

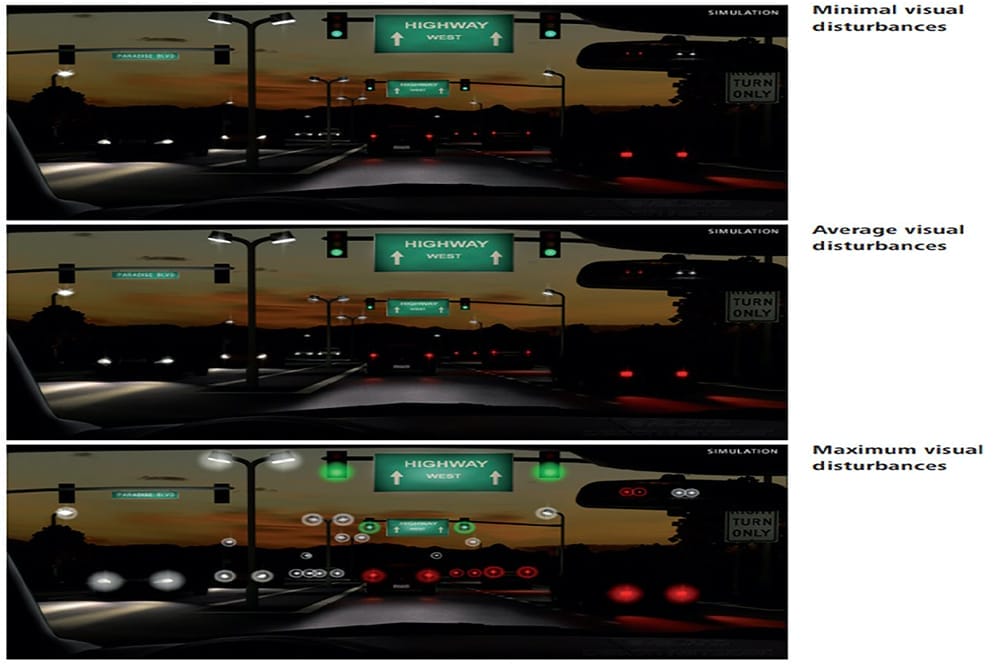
Figure 2. Glare simulator showing minimal, average, and maximum visual disturbances at nighttime from a diffractive IOL.
As a cataract and refractive specialist, Dr Armand Borovik sees a large proportion of presbyopic and cataract patients who wish to gain independence from glasses or contact lenses. This can be achieved through either corneal refractive surgery to give the patient monovision, or through lens-based surgery. Here, he provides advice on talking to patients about presbyopia correcting intraocular lenses.
In Australia, we are fortunate to be able to offer our patients the latest technology in presbyopia correcting intraocular lenses (PC-IOLs) and in my experience, patients are extremely happy with their post-operative results. A recent survey demonstrated that following cataract surgery, patients who received PC-IOLs felt more positive about ageing and had an improved quality of life relative to those who received monofocal lenses.1
To keep up with increasing demand, the proportion of PC-IOLs I implant has increased significantly, to the point where a PC-IOL is my standard of care for all appropriate patients.
To achieve the highest level of satisfaction, it is critical to appropriately counsel a patient about their options and work with them to determine the particular lens that will best meet their visual needs.
EVOLUTION OF IOLS
Cataract surgery is the most common elective surgery performed in the world, with an estimated 20 million procedures performed annually.2 In Australia, approximately 225,000 cataract procedures are performed each year.3 For many years, since the widespread uptake of cataract extraction and insertion of intraocular lenses (IOLs), the only options were monofocal IOLs or more recently, monofocal toric IOLs.
Over the past decade or so, new and evolving technologies have changed the landscape in which Australian ophthalmology is practised. We now have a plethora of choice when it comes to offering patients more than a single focal point in their IOL. In fact, it could be argued that monofocal lenses are becoming a “special use” lens with limited applications in modern day practice. This is a complete paradigm shift when it comes to thinking about how we help patients choose the appropriate IOL for their surgery.
CHANGING VISUAL NEEDS
Increasingly, our lives revolve around interacting with devices such as laptops, phones, and the dashboard of our cars. This means our patients’ demands for unaided intermediate (63 cm) and near (40 cm) vision is increasing.4 It is therefore, prudent for ophthalmologists to offer presbyopia correcting IOLs to their patients to truly fulfil their desire for reduced spectacle dependence across their tasks of daily living.
This makes it increasingly important for optometrists, as primary eye care providers, to understand the range of presbyopia correcting IOLs available and the suitability of patients for particular lenses.
A recent article in the American Journal of Ophthalmology sought to find consensus among world experts in lens and refractive surgery regarding guidelines for the use of presbyopia correcting lenses.4 They reached consensus on the following key criteria for diffractive multifocal IOLs: to be used in patients with potential post-operative visual acuity >0.5, keratometry between 40–45 dioptres, pupil diameter of >2.8 mm under photopic conditions and <6.0 mm under scotopic conditions, and a root mean square of higher order corneal aberrations <0.5 µm). Additionally, they advised that monofocal or non-diffractive IOLs should be considered for patients with coexisting eye disorders or those not meeting the agreed criteria. However, they were unable to reach a consensus regarding criteria for patient selection for PC-IOLs, suggesting this process is still somewhat of an elusive science.
In my own practice, approximately 95% of the lenses that I implant are now PC-IOLs, with 60% of these being extended depth of focus (EDOF) lenses, 35% diffractive multifocal lenses, and 5% monofocal lenses. Patients receive a monofocal lens if they have specific ocular co-morbidities that are contraindicated in PC-IOLs. Recent improvements in the optics of PC-IOLs and improved accuracy of biometry, combined with appropriate patient selection and counselling, have resulted in an extremely high satisfaction rate in my presbyopic patient cohort.
Optometrists play a crucial role in the care of patients undergoing refractive lens exchange or cataract surgery. They have often had a long relationship with their patient and understand their visual needs and refractive history. Working with the ophthalmologist, optometrists can be an invaluable part of the process by providing a history of the patient’s visual needs, previous use and tolerance of multifocal glasses or contact lenses, and feedback on conversations with the patient about postoperative aims and expectations.
PRESBYOPIA CORRECTING INTRAOCULAR LENS OPTIONS
Broadly speaking, PC-IOLs can be divided into two commonly used subtypes: multifocal IOLs (MF IOLs), which split light into multiple foci, whether they be bifocal or trifocal through diffractive optics, and EDOF IOLs, which create a prolonged focal point to give patients distance and intermediate vision through different mechanisms.
In practical terms, presbyopia correction is an interplay of three factors:
- Visual quality,
- Depth of field, and
- Potential post operative dysphotopsias.5
MF IOLs can provide additional near vision compared to EDOF lenses, but that comes at the expense of an increased chance of postoperative dysphotopsias, and loss of contrast due to the diffractive mechanism of light splitting by the MF IOLs. This knowledge can help to guide lens selection, taking into account a patient’s visual needs and potential tolerance of these side effects.

Figure 1. Pre-consultation questionnaire
Working Through the Selection Process
When considering lens selection with my patients, I ask them to complete a clinical questionnaire (Figure 1). The questionnaire helps elucidate the following valuable information about their lifestyle, hobbies, and visual preferences, all of which is integral to lens selection:
To find out about the patient’s lifestyle and visual requirements, I ask about their vocation and hobbies.
If a patient is a professional truck driver, I will tend to advise against a diffractive IOL as the potential glare at night might compromise the visual function required for their work. In these cases, I generally recommend an EDOF IOL, and have found this to result in happy outcomes for this cohort. If a patient is active and plays a lot of sports, then an EDOF IOL may also be preferred to maximise their distance and intermediate vision.
However, if a patient sews or is an artist, then an MF IOL may be the preferred option. To understand the patient’s expectations about wearing glasses post-surgery, I ask them to indicate which focal length they would mind wearing glasses for: distance, intermediate or near vision? Most patients circle that they don’t like wearing glasses for any distance. However, not infrequently they will say they don’t mind glasses for near work as they wish to prioritise distance and intermediate vision, making them an ideal candidate for an EDOF lens.
I predict a patient’s tolerance of dysphotopsia in two ways: by directly asking whether they are willing to tolerate glare and, with an indirect question to help determine their personality type; “How would your friends describe your personality?”.
Traditionally, ‘Type A’ personalities, such as engineers who are very meticulous, were considered poor candidates for diffractive IOLs as they would ‘nitpick’ the associated visual phenomena they experience and be dissatisfied. In my practice, however, these patients are still suitable for all lens types if they are given appropriate counselling. All they need is to be aware of what to expect – they don’t tend to like surprises but if they expect glare and haloes then they are more likely to tolerate them.
The patient’s responses to the questionnaire usually provides me with a good understanding about the lens to select for their surgery.
Glare Simulator
In my experience, it is essential to show patients a glare simulator that gives them an idea of what to expect in their visual system after implantation of an MF IOL. There are various simulators available, however I use the simulator shown in Figure 2 as it demonstrates the most severe outcome that may occur. Although it is rare, I make sure patients know this ‘severe’ outcome may in fact be their visual experience post-surgery. I will only recommend an MF IOL if they say they already have similar phenomena, or that they wouldn’t be bothered by the glare in exchange for independence from glasses. Additionally, patients who do not drive at night or patients in nursing homes make ideal MF IOL candidates as the issue with glare is not relevant for them.
In the past, much has been discussed about dysphotopsias causing patient dissatisfaction post-surgery, however in my experience, there is a greater degree of dissatisfaction as a result of post-operative residual refractive error and uncorrected astigmatism. A 2011 study by de Vries et al.,6 assessing patient symptoms after MF IOL surgery, found that residual ametropia and astigmatism, posterior capsule opacification, and a large pupil were the three most significant aetiologies in post-surgical patient dissatisfaction. Post-operatively, 64 eyes (84.2%) were amenable to therapy with either refractive surgery, glasses, or laser capsulotomy.
One way to assess this post-operatively is to do a contact lens trial correcting their residual refractive error. If this improves their symptoms, then correcting their residual refractive error will most likely alleviate their symptoms. This also assists in the decisionmaking process around whether to proceed with a YAG capsulotomy, which makes an IOL exchange more challenging with a higher risk of complications.7
A recent patient experienced severe dysphotopsia after MF IOL implantation. Her residual refractive error was -0.5 in each eye, and she had mild-to-moderate posterior capsular opacification. Her treating surgeon had advised her that dry eyes were to blame for her symptoms, however a contact lens trial resolved her dysphotopsias and we decided to proceed to a capsulotomy to improve the accuracy of the subsequent laser refractive surgery we were planning. Interestingly, all of her symptoms resolved after the capsulotomy and as such, she did not require any additional intervention.
In offering patients PC-IOLs, it is useful for the treating surgeon to be able to correct any residual refractive error or have a pathway to offer post-operative refractive touch-ups to achieve the optimal result for the patient.

Figure 3. Angle kappa is the angular value between the pupillary axis and the visual axis whereas angle mu or the Chang Waring chord is the two-dimensional distance between the centre of the pupil and the subject-fixated coaxially-sighted light reflex
Technical Evaluation and Considerations
Chord Mu or Chang Waring Chord
Traditionally, angle kappa was used to assess for centration when considering MF IOLs. This is the angular value between the pupillary axis and the visual axis,8 whereas chord mu is the two-dimensional distance between the centre of the pupil and the subject-fixated coaxiallysighted corneal light reflex (Figure 3).9
Multiple machines, including the ZEISS IOL Master 700 (IOLM 700) and the ZEISS Atlas, measure the apparent chord mu, however the true chord mu is smaller. The placement of an IOL is ideal if it is placed on the visual axis or between the pupillary centre and the visual axis. This happens when the chord mu is minimal.10 This is an important factor to consider to ensure that the patient’s visual axis falls inside the central optical zone of a diffractive IOL and hence decreases the risk of them experiencing significant postoperative dysphotopsias.
Common diffractive IOLs have different central optical zone sizes, ranging from 1.04 mm (ZEISS At Lisa, Carl Zeiss Meditec, Jena, Germany) to 1.164 mm (Clareon Panoptix, Alcon Laboratories, Fort Worth, Texas, USA). Different cutoffs for the value of chord mu have been recommended but are generally based on a measure approximately half the size of the central optical zone of these lenses, which increases the chance of the central zone of the lens centering over the visual axis. A common cut off is a chord mu of less than 0.6 mm, which is the figure that I use. Figure 4 shows the IOLM 700 light reflex for a patient with a chord mu of 0.68 mm with the central optic of an MF IOL superimposed over the centre of the pupil. It can be seen that light passing through the coaxial light reflex will intersect with the edge of the diffractive rings and hence increase the chance of this patient having more dysphotopsias and decreased quality of vision. This patient was excluded from receiving a MF IOL and was implanted with an EDOF lens instead.

Figure 4. A diffractive multifocal IOL superimposed on the image of a patient’s eye with a large Chang Waring chord.
Corneal Higher Order Aberrations
One of the main pathologies I assess for, when considering a patient for a PC-IOL, is their corneal morphology. Traditionally, a cutoff of 0.5 root mean square for overall corneal higher order aberrations (HOAs) has been used as a benchmark for exclusion of patients for MF IOLs.4 This number can be measured directly on various aberrometers or on more commonly used devices such as the Pentacam (Oculus, Germany) if the appropriate modules are available. It can be argued that EDOF lenses are more forgiving of HOAs.11 In my experience I prefer to avoid EDOFs in irregular corneas as patients can experience a decreased visual quality. Pinhole style lenses, such as the IC-8 lens (Bausch and Lomb, United States) may be useful for treating patients with irregular corneas.12
In our clinic, we assess all patients’ corneal topography for irregularity and we also assess the raw images of the corneal reflections used for biometry. Corneal topography can be significantly impacted by dry eye disease, which is discussed below. It should be repeated until there is consistency across measurements.
Coexisting Ocular Pathology
One of the most important factors in assessing a patient’s suitability for a PC-IOL is a thorough assessment for coexisting pathology. Diffractive lenses split light by design, and a patient with an already compromised visual system can suffer from increased visual side effects and a deterioration in their best corrected visual acuity if implanted with one of these lenses. Real world experience tells us that due to the difference in design between MF IOLs and EDOF IOLs, EDOF lenses may be more forgiving.13 However, this real world experience needs to be further studied in randomised controlled trials before any true recommendations for their use in these patients can be made.
A whole eye examination, including dilated fundus exam and optical coherence tomography (OCT), of the nerve and macula are fundamental to the initial assessment of all patients being considered for any lens procedure undertaken in our clinic. Undiagnosed co-morbidities, such as macular degeneration or glaucoma with field loss, set the patient up for a compromised outcome after surgery and psychological disappointment with their outcome. Specific issues to consider are common pathologies such as:
Glaucoma with field loss: This may not be an absolute contraindication if the patient’s pressures have been well controlled and there is no central field involvement.14
Amblyopia: mildly amblyopic patients may still be candidates for PC-IOLs, however they should be advised that their vision, particularly for near tasks, is better when both eyes are normal.
Monocular patients: These patients were traditionally excluded from PC-IOLs due to the risk of dysphotopsia and compromised visual quality in their only eye, however I have had excellent success with EDOF lenses in only-eyed patients. They are advised of the same caveat as above; their reading vision won’t be as good as with the summative effect of a normal functioning contralateral eye.
Dry eyes: The tear film is one of the most important refractive elements of the eye,15 and dry eye patients with significant corneal staining tend to suffer from more dysphotopsias and impaired visual quality than those with a normal ocular surface.16 Aside from the impact on their vision, their biometry will be impacted if their eyes are dry as will the refractive outcome of their surgery. It is, of course, critical to be spot on with your refractive target in PC-IOL patients, so our protocol is to treat dry eye disease aggressively and bring the patient back for repeat biometry only once their ocular surface is optimised. This can be frustrating for both patient and surgeon alike but is something that I do not compromise on in the interests of achieving the best possible refractive outcome. EDOF lenses may have more of a role in these patients, but in my experience patients with a background of dry eye disease implanted with EDOF lenses can still experience a reduced quality of vision. As an example, Figure 5 is a graph of the unaided Snellen visual acuity of a patient with severe dry eye disease who has a monofocal lens in her right eye (Clareon, Alcon Laboratories, Fort Worth, USA) and an EDOF IOL in her left eye (Alcon Acrysoft Vivity, Alcon Laboratories, Fort Worth, USA). In periods of dry eye exacerbation, her vision became compromised in each eye, however the EDOF eye tended to suffer more in terms of Snellen acuity.

Figure 5. A patient with a monofocal lens in their right eye (red) and EDOF lens in their left eye (green) showing that vision with a monofocal lens tends to be less impacted by dry eye fluctuation than an eye with an EDOF IOL.
Macular disease: Traditionally, macular pathology was a contraindication to presbyopia IOL implantation.17 However, the advent of lenses that do not split light has allowed these patients the opportunity to be implanted with an EDOF lens. After assessing a patient’s OCT and pinhole vision, I estimate how much their macular pathology is likely impacting on their vision and assess whether they are likely to benefit from the use of a PC-IOL. I caution these patients as they may be disappointed with their lack of intermediate or reading vision and I suggest surgeons avoid implanting PC-IOLs in these patients if they are new to PC-IOLs in general. This patient cohort requires thorough counselling and should be given a guarded prognosis, particularly for their intermediate and near vision.
Previous laser refractive surgery: While generally not associated with pathology, previous laser refractive surgery is an important consideration in lens selection. These patients have previously had good unaided vision for all distances, and often expect the same after the lens surgery that they are about to undergo. They are at increased risk of a refractive surprise, which may result in dissatisfaction, and may have aberrated corneas that are not suitable for MF IOLs. They must, therefore, be counselled appropriately around what to expect after their surgery and the real risk of still needing glasses in some, or all circumstances. My current preferred IOL in these patients is a non-diffractive EDOF IOL.
Other Considerations
Pupil size: Pupil size is an important consideration when implanting a PC-IOL. Patients with very large pupils tend to have more dysphotopsias at nighttime, as their pupil significantly dilates, exposing multiple rings of the lens.18 Their reading ability may also be compromised more in dim light as their pupil is not constricting adequately to allow them to look through the central most reading zone of the lens. Likewise, a very small pupil may not allow the patient to fully use all of the zones of the lens, which will limit its multifocality. I tend not to place as much emphasis on the pupil size with EDOF lenses as the optics of the central zone are more forgiving. Significant corectopia or polycoria are absolute contraindications to PC-IOL use.
Pre-operative unaided visual acuity and refractive error: Patients with large refractive errors tend to be some of the happiest patients after any lens or refractive procedure as their baseline unaided vision was so poor. They also tend to be more forgiving of dysphotopsias than those who are close to emmetropia and simply wish to improve their unaided reading vision.
Many of my colleagues have told me they avoid PC-IOLs in the low myope, typically around -2 to -3 dioptres, as replicating their unaided near vision with any lens is difficult. Personally, I do not rule these patients out for a PC-IOL immediately due to their refractive error. Rather, it is important to be upfront with them about what to expect after the surgery. I tell them that in exchange for better distance and intermediate vision, their near vision is unlikely to be as good as it currently is. If they are happy with that trade-off, then we will proceed with a PC-IOL. If they are not willing to sacrifice any near vision, then I will offer them mini-monovision using an EDOF IOL and aim for residual myopia in their non-dominant eye. Even then, I tell them they may still need reading glasses in some circumstances as they are no longer binocularly myopic.
I rarely offer patients true monovision with monofocal IOLs as I think this can lead to issues with depth perception and a potential increase in a patient’s falls risk as they become older and less mobile. It is prudent to keep in mind that the visual set up we choose needs to work not only for today, but for the rest of the patient’s life.
Ocular dominance: All patients are tested to try to determine their ocular dominance. This can be difficult to truly assess, particularly in patients who have asymmetric cataracts and relatively compromised vision in what was previously their dominant eye. There are various techniques to do this. In my practice, we use the hole in a card, telescope, and pointing method for all patients. In patients where this is difficult to ascertain, or if their eye dominance is contralateral to their hand dominance, asking them which eye was dominant can be helpful. For instance, a patient may remember which eye they used to look through the viewfinder in a camera, or may know which eye they used to shoot a gun with.
It is important to check dominance to assist in the refractive target I plan for each eye. I believe that for the patient to feel satisfied with their quality of vision, the dominant eye should always be rendered emmetropic. This is less of an issue when targeting emmetropia in both eyes, such as with an MF IOL, however when I implant EDOF IOLs I will target the first ‘plus’ lens up to 0.16 D and then adjust the non-dominant eye lens to how much I feel the patient values their near vision.
I will usually aim for the first minus lens in that eye if the patient wishes to prioritise distance vision but will increase the amount of residual myopia down to -1 if they want more reading vision. If a patient’s vision is adequate, I like them to have a monovision trial – preferably in a contact lens – to show them what life looks like with that imbalance.
Open disclosure
To ensure patients are happy with their outcome it is essential to be open and upfront with them about what to expect in terms of vision and potential side effects after surgery. If a patient is expecting clear unaided distance and near vision after surgery, implanting an EDOF lens will set them up for disappointment and a feeling of failure postsurgery. While this seems logical and obvious, in my experience most unhappy patients are those who weren’t given the opportunity to discuss their specific visual needs and gain an understanding of the lens choices and trade-offs with their surgeon prior to their lens operation.
Most commonly, dissatisfied PC-IOL patients weren’t advised as to what to expect in terms of spectacle independence or risk of dysphotopsias for their choice of PC-IOL.
My approach is to have a candid discussion with my patients. I explain that there is no perfect solution and all options have a compromise. Ultimately, the choice of PC-IOL comes down to which of those compromises the patient is willing to accept, given their ocular history and visual needs.
I advise my patients that MF IOLs always cause glare and haloes around lights, that this is normal, and part of the way the optics of the lens work. As MF IOLs split light into distinct focal points, this may cause a modest decrease in subjective visual quality, meaning that the patient can expect to see everything without glasses but may find their quality of vision different from past years.
Additionally, I advise them that EDOF IOLs have fewer side effects, but the compromise is less reading vision.
The power of preparing the patient for what to expect cannot be underestimated; fortunately, in my practice I have not had to exchange a single PC-IOL that I have personally implanted.
As with any surgery, it is our patients who are taking the risk; not the surgeon or the optometrist. And ultimately, it is the patients who have to live with their post-operative vision. As such, it is vital that we provide sufficient information about the pros and cons of each type of PC-IOL so that we can help them make the right choice for their individual needs.
Diagnostic and Intraoperative Technology
While not strictly part of the selection criteria, having access to a modern biometer and using the most accurate IOL formulae is integral to success when implanting PC-IOLs. Hitting our refractive target is critical. A high proportion of patients will require a toric IOL. Using an intraoperative digital alignment system for these cases will assist in ensuring accuracy with the refractive outcome in these patients.
CONCLUSION
PC-IOLs are becoming more common in modern ophthalmology as patients’ visual needs shift to include near and intermediate tasks. Patients now expect high levels of spectacle independence after their lens surgery. When we consider all the factors addressed in this article, we realise that for almost all patients, it is now possible to move away from monofocal IOLs and implant PCIOLs. For my practice, doing so has resulted in a higher satisfaction rate among patients and has contributed significantly to the growth of my own practice.
While the selection criteria described in this article may seem arduous, this quickly becomes intuitive, and the process of lens selection and counselling becomes second nature. It is human nature to remain stagnant if what we are doing is not challenged. I believe it is beholden upon eye care professionals to be aware of modern lens choices and help provide patients with the best possible outcome from their surgery.
To earn your CPD hours from this article, visit mieducation.com/presbyopia-correcting-iols shaping-the-future-of-clear-vision.
Dr Armand Borovik MBBS FRANZCO is an ophthalmic surgeon with fellowship training in cataract, cornea, and refractive surgery. He practises in Sydney and Wollongong and holds a staff specialist position at Prince of Wales Hospital, where he teaches cataract and corneal surgery.
 Dr Borovik has published numerous articles in the peer reviewed literature,and lectured widely at international conferences including the American Academy of Ophthalmology and American Society of Cataract and Refractive Surgeons. He has also served as a surgical instructor for courses in corneal surgery and complex ocular surgical techniques. He has a special interest in refractive cataract surgery and decreasing patients dependence on glasses after surgery.
Dr Borovik has published numerous articles in the peer reviewed literature,and lectured widely at international conferences including the American Academy of Ophthalmology and American Society of Cataract and Refractive Surgeons. He has also served as a surgical instructor for courses in corneal surgery and complex ocular surgical techniques. He has a special interest in refractive cataract surgery and decreasing patients dependence on glasses after surgery.
References
- Global patient survey: Patient attitudes to cataracts and cataract surgery. Alcon 2023.
- Kauh, C.Y., Blachley,T.S., Lichter, P.R., et al., Geographic variation in the rate and timing of cataract surgery among US communities. JAMA Ophthalmol 2016;134:267–76.
- Australian Institute of Health and Welfare. Admitted patient care 2017–18. Australian hospital statistics (Cat. no. HSE 225). Canberra: AIHW, 2019.
- Romano, V., Madrid-Costa, D., Alfonso, J.F. et al., Recommendation for presbyopia-correcting intraocular lenses: A Delphi consensus statement by the ESASO study group, American Journal of Ophthalmology, Volume 253, 2023, 169–180.
- Kanclerz, P., Toto, F., Grzybowski, A., et al., Extended depth-of-field intraocular lenses: an update. Asia Pac J Ophthalmol (Phila). 2020; 9(3): 194–202
- de Vries, N.E., Webers, C.A.B., Touwslager, W.R.H., et al., Dissatisfaction after implantation of multifocal intraocular lenses, Journal of Cataract & Refractive Surgery, 37:5, 2011, 859–865.
- Leysen, I., Bartholomeeusen, E., Coeckelbergh, T., Tassignon M.J.B.R., Surgical outcomes of intraocular lens exchange: five-year study J Cataract Refract Surg. 2009 Jun;35(6):1013–8.
- Chang, D.H., Waring, G.O., The subject-fixated coaxially sighted corneal light reflex: a clinical marker for centration of refractive treatments and devices. Am J Ophthalmol 2014 Nov;158(5):863–74. Epub 2014 Aug 12.
- Agarwal, A., Narang, P., Chord mu: a new reference marker and its clinical relevance. Ocular Surgery News. October 10, 2019. Available at: healio.com/news/ophthalmology/20191007/chord-mu-a-new-reference-marker-and-its-clinical-relevance [accessed Feb 2024].
- Sella, R., Shouchane-Blum, K., Reitblat O., et al., ARVO annual meeting abstract, The association between pupil diameter and apparent chord mu length value, June 2022.
- Baartman, B.J., Karpuk, K., Eichhorn, B. et al., Extended depth of focus lens implantation after radial keratotomy. Clin Ophthalmol. 2019; 13: 1401–1408.
- Ang, R.E.T., Araneta, M.M.Q., Cruz, E.M., Review of surgical devices using small aperture optics. Taiwan J Ophthalmol. 2022 Jan 7;12(3):282–294.
- Rementería-Capelo, L.A., Lorente, P., Carrillo, V. et al., Patient satisfaction and visual performance in patients with ocular pathology after bilateral implantation of a new extended depth of focus intraocular lens. J Ophthalmol. 2022 Apr 28;2022.
- Kerr, N.M., Moshegov, S., Lim, S. et al., Visual outcomes, spectacle independence, and patient-reported satisfaction of the Vivity extended range of vision intraocular lens in patients with early glaucoma: an observational comparative study. Clin Ophthalmol. 2023 May 30;17:1515–1523.
15 Sridhar, M.S., Anatomy of cornea and ocular surface. Indian J Ophthalmol. 2018 Feb;66(2):190–194.
16 Pusnik, A., Petrovski, G., Lumi, X., Dysphotopsias or unwanted visual phenomena after cataract surgery. Life (Basel). 2022 Dec 24;13(1):53.
- Grzybowski, A., Kanclerz, P., Tuuminen, R., Multifocal intraocular lenses and retinal diseases. Graefes Arch Clin Exp Ophthalmol. 2020 Apr;258(4):805–813
- Ouchi, M., Shiba, T., Diffractive multifocal intraocular lens implantation in eyes with a small-diameter pupil. 2018 Sci Rep 8.





