

We experience the world through our senses and around three in four Australians (76%) consider eyesight as their most important sense.1 For us to live to our full potential, looking after our health, wellbeing, and eyesight must be a priority. Interestingly, over half of Australians (59%) worry about the quality of their eyesight, yet are anxious about visiting an optometrist.
This article will review how we can best personalise, support, and influence new contact wearer’s experiences to increase compliance, maximise the chance of success, and reduce the likelihood of early contact lens drop out.
Demand for eye health and contact lens services will continue to increase, due to the rising incidence of ocular disease. The prevalence of myopia for example, is expected to be nearly 50% of the population by 2050.2 With more requirement for refractive correction, there has never been a better time to recommend contact lenses.
As well as providing visual and practical benefits, contact lenses can make a real difference to a person’s quality of life, by positively impacting their emotional and physical state of mind.3 Yet despite these health and wellbeing advantages, as mivision has previously reported, Australia has one of the world’s lowest contact lens uptakes by spectacle wearers.4
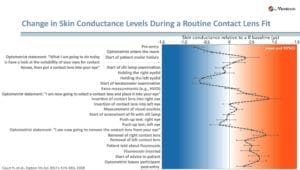
Figure 1. Anxiety level changes during contact lens fitting.5
Key psychological barriers to contact lens wear include perceptions of difficulty applying and removing contact lenses, and wearer discomfort.1
Although potential new wearers may have a high desire to wear contact lenses, this unfamiliar experience may lead to initial feelings of uncertainty or apprehension. Not surprisingly, research by Courts et al., found an association between patient anxiety, patient satisfaction, and retention of information during the contact lens fitting journey (Figure 1).5 The findings may help explain why there are reported discrepancies between information eye care practitioners (ECPs) believe to have provided patients versus that which patients recall receiving. They are a valuable reminder of the importance of reiterating key messages.
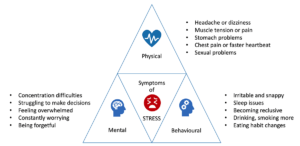
Figure 2. Adapted from the United Kingdom’s National Health Service (NHS) website.6
MANIFESTATION OF EMOTIONAL RESPONSES
Stress triggers can occur if the patient isn’t at ease with the practitioner, doesn’t feel they are able to share their concerns or thoughts, or feels a lack of control. Figure 2 reflects typical mental, physical, and behavioural changes associated with stress.6 As practitioners, we should look for symptoms of stress, such as closed body language and changes in behaviour.
HOW CAN WE SUPPORT?
Communication, rapport, and the relationship with the patient are vital for a positive contact lens experience. Getting the basics right could be as simple as ensuring the patient is seated comfortably, offering them water, and taking time to allay them of any concerns they may have.
Referring to why they want to wear contact lenses and linking this to the benefits during their everyday activities is a powerful motivator to help reduce the chance of drop out. Figure 3 highlights some of the advantages of contact lenses.
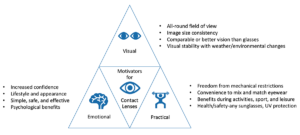
Figure 3. Benefits of contact lenses adapted from the BCLA.7
HELP PATIENTS REMAIN CALM
Inside the Consultation Room
When fitting a patient for the first time with contact lenses:
Get to know the patient as a person. Ask about their lifestyle, taking interest in their hobbies and activities, pets, and family. A patient will feel most relaxed when talking about things that bring them joy.
Discover why they personally want contact lenses. Establishing their reason for contact lens wear will be a great motivator throughout the journey.
Ask if they have heard about experiences of others or have any questions. This is a great way to reveal preconceived views on contact lenses.
Reassure and validate. Reassure your patient that no worry is too small and invite them to share any further worries.
Show them what contact lenses look like. Allow them to hold and touch them. Explain what makes contact lenses so great, and how they are designed to ensure ease of handling and fit on the eye.
Outside the Consultation Room
When teaching the patient about contact lenses:
Prepare well. Ensure the environment is clean, safe, and clutter free, with all resources easily accessible. Calming music in the background can help reduce anxiety.8
Promote compliance and best practice. Instil good habits from the outset, such as correctly washing and thoroughly drying hands.
Use a range of learning resources. Invite the patient to watch a video on lens application and removal. If the teaching session is booked on a separate day, ask the patient to prepare by touching parts of their eye, like the lids and lashes, and holding their blink for a few seconds. Be sure to discuss the need for hygiene before they do this.
Reassure and offer empathy. Advise the patient what will happen during the teaching session; reassure them that there is plenty of time to ask questions and practice application and removal. Remind them that it’s normal to feel nervous when they are doing something new.
Be adaptive and responsive. If the patient becomes disheartened, let them know it usually takes a few attempts to successfully apply and remove contact lenses. You might let them know it took you more than a few attempts to master it. Remind them of their motivation driver.
Look for heightened stress signs. Personalise the journey by giving as many breaks as needed. Distract and relax them by asking about their hobbies and interests (general life talk). Give them steps to practise between sessions.
Checklists and feedback. Once the teaching session is successful and the lens has settled, it’s very important to praise the patient on excellent technique before asking how they are feeling and how the lens feels.
Patients may not have retained all the information provided.7 This makes it important to provide various written and/or digital materials to reiterate key messages.
Check in. Let your patient know that their satisfaction and happiness with their new contact lenses is important to you and, as a courtesy, you will call them to check how they are getting on.
Outside the Practice
When talking to patients about ongoing wear of contact lenses:
Provide appropriate advice and support. Ensure the wearer understands how to best seek guidance, both during and out of practice opening hours. Consider resources such as videos to support the learning process.
Follow-up. Contact lens handling, vision and discomfort are three of the key reasons new patients cite for dropping out of lens wear.9
This makes it critical to listen carefully and communicate clearly about any concerns they have. Early contact during the first week will help address any concerns and act as a catalyst for further decision-making. Figure 4 provides a holistic overview of key touch points during the new contact lens wearer’s journey.
Look for changing patterns of lens wear. Patients adapt their contact lens wear schedule for different reasons. One perspective put forward by Dr David Stephenson is that ‘working from home has disrupted patients’ contact lens wear’. He found that that those who began to work more from home reduced their contact lens wear and chose to wear glasses.
Similarly, people suffering from mental health issues may reduce their contact lens wear if they become more withdrawn, spend less time socialising, and more time alone at home.
It is important to converse with patients to understand their reason for reducing their contact lens wear or not wearing them at all. Choosing different lens options and adjusting to suit the patient’s lifestyle can avoid them ceasing lens wear altogether.10
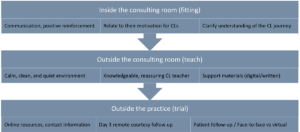
Figure 4. Touch points to maximise success during the contact lens journey.
MAKE HANDLING SIMPLER
When you understand differences between products, you can provide specific guidance that will improve patient reported outcomes rather than relying on visual acuity assessment alone.
Features, such as shape retention, edge design and surface properties can all impact contact lens handling. If the lens is too floppy it may stick to the finger. If it is too slippery, it may be difficult to remove from the packaging without damaging the lens.
Modality also has an impact. For example, it has been reported that reusable soft lenses require around double the number of compliance steps as daily disposable soft lenses.11
If the lens dehydrates on the eye and the fitting behaviour becomes tighter with insufficient lens movement, removal may become more challenging. This may occur if a wearer has slept in the contact lens or experiences dry eye. Advising the patient to use rewetting drops / saline to help mobilise the lens before removal can be beneficial. A contact lens review may also be necessary.
Manufacturers have responded to handling concerns by adding tints to make the lenses more visible on the eye, and markers to help identify correct orientation and ensure the lens is removed from the packaging the correct way up.
It is particularly important to explain the marker on a toric contact lens as this can be used to quickly achieve the desired lens position on the eye for optimal vision.
Patients prescribed multifocal designs for presbyopia should be advised of the likelihood of an adaption period of up to 10 days.12
Different patients will also have different preferences. Some, for example, may prefer the stiffness of handling a lens with a higher modulus.
MENTAL HEALTH AND DRY EYE
An association between mental health and dry eye disease has been reported in the literature, with nearly half (47%) of those with dry eye reporting mental health issues.13 This may, to varying levels, be influenced by the side effects of medications prescribed to these individuals as many such drugs can result in ocular manifestations such as dry eye, reduced accommodation, higher intraocular pressure / glaucoma risk, and visual changes.14
As contact lens wear can elicit dry eye symptoms and signs, a prudent approach in patients at high risk is to follow the Tear Film and Ocular Surface Society (TFOS) DEWS II guidance, ensuring a comprehensive dry eye assessment is conducted.15
Researchers have established various questionnaires that are available to assess health status, disease severity, and any impact on quality of life. These include:
- VFQ-28R (visual function on quality of life, activity limitations), • EQ-5D-5L (five dimensions of health status, daily basis),
- WPAI (work productivity and activity impairment), and
- IDEEL (impact of dry eye on everyday life).
Introducing these questionnaires alongside more traditional dry eye questionnaires can help build a better picture of not just the patient’s ocular status, but also the overall impact of contact lenses on physical and mental wellbeing.
CONCLUSION
Approximately one in four new wearers report handling issues as a key reason for contact lens drop out,16 however this is something that can easily be avoided and addressed with education.
Reassurance regarding contact lens misconceptions can also reduce the risk of drop out. Patients, for example, need to be reassured that the contact lens cannot get stuck behind the eye, although there is the potential for short-term retention in the eyelid fornix.17
By understanding each patient’s emotional and physical responses to contact lenses, we can tailor our approach to suit.
Ensuring a well-educated, customer-centric team with a diverse knowledge of best practice approaches for different lens requirements, and stocking a variety of patient facing resources will ensure each new contact lens wearer has the best chance of success.
Interestingly, non-wearers do not appear to fully appreciate the psychological benefits that contact lens wear provides when compared to wearers, so avoid making presumptions and be proactive with recommendations.18
Everyone is unique in the way they see, hear, respond, and learn. Giving a personalised service will ensure their needs are heard and met, and their experience will be productive, positive, and exciting. Keep the process simple and fun.
*Patient names changed for anonymity.
This article is adapted from an article originally published in Optician.
Neil Retallic is an optometrist with experience working in practice, education, industry, and head office roles. He currently works for the College of Optometrists and Specsavers in the United Kingdom. He has been involved with various organisations across the sector and is the immediate past President of the British Contact Lens Association.
Sheena Tanna-Shah is an optometrist working in practice, based in the United Kingdom. She is also an author, rapid transformation therapy practitioner, life coach, mindfulness, meditation, neuro-linguistic programming practitioner, and nutritionist.
References
- Empirica Research, The 2020 Vision Index: Taking a closer look at Australia’s eye health, available at: optometry. org.au/wp-content/uploads/GVFL/Vision_Index/2020- Vision-Index-Report-FINAL.pdf [accessed 9 August 2023].
- Holden B., et al., Global prevalence of myopia and high myopia and temporal trends from 2000 through 2050. Ophthalmology. 2016 May;123(5):1036–42.
- Retallic, N., The person behind the contact lens. Optician. 17 September 2021.
- ‘Massive’ industry campaign to boost contact lens sales, mivision, 15 May 2022 available at: mivision.com. au/2022/05/massive-industry-campaign-to-boost-contactlens-sales [accessed 9 August 2023].
- Court H., et al., Evaluating patient anxiety levels during contact lens fitting. Optom Vis Sci. 2008: Jul;85(7):574–80.
- National Health Service, Stress (webpage), available at: nhs.uk/mental-health/feelings-symptoms-behaviours/ feelings-and-symptoms/stress [accessed 9 August 2023].
- British Contact Lens Association (webpage), available at: bcla.org.uk/Public/Consumer/Benefits_of_contact_lenses. aspx [accessed 9 August 2023].
- Thoma M., et al., The effect of music on the human stress response. PLoS One. 2013: Aug 5;8(8):e70156PMC3734071.
- Wolffsohn, J., et al., CLEAR – Evidence-based contact lens practice. Cont Lens Anterior Eye.2021 Apr;44(2):368–397.
- Morgan P.B., Sulley A.L., Challenges to the new soft contact lens wearer and strategies for clinical management. Cont Lens Anterior Eye. 2023 Jun;46(3):101827. doi: 10.1016/j.clae.2023.101827. Epub 2023 Mar 17. PMID: 36935225.
- Efron, N., Morgan, P., Rethinking contact lens aftercare. Clinical and Experimental Optometry. 2017: Volume: 100, Issue: 5, Pages: 411–431,
- British Contact Lens Association, Important Do’s and Don’ts of Contact Lens Wear (webpage) available at bcla.org.uk/Public/Consumer/Important_dos_and_ dont_s_of_contact_lens_wear.aspx [Accessed 9 August 2023].
- Hossain P., et al., Patient-reported burden of dry eye disease in the UK: a cross-sectional web-based survey. BMJ Open 2021.
- Gherghel D., Ocular side effects of system drugs3- Central nervous system agents. Optician. 22 May 2020; 18–22.
- Wolffsohn J.S., et al., TFOS DEWS II Diagnostic Methodology report. Ocul Surf. 2017 Jul;15(3):539-574.
- Sulley, A., et al., Factors in the success of new contact lens wearers. Cont Lens Anterior Eye. 2016;40:1 15-24.
- Retallic, N., Nagra, M., Contact lens handling. Contact Lens Spectrum: Volume:38: June 2023: 36–40.
- Naroo, S., et al., Exploring contact lens opportunities for patients above the age of 40 years. Cont Lens Anterior Eye. 2022 Dec;45(6):101599.
- Ramamoorthy P., Nichols J., Compliance factors associated with contact lens related dry eye. Eye Contact Lens.2014:40(1):17–22.
- Wolffsohn, J., et al., British Universities Committee of Contact Lens Educators (BUCCLE). History and symptom taking in contact lens fitting and aftercare. Cont Lens Anterior Eye. 2015 Aug;38(4):258–65.
- BMG Research, GOC Contact Lens Survey (2015)
CASE ONE: THE SPORTSMAN
Mark*, a 32-year-old male, attended for a contact lens consultation. He had unsuccessfully tried contact lenses four years ago and immediately given up. Having taken up sports, he had decided to trial contact lenses again, but wasn’t confident of a positive outcome. Mark was not on any medication. He had no contact lens contraindications or dry eye.
I gave him a motivational boost with some encouraging words and we had an interactive discussion about what to expect. I showed him a video on handling contact lenses and gave him the opportunity to handle some lenses. By this time he had visibly relaxed.
Careful questioning revealed that Mark’s primary concern was breaking or losing a contact lens. This was overcome with reassurance. I addressed common myths about losing contact lenses on eye and suggested he take a few deep breaths before giving contact lenses a go.
With the support of consistent positive language throughout the teaching session, Mark scored his confidence in handling as 7/10. On repeating the process, his score improved to 9/10.
I reminded Mark of the ‘dos and don’ts’ of contact lens wear and provided him with a checklist created by the British Contact Lens Association (BCLA) (Figure 5). I made sure he was happy, was satisfied with the advice I’d provided, and that he had no doubts or concerns as he left the practice. I also let him know that I would call him in a few days to check on how he was getting on.
Mark was absolutely delighted with the whole experience and felt confident that he would enjoy playing sport now that he could successfully wear contact lenses. Figure 6 demonstrates his emotional journey.

Figure 5. BCLA eye care practitioner and patient resources.11

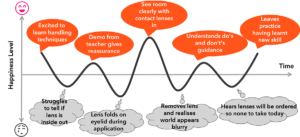
Figure 6. Emotional journey during the teach process.
CASE TWO: HANDLING DIFFICULTIES
Laura*, at 22-years-old, was fitted with daily disposable contact lenses. When telephoned three days after the initial fit, she was enthusiastic, sharing how she loved wearing her contact lenses and the newfound confidence they provided.
She answered yes to the three key questions highlighted in Figure 7:
Do you see well?
Do your eyes look good?
Do they feel good?

Figure 7. BCLA guidance on three questions that wearers should regularly ask themselves.11
Laura positively responded to all aspects except handling, which rated as 6/10, especially application. We agreed to switch to a video call so she could demonstrate her technique.
I observed that she was not holding her eye lids firmly open. I advised her on how to adapt her approach, keeping both eyes open. When she returned for follow-up she described her contact lens journey at home as shown in Figure 8.
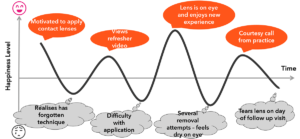
Figure 8. Emotional journey while at home
CASE THREE: THE HYGIENE RISK
Karl*, 25, attended my practice for a routine annual contact lens check-up. He reported that he was happy with his contact lenses.
During the consultation I asked him to demonstrate the removal and application of his contact lenses, noting in the process that he did not wash or dry his hands prior to removal. Surprisingly, despite the risks, up to 50–60% of lens wearers admit to a lack of correct handwashing.19,20 Yet a survey revealed that not all eye care practitioners routinely observe compliance-related behaviours during contact lens follow-up consultations.20
To encourage compliance with contact lens hygiene procedures, I reminded Karl of his motivation for contact lenses and linked this with how he would feel if he was no longer able to wear them.
This approach is usually more effective than using ‘scare’ tactics with horror stories of sight-threatening infections.21
Contact lens hygiene should not be overlooked as, in the absence of proper handwashing, the risk of contact lens infection increases by about 4.5 times.9





