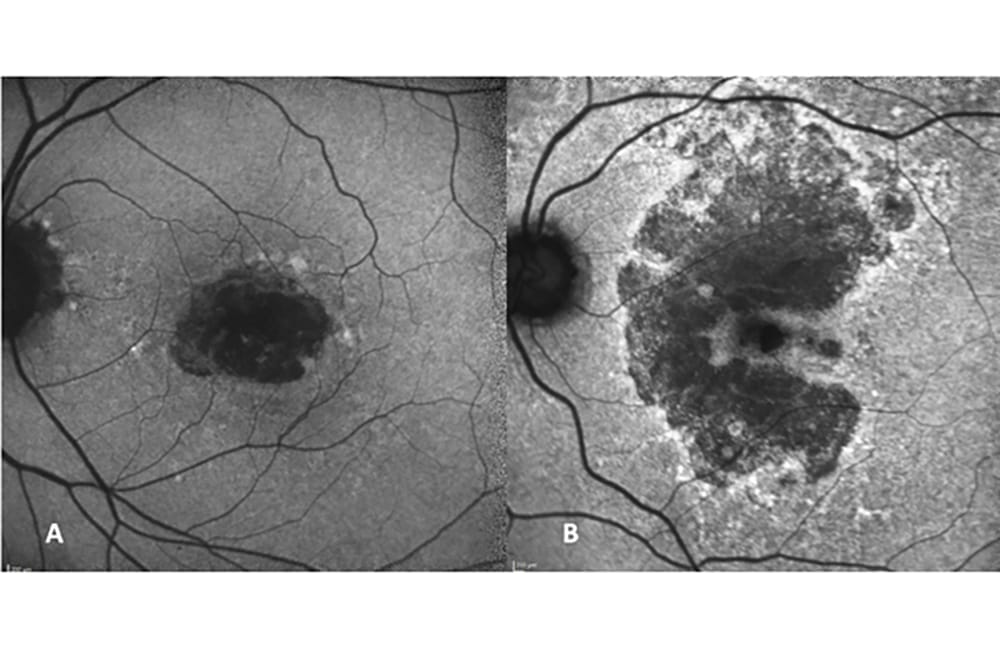
The fundus FAF image allows us to delineate the extent of the lesion, much better than a colour image or a clinical examination, as the lesions appear dark grey or black due to the lack of the retinal pigment epithelium (RPE) that provides the auto fluorescent (AF) signal. FAF images, captured over successive visits, are useful to show patients and their relatives how their lesions are changing over time. This helps guide a discussion on the potential importance of an intervention to slow down the growth of the lesions. FAF also allows us to look at patterns of AF surrounding the lesions, referred to as background AF. There are different background AF patterns, with the characteristics of the hyper-AF spots important as a biomarker of growth rate. Shown in Figure 1A is a GA lesion without any hyper-AF lesions in the background image. Such lesions are the slowest growing lesions, whereas the most rapid rate of growth will be in those eyes with a diffuse pattern of background hyper-AF (Figure 1B).8

Figure 1. (A) FAF of a GA lesion with minimal hyper-AF background. (B) FAF of a GA lesion with diffuse hyper-AF background.
FAF patterns are also extremely useful to help differentiate atrophy secondary to AMD from that due to inherited retinal diseases (IRDs), which are often misdiagnosed as GA, such as Stargardt’s disease or its later onset form, fundus flavimaculatus. This distinction is now more important than ever as we consider treatments for GA secondary to AMD that will not be appropriate in cases where the atrophy is due to other causes. Additionally, we are entering an era where it will be possible to intervene in some of these IRDs, with appropriate gene therapy. Hence, identifying these cases has added significance so that people with IRD can also be appropriately referred for disease specific interventions.
OCT imaging provides additional and complementary information. OCT allows for other relevant biomarkers to be identified, such as the presence of reticular pseudodrusen (RPD), which are deposits located above the RPE, as distinct from conventional drusen that appear below the RPE.9 RPD are much more common than originally thought, with around a quarter of people with large drusen (intermediate AMD) having RPD, increasing to over half the population of those with GA.10 Presence of RPD is thought to reflect a retina with more dysfunctional RPE and may represent a disease stage more advanced, and harder to protect, than those AMD eyes without RPD.9,10 AMD eyes with GA and RPD have been found to have more rapid GA growth than those without RPD, and it even appears that the GA lesions grow faster in a region within the retina with RPD.11,12
On OCT B-scans, disruption of the ellipsoid zone, representing the photoreceptor mitochondrial band, has been reported as a possible biomarker for predicting the location of future GA progression.13 OCT imaging can also clearly identify how close the atrophic lesion is to the fovea, which is not so precise with FAF imaging, given the blocking of the AF signal around the fovea from the overlying luteal pigment.
There is considerable ongoing effort into exploring the use of artificial intelligence (AI) to develop algorithms that can consider imaging features as well as other parameters to help predict growth rates.14 Eventually, image analysis software, or AI algorithms, will undoubtedly be incorporated into standard imaging equipment to provide risk stratification tools that help identify high-risk characteristics, or aid in predicting progression rate and direction of progression. These AI tools will support the clinician in their decision making, but currently, until they can be implemented in the clinic, the best approach will be to become familiar with the imaging characteristics that can be identified right now to inform on individual GA lesion size, location, and identify features that impact growth rate.
OCT imaging also allows the early stages of atrophy to be seen that are not evident on FAF, colour fundus photographs or clinical examination (Figure 2). Signs indicating the beginning of cell death are those of hypertransmission of the OCT signal into the choroid, and disruption or attenuation of the RPE and loss of the outer retinal bands – the so called RPE and outer retinal atrophy (RORA).15,16 Specifically, the two key features of nascent GA (nGA): i) the subsidence of the outer plexiform layer (OPL) and inner nuclear layer (INL), or ii) a hypo-reflective wedge shaped band within Henle’s nerve fibre layer, are signs that indicate a very high risk of progression to GA.17,18

Figure 2. OCT B-scan showing the OCT signs of early atrophy. (A) Hyper transmission of the OCT signal into the choroid, disruption, or attenuation of the RPE, and loss of the outer retinal bands, so called RPE and outer retinal atrophy (RORA) (arrow). (B) Nascent GA (nGA) with the subsidence of the outer plexiform layer (OPL) and inner nuclear layer (INL), and hypo-reflective wedge-shaped bands within Henle’s nerve fibre layer (arrow).
Early identification of cases at high risk of progression to GA should trigger a different conversation about the potential treatments becoming available in the near future, compared to those without these high-risk signs. While all the current treatment trials require an atrophic lesion big enough to be accurately measured on FAF imaging (usually at least half a disc diameter) to be eligible for enrolment, being able to identify the signs that signify the start of the atrophic process will allow a more targeted conversation about potential treatments that they may need in the future, or potentially, treatments may well start earlier, once the real world and longer-term benefits are better understood and as treatments hopefully become less burdensome and carry less risk of adverse events.
New Treatments for GA
AMD is a complex, chronic disease with both genetic and environmental risk factors known to be important in its patho-aetiology. However, the underlying cause and chain of events that lead to progression are still not well understood and, as such, there are multiple different treatment approaches being considered.19,20
Trials at various stages of development are underway which target a diverse array of pathways such as i) reduction of oxidative stress, ii) reduction of toxic by-products by modulating the visual cycle, iii) neuroprotective approaches, iv) improved blood flow in the choroid, and v) replacing, repairing, or regenerating RPE cells and photoreceptors with cell-based therapies. However, the area with most activity and with intervention strategies furthest along in clinical development are those aiming to reduce inflammation by inhibition of the complement pathway.21 The complement pathway is a key component of the innate immune system and is well-established as being implicated in AMD pathogenesis.22
Pegcetacoplan
Pegcetacoplan, which inhibits complement factor 3 (C3), a protein critical to the complement pathway, is the compound that was approved for use in the US by the Food and Drug Administration (FDA) in February 2023.23
The Therapeutic Goods Administration is currently evaluating Syfovre for use in Australia. It is administered by intravitreal injections monthly, or every-other-month, on an ongoing basis and aims to slow GA growth. Both Phase 3 randomised controlled trials (DERBY and OAKS) demonstrated that pegcetacoplan slows GA lesion growth using FAF at 12 months – with only OAKS being statistically significant – the primary endpoint of the study.24 Additional follow-up to 24 months confirmed this reduced growth rate, which was significantly different from the growth rate in the sham group in both studies at 24 months. While treatment reduced the rate of atrophic lesion growth, at 12 and 24 months there was no significant difference in visual acuity between treated and sham groups.25 Subsequent post hoc analysis however, shows greater preservation of both the photoreceptor layer and RPE in the treated compared to the sham arm of these studies, reiterating the ability to save crucial retinal cells from dying, which will ultimately preserve visual function.26 Pegcetacoplan was well tolerated with manageable levels of adverse events. There was an increase in nAMD in the treatment arms compared with the sham arm, which will need to be considered in each individual case when contemplating treatment.24 In August 2023, several cases of vasculitis were reported with the real world use of pegcetacoplan, with none reported in any of the clinical trials, including the long-term extension study GALE. These cases are currently being investigated.
Avacincaptad Pegol
Avacincaptad pegol, also delivered via intravitreal injections, targets the complement cascade as a C5 inhibitor, and has been studied in the GATHER 1 and 2 trials. These Phase 3 trials have met their primary 12-month endpoint.27 The FDA approved the drug for use in the US in August 2023.28
While pegcetacoplan and avacincaptad pegol were the first to market, there are other novel interventions, both targeting the same complement pathway or different pathways, currently in clinical trials.
Other Options
Another trial underway in Australia and elsewhere, is the GOLDEN study, which uses an antisense inhibitor of complement factor B (Ionis-FB-LRx, Ionis) but, unlike pegcetacoplan and avacincaptad pegol, which are given via frequent intravitreal injections, the delivery of Ionis-FB-LRx is via a subcutaneous injection. This offers the exciting possibility of both in-the-home treatment and bilateral treatment of GA, although at the same time exposes the patient to systemic complement inhibition with potentially more systemic adverse events.29
Another strategy that aims for a once-off treatment is the administration of an agent via gene therapy. One such gene therapy trial, with patients from Australia currently enrolled, aims to increase the level of complement factor I, a key regulator of the pathway, through adeno-associated virus-based (AAV) gene therapy given via subretinal injection delivery (GT005, Gyroscope Therapeutics).30 GT005 aims to restore balance to an overactive complement system by increasing production of the complement factor I protein, which regulates the activity of the complement system.
Additionally, there are other complement pathway trials underway including ANX007 (Annexon), CB2782 (Catalyst), ALXN1720 (Alexion), HMR59 (Janssen) and Danicopan (Achillion), and even more in development, showing the immense interest from the pharmaceutical industry in this inflammatory pathway.
Other trials are targeting non-complement pathways, including ONL1204 (ONL Therapeutics), given via intravitreal injection and targeting the Fragment Apoptosis Stimulator (Fas) pathways upstream of the death signalling and inflammatory pathways.
Recently, Belite Bio announced that it intends to conduct a Phase 3 trial in Australia of its orally administered tablet, which aims to reduce the accumulation of toxins in the retina that are thought to contribute to GA and are by-products of the visual cycle. The oral administration, like subcutaneous injections, means that both eyes can be targeted with this delivery approach. However, this also exposes the individual to potential systemic adverse events, which are far less an issue with local delivery into the eye.
The Aims of GA Treatment
Unlike nAMD, where rapid vision loss and permanent scarring are the likely sequelae in an untreated eye, in GA, vision loss associated with a scotoma is often initially unnoticed by the patient. Additionally, although there is usually a relentless increase in scotoma size, the change of vision is not typically as dramatic.
The aim of treatment in nAMD is to prevent vision from deteriorating, with the hope that in many cases there will be an improvement in presenting vision if the lesion is caught early, once exudation occurs.
In GA the aim of treatment with pegcetacoplan and most other compounds currently under study, is to slow the decline in function. At this stage, potential treatments are unable to reverse or even stop this loss.
With pegcetacoplan, although the growth of the GA lesion area was significantly reduced in both Phase 3 trials at 24 months, there was no demonstrable significant difference in functional tests undertaken that included best corrected visual acuity, low luminance visual acuity, a number of different reading parameters, and retinal sensitivity as measured with microperimetry. Indeed, the expectation is that lesion size and visual function will get worse despite treatment, albeit at a slower rate than if left untreated. As such, the conversation with the patient needs to be around the additional time gained with useful central vision for activities such as reading or driving, rather than the ability to totally halt or reverse the changes in function already present.
Much like the treatment approach with some incurable cancers, where the aim is for additional survival time, conversations with GA patients need to set realistic expectations. With the first approved treatment requiring ongoing monthly or every other month intravitreal injections, the treatment commitment and likely benefits need to be clearly articulated.
Having access to an individual patient’s prior GA growth behaviour will be an enormous help when determining a clinical recommendation around the need to commence this long-term treatment. Knowledge of prior rates of lesion enlargement has been reported to be the most significant factor in predicting subsequent enlargement rates.10
Having sequential imaging, such as FAF or OCT will allow an assessment of growth rate as well as the presence or absence of biomarkers indicative of fast progression. Additionally, as there is no clinical measure that can be used to gauge early response to treatment (unlike when treating nAMD), success can only be measured as a change in rate of growth over an extended period. As such, growth rate prior to commencement of treatment will be the only comparator.
Imaging now, before patients start asking if they should get treatment, seems a very logical and highly desirable first step as we prepare for treatments to be approved in Australia.
We are at the dawn of a new era with a certainty that there will be more treatments to come. Before recommending the commencement of GA treatment, information about the GA lesion needs to be considered within the context of the patient age, visual needs, and ongoing quality of life issues.
Prepare Now for Treatments in Australia
Community-based eye care professionals are often the ones managing patients with GA, as these patients do not present acutely to hospitals, nor are they often referred to retinal specialists. Therefore, it is community-based optometrists who will often be first to identify people with GA, and as such start a discussion on the possibility of treatment options and offer an ophthalmology referral for further treatment discussion. Including any prior history, especially longitudinal imaging, in referrals will be useful to help determine the relative merits of intervening.
In some regions, practice patterns for managing people with GA may need to change to ensure these patients are seen by clinicians with multi-modal imaging capabilities so that a baseline assessment can be made, even before treatments are available. This will provide a valuable glimpse of the individual’s natural history when discussing the possibility of treatment.
While there can be significant differences in appearance of GA, depending on the FAF imaging device and acquisition parameters used (e.g., green- or blue-light FAF), as long as the images on an individual are performed on the same instrument, useful information will be captured to inform on the natural history of the GA. Increasing OCT scan densities (for example to 97 B-scans in a cube), with reduced distance between scans, would be ideal to capture all relevant anatomical change that might inform risk features for growth, distance from the fovea and allow en face visualisation.
By starting to image our GA patients now, we will all be in the best position to counsel our patients individually on the risks and benefits of treatment for GA. Ideally FAF and OCT images can be captured to document the baseline extent of GA, identify any risk factors for progression, document progression rate before any potential treatment, and ensure the patient doesn’t have an IRD that has been misdiagnosed. In this way, we will be better equipped to collaboratively manage our GA patients when treatments arrive on our doorstep.
 Professor Robyn H. Guymer AM MBBS FRANZCO PhD is an ophthalmologist with medical retinal subspeciality training. She is Professor of Ophthalmology at the University of Melbourne and Deputy Director of the Centre for Eye Research Australia. Prof Guymer sits on advisory boards of Apellis, Genentech, Roche, Novartis, and Bayer.
Professor Robyn H. Guymer AM MBBS FRANZCO PhD is an ophthalmologist with medical retinal subspeciality training. She is Professor of Ophthalmology at the University of Melbourne and Deputy Director of the Centre for Eye Research Australia. Prof Guymer sits on advisory boards of Apellis, Genentech, Roche, Novartis, and Bayer.
 Carla J. Abbott BOptom PhD PGDipOcTher is a therapeutically endorsed optometrist and Senior Research Fellow at the University of Melbourne and the Centre for Eye Research Australia.
Carla J. Abbott BOptom PhD PGDipOcTher is a therapeutically endorsed optometrist and Senior Research Fellow at the University of Melbourne and the Centre for Eye Research Australia.
References
1. RANZCO referral pathway for AMD management, available at: ranzco.edu/home/health-professionals/referral-pathway-for-amd-management [accessed 8 August 2023].
2. Hart, K. M., Abbott, C., Ly, A., et al., Optometry Australia’s chairside reference for the diagnosis and management of age-related macular degeneration (2020). Clinical and Experimental Optometry, 103(3), 254–264.
3. Keel, S., Xie, J., Foreman, J., et al., Prevalence of age-related macular degeneration in Australia: The
Australian National Eye Health Survey. Jama Ophthalmol.2017;135:1242–49.
4. Fleckenstein, M., Bailey, M., Freund K.B., et al., The progression of geographic atrophy secondary to age-related
macular degeneration. Ophthalmology. 2018;125:369–390.
5. Schmitz-Valckenberg, S., Sahel, J.A., Danis, R., et al., Natural history of geographic atrophy progression
secondary to age-related macular degeneration (Geographic Atrophy Progression Study). Ophthalmology.
2016;123:361–368.
6. Lindner, M., Boker, A., Mauschitz, M.M., et al., Directional kinetics of geographic atrophy progression in age-related macular degeneration with foveal sparing. Ophthalmology.2015;122:1356–1365.
7. Fleckenstein, M., Schmitz-Valckenberg, S., Adrion, C., et al., Progression of age-related geographic atrophy: Role of the fellow eye. Invest Ophthalmol & Vis Sci. 2011;52:6552–6557.
8. Holz, F.G., Bindewald-Wittich, A., Fleckenstein, M., et al., Progression of geographic atrophy and impact of
fundus autofluorescence patterns in age-related macular degeneration. Am J Ophthalmol. 2007;143:463–472.
9. Greferath, U., Guymer, R.H., Vessey, K.A., et al., Correlation of histological features with in-vivo imaging of reticular pseudodrusen. Ophthalmology. 2016;123(6):1320–31.
10. Wu, Z., Fletcher, E.L., Kumar, H., et al., Reticular pseudodrusen: A critical phenotype in age-related macular
degeneration. Prog Ret Eye Res. 2022; 88:101017.
11. Marsiglia, M., Boddu, S., Bearelly, S., et al., Association between geographic atrophy progression and reticular
pseudodrusen in eyes with dry age-related macular degeneration. Invest. Ophthalmol. Vis. Sci. 2013;54: 7362–7369.
12. Thiele, S., Nadal, J., Pfau, M., et al., Prognostic value of intermediate age-related macular degeneration phenotypes for geographic atrophy progression. Br. J. Ophthalmol. 2021;105: 239–245.
13. Giocanti-Auregan, A., Tadayoni, R., Fajnkuchen, F., et al., Predictive value of outer retina en face OCT imaging for geographic atrophy progression. Invest Ophthalmol Vis Sci.2015;56:8325–8330.
14. Vogl, W.D., Riedl, S., Mai ,J. et al., Predicting topographic disease progression and treatment response of
pegcetacoplan in geographic atrophy quantified by deep learning. Ophthalmol Retina. 2022;6:501–511.
15. Sadda, S.R., Guymer, R., Holz, F.G., et al., Consensus definition for atrophy associated with age-related macular
degeneration on OCT: Classification of atrophy report 3.Ophthalmology. 2018;125(4):537–48.
16. Guymer, R.H., Rosenfeld, P.J., Curcio, C.A., et al., Incomplete retinal pigment epithelial and outer retinal atrophy in age-related macular degeneration: Classification of atrophy meeting report 4. Ophthalmology 2020;127:394–409.
17. Wu, Z., Luu, C.D., Ayton, L.N., et al., Optical coherence tomography-defined changes preceding the development
of drusen-associated atrophy in age-related macular degeneration. Ophthalmology. 2014 Aug 8;121(12):2415–22.
18. Wu, Z., Luu, C.D., Hodgson, L.A.B., et al., Prospective longitudinal evaluation of nascent geographic atrophy
in age-related macular degeneration. Ophthalmol Retina 2020;4:568–575.
19. Guymer, R.H., Campbell, T.C., Age-related macular degeneration. Lancet 2023 29;401:1459–1472.
20. Fleckenstein, M., Keenan, T.D.L., Guymer, R.H., et al., Age-related macular degeneration. Nat Rev Dis Primers.
2021;7:31.
21. Li, H., Chintalapudi, S.R., Jablonski, M.M., Current drug and molecular therapies for the treatment of atrophic age-related macular degeneration: phase 1 to phase 3 clinical development. Expert Opin Investig Drugs. 2017;26:1103–14.
22. Hageman, G.S., Anderson, D.H., Johnson, L.V. et al., A common haplotype in the complement regulatory gene
factor H (HF1/CFH) predisposes individuals to age-related macular degeneration. PNAS 2005;102: 7227–7232.
23. FDA approves Syfovre (pegcetacoplan injection) as the first and only treatment for geographic atrophy, a leading cause of blindness (media release, 17 February 2023) available at: investors.apellis.com/news-releases/news-release-details/fda-approves-syfovretm-pegcetacoplaninjection-first-and-only. [Accessed 17 February 2023].
24. Goldberg, R., Heier, J.S., Wykoff, C.C., et al., Efficacy of intravitreal pegcetacoplan in patients with geographic
atrophy: 12-month results from the phase 3 OAKS and DERBY studies. Invest Ophthalmol Vis Sci. 2022;63:1500–00.
25. Hutton, D., (24 April 2023). ARVO 2023: Data outlines phase 3 functional analyses of pegcetacoplan injection for geographic atrophy. Available at: ophthalmologytimes.com/view/arvo-2023-data-outlines-phase-3-functionalanalyses-of-pegcetacoplan-injection-for-geographic-atrophy [accessed 8 August 2023].
26. Riedl, S., Vogl, W.D., Mai, J., et al., The effect of pegcetacoplan treatment on photoreceptor maintenance in geographic atrophy monitored by artificial intelligence–based OCT analysis. Ophthalmol Retina. 2022; 6:1009–1018
27. Jaffe, G.J., Westby, K., Csaky, K.G., et al., C5 inhibitor avacincaptad pegol for geographic atrophy due to age-related macular degeneration: a randomized pivotal phase 2/3 trial. 2021;128:576–86.
28. Astellas Pharma Inc., Iveric Bio receives US FDA approval for Izervay (avacincaptad pegol intravitreal solution), a new treatment for geographic atrophy (media release, 4 August 2023) available at: prnewswire.com/news-releases/iveric-bio-receives-us-fda-approval-for-izervay-avacincaptadpegol-intravitreal-solution-a-new-treatment-for-geographicatrophy-301894042.html [accessed 8 August 2023].
29. Halawa, O.A., Lin, J.B., Miller, J.M. et al., A review of completed and ongoing complement inhibitor trials for
geographic atrophy secondary to age-related macular degeneration. J. Clin. Med. 2021, 10(12), 2580.
30. Kiss, S., Interim results from a first-in-human phase I/II gene therapy study (FOCUS) of GT005, an investigational AAV2 vector encoding complement factor I, in patients with geographic atrophy. Presented at Retina Society; 30 September, 2021; Chicago, IL.
More paragraph text
Table Box Title |
|---|
| Table of info towards the bottom of the article. We will look to see if there is an easier way to build these for you as this is not ideal, but inherited from the old Red5 CMS |
Final information about the author





