
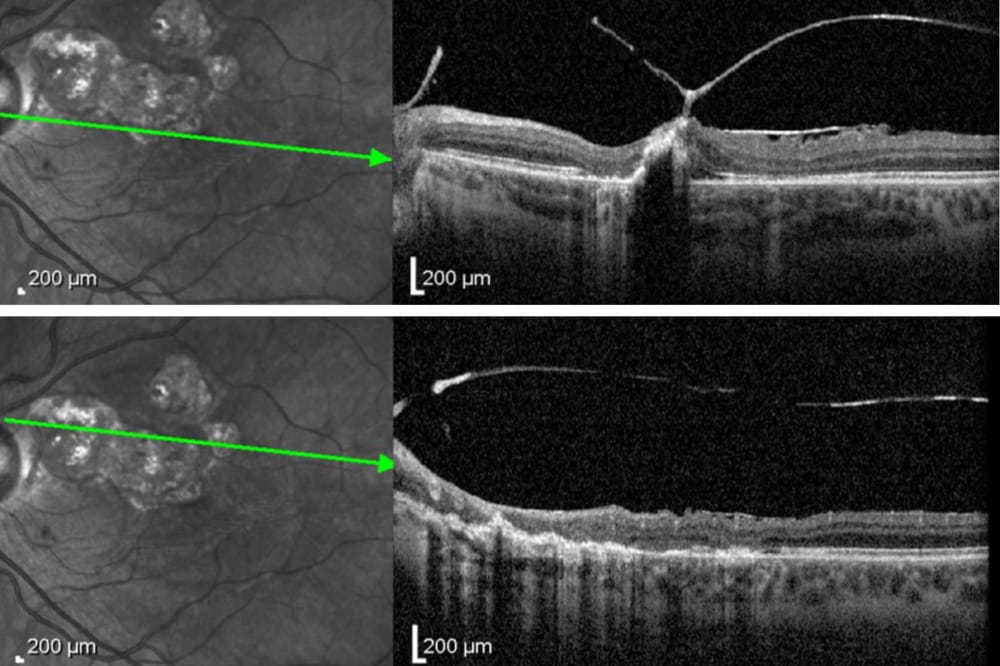
Figure 2. OCT raster scans showing outer retinal atrophy, retinal disorganisation, vitreoretinal adhesion, and an overlying ERM.
Epiretinal membranes (ERMs) are a common finding within optometric practice, with some studies reporting a prevalence of up to 34%.1 While many clinicians may consider an ERM a relatively benign finding, it is important to recognise that they can be associated with a plethora of vision-threatening ocular disorders.2
This article steps through several cases of secondary ERMs reviewed at the Centre for Eye Health. It provides an evidence-based approach to the clinical assessment of ERMs, with particular emphasis on the role of multimodal imaging as a diagnostic tool.
IDIOPATHIC VS SECONDARY ERM
An ERM (also commonly known as macular pucker or cellophane maculopathy) is a growth of fibrocellular tissue at the vitreomacular interface.3 ERMs can be classified as either idiopathic or secondary to ocular diseases, trauma, or retinal surgery.
A number of theories are currently proposed with regards to the cause of idiopathic ERMs. They include the proliferation of glial cells migrating through focal defects in the internal limiting membrane4 or, alternatively, the transformation of hyalocytes on the retinal surface following posterior vitreous detachment. Retinal pigment epithelium (RPE) migration has also been suggested.5,6
On the other hand, secondary ERMs are the result of a coexisting or preceding ocular pathology and make up 32.3% of cases.7 The most frequent causes include previous cataract surgery, and vascular diseases such as diabetic retinopathy and retinal vein occlusions. In particular, proliferative diabetic retinopathy has been shown to be a strong risk factor for secondary ERMs.8 Secondary ERMs are also associated with intraocular inflammation. Approximately 40–50% of cases of intermediate and posterior uveitis develop an ERM.9 Additionally, retinal detachments and tears, ocular trauma, and other retinal surgical procedures can lead to ERM formation.2,10,11 A comprehensive list of secondary causes is outlined in Table 1.
The underlying mechanism involves inflammatory mediators and growth factors, which are responsible for stimulating fibrocellular growth. In addition, retinal pigment epithelial cells migrating through retinal breaks can proliferate on the inner retinal surface, contributing to ERM development.10,12 Compared with idiopathic ERMs, the secondary form has more focal points of adhesion to the retina.13 Secondary ERMs tend to have thicker central macular thickness, poorer presenting visual acuity, worse metamorphopsia, and more optic disc and extramacular involvement.12,13,14 They occur more frequently in younger populations compared with idiopathic ERM patients.12,14
CLINICAL WORKUP OF SECONDARY ERMS
It is not usually clinically possible to detect whether an ERM is idiopathic or secondary from the appearance of the ERM itself. As a result, as well as investigating and documenting the ERM, clinical assessment needs to be targeted to exclude secondary causes.
History and Symptoms
While many patients with ERMs may be asymptomatic,15 those with secondary ERMs are more likely to experience blurred vision, metamorphopsia, micropsia or macropsia, photopsia, diplopia, loss of stereopsis or aniseikonia.2 For this reason, it is important to ask whether the patient is experiencing any difficulties with reading, working, driving or other day-to-day activities. History taking should also elicit for any secondary causes, including flashes or floaters, previous intraocular surgery, uveitis, retinal breaks or trauma.2 Vascular diseases (diabetes, hypertension, hyperlipidaemia) can be associated with ERMs secondary to central or branch vein occlusions, so including these in history taking is also prudent.
Entrance Tests
Visual acuity and monocular Amsler grid testing should be performed to evaluate for vision reduction and metamorphopsia. Amsler grid testing results should be interpreted with caution however, as the Amsler grid relies heavily on subjective interpretation and has poor sensitivity in the early detection of metamorphopsia.16 Less commonly, other functional tests such as contrast sensitivity charts, microperimetry, M-charts for metamorphopsia, and aniseikonia test charts, may also be used to document subjective vision changes.17
Slit Lamp Examination
A thorough examination of the anterior eye is necessary to identify secondary causes of an ERM. Signs of current uveitis may include anterior chamber cells and/or flare, hypopyon, keratic precipitates or inflammatory cells within the vitreous. Posterior synechiae, pigmented keratic precipitates or rubeosis iridis may suggest a chronic or prior event.18 Previous ocular trauma may manifest as corneal scars, traumatic mydriasis or miosis, corectopia, iris stromal tears, angle recession on gonioscopy, cataracts or lens subluxation.19
Posterior Eye Examination
A dilated fundus examination should be performed on all patients with ERMs,2,3 particularly if they are a new patient or if the ERM is a new finding. As well as assessing and documenting the characteristics of the ERM itself, it is important to screen for any peripheral retinal breaks, signs of posterior uveitis or previous intraocular surgery, such as laser retinopexy or panretinal photocoagulation therapy. Retinal haemorrhages or evidence of ischemia may be indicative of diabetic retinopathy or vascular occlusions. Advanced ERMs can be associated with small retinal haemorrhages, cystoid macular oedema and lamellar or full thickness macular holes.2,3
Multimodal Imaging
Multimodal imaging is a key component in both the analysis of ERMs themselves as well as enhancing the detection of secondary causes.
- Optical coherence tomography (OCT) is the most useful imaging modality for assessing the structural features of ERMs as well as for assessing whether vitreomacular traction is implicated as the underlying cause.20 ERMs appear as a hyper-reflective layer on the internal limiting membrane and can be associated with underlying retinal wrinkling and loss of the foveal pit.
ERMs may also result in cystoid spaces, foveoschisis, macular holes, disorganisation of the retinal layers, and disruption to the ellipsoid zone or interdigitation zone.2 When vitreomacular disease or any of these features are present, a combination of horizontal raster scans and radial scans is likely to be beneficial to maximise detection and monitoring of these associated signs.
- Ultra-widefield retinal imaging can be used to supplement a dilated fundus examination to document any vascular or peripheral retinal lesions likely to be linked to secondary causes of ERMs. Posterior pole, and in particular widefield autofluorescence, can also be used to help exclude retinal dystrophies that may be associated with ERMs.
- OCT-angiography (OCT-A) can assist with further information on the extent of vascular diseases associated with ERMs. Furthermore, OCT-A may reveal alterations in the foveal avascular zone21 and changes to the tortuosity of retinal vessels,22 especially in advanced stages.
CONCLUSION
A thorough clinical examination and dilated fundus examination is integral for differentiating between idiopathic and secondary ERMs. Multimodal imaging is particularly useful in the detection of secondary causes of ERMs and should be included as appropriate to assist the comprehensive work up.
For further reading, we recommend referring to Fung et al., in Clinical and Experimental Ophthalmology for a comprehensive review of ERMs.2
CASE EXAMPLES
Case 1: ERM Secondary To Posterior Uveitis
A 38-year-old Caucasian female (Mrs Apple*) was referred to the Centre for Eye Health for further investigation and documentation of a toxoplasmosis scar in the left eye. Mrs Apple had been diagnosed as having toxoplasmosis in her left eye in 2005 and had an injection in the eye at the time of diagnosis. She noted difficulties with night driving and fluctuating reading vision. She denied any flashes or floaters, or past history of uveitis, retinal breaks or trauma. Medical history was unremarkable.
Best-corrected visual acuities were RE 6/4.8 and LE 6/24+2 (which did not improve on pinhole). Amsler grid results were clear in the right eye, with metamorphopsia centrally in the left eye.
Anterior ocular examination was unremarkable. Posterior pole examination was unremarkable in the right eye, however, there were multiple areas of chorioretinal atrophy and associated RPE hyperplasia at the left macula, consistent with scarring from toxoplasmosis (Figure 1). Cirrus OCT through the area revealed outer retinal atrophy inferior to the lesion, vitreoretinal adhesion, and an overlying ERM (Figure 2). The peripheral retina was unremarkable in both eyes (Figure 3).

Figure 1. Coloured and red-free fundus images showing multiple areas of toxoplasmosis scarring

Figure 3. Ultra-widefield retinal imaging showing a clear periphery and fundus autofluorescence, revealing hypoautofluorescent lesions with surrounding hyperautofluorescence at the left macula.
Case 2: ERM Secondary to Treated Retinal Detachment
A 60-year-old Asian male (Mr Barry*) was referred to the Centre for Eye Health for further investigation and documentation of an ERM in the right eye. Mr Barry noted occasional floaters in each eye, but no significant visual concerns. He had experienced a previous retinal tear and detachment in the right eye, which had been lasered two years ago. He denied any flashes, or history of uveitis or trauma. His medical history was unremarkable.
Mr Barry’s best-corrected visual acuities were RE 6/4.8 and LE 6/6+2. Amsler grid results revealed metamorphopsia centrally in the right eye, but clear in the left eye.
Anterior ocular examination was unremarkable apart from age-appropriate cataracts in each eye. Posterior ocular examination showed a semitranslucent, grey-white membrane with superficial retinal folds over the foveal and parafoveal area of the right eye (Figure 4). Dilated fundus examination revealed extensive laser retinopexy surrounding lattice degeneration in the superior periphery of the right eye. There was also an area of laser retinopexy surrounding a horseshoe tear and associated retinal detachment in the temporal periphery (Figure 5). The left fundus was unremarkable.

Figure 4. Coloured and red-free fundus images showing an ERM at the right macula.

Figure 5. Ultra-widefield retinal imaging revealing lattice degeneration and laser retinopexy in the superior periphery. There was a horseshoe tear with associated retinal detachment and surrounding laser retinopexy in the temporal periphery.
Cirrus OCT scans showed an ERM with associated foveoschisis at the right macula (Figure 6). The right eye peripheral findings were confirmed via OCT line scans (Figure 7).

Figure 6. OCT raster and radial scans confirming an ERM with associated foveoschisis.

Figure 7. Peripheral OCT line scans through the horseshoe tear and retinal detachment.
*Patient names changed for anonymity.
The author acknowledges Michael Yapp and Michele Clewett who reviewed and contributed to this article.
Tania Lu BSc MClinOptom completed her Bachelor of Vision Science and Master of Clinical Optometry from The University of New South Wales. She works in both corporate optometric practice and as a staff optometrist at the Centre for Eye Health. She has an interest in treating posterior ocular diseases and reducing preventable blindness in the community.
*Patient names changed for anonymity.
The author acknowledges Michael Yapp and Michele Clewett who reviewed and contributed to this article.
Tania Lu BSc MClinOptom completed her Bachelor of Vision Science and Master of Clinical Optometry from The University of New South Wales. She works in both corporate optometric practice and as a staff optometrist at the Centre for Eye Health. She has an interest in treating posterior ocular diseases and reducing preventable blindness in the community.
References
- Meuer, S.M., Myers, C.E., Klein, B.E., et al., The epidemiology of vitreoretinal interface abnormalities as detected by spectraldomain optical coherence tomography: The Beaver Dam Eye Study. Ophthalmology. 2015;122(4):787–795.
- Fung, A.T., Galvin, J., Tran, T., Epiretinal membrane: A review. Clinical and Experimental Ophthalmology. 2021 Apr;49(3):289–308.
- Ożóg, M.K., Nowak-Wąs, M., Rokicki ,W., Pathophysiology and clinical aspects of epiretinal membrane–review. Frontiers in Medicine. 2023;10.
- Vieira, L., Reina, M., Medeiros, M.D., et al., Secondary epiretinal membrane after trabeculectomy. Journal of Glaucoma. 2016 Jun 1;25(6):e576–80.
- Smiddy, W.E., Maguire, A.M., Green, W.R., et al., Idiopathic epiretinal membranes. Ultrastructural characteristics and clinicopathologic correlation. Ophthalmology. 1989; 96(6): 811–820.
- Sebag, J., The vitreoretinal interface and its role in the pathogenesis of vitreomaculopathies. Ophthalmologe. 2015; 112(1): 10–19.
- Kawasaki, R., Wang, J.J., Mitchell, P., et al., Racial difference in the prevalence of epiretinal membrane between Caucasians and Asians. Br J Ophthalmol. 2008; 92(10): 1320–1324.
- Cheung, N., Cheng, C.Y., Wong, T.Y., et al., Prevalence and risk factors for epiretinal membrane: the Singapore Epidemiology of Eye Disease study. British Journal of Ophthalmology. 2017 Mar 1;101(3):371–6.
- Yap, A., Welch, S., Niederer, R.L., et al., Epiretinal membrane in uveitis: Rate, visual prognosis, complications and surgical outcomes. Clinical and Experimental Ophthalmology. 2024 Jan;52(1):54–62.
- Perente, I., Özçalişkan, Ş., Karasu, B., et al., Secondary epiretinal membrane following rhegmatogenous retinal detachment. Photodiagnosis and Photodynamic Therapy. 2020 Sep 1;31:101833.
- Tsotridou, E., Zachariadis, Z., Anogeianakis, G., et al., A review of last decade developments on epiretinal membrane pathogenesis. Medical Hypothesis, Discovery and Innovation in Ophthalmology. 2020;9(2):91.
- Lee, G.W., Kim, S.J., Kang, S.W., et al., Characteristics of secondary epiretinal membrane due to peripheral break. Scientific Reports. 2020 Nov 30;10(1):20881.
- Mori, K., Deguchi, T., Yoneya, S., et al., Comparison of epiretinal membranes of differing pathogenesis using optical coherence tomography. Retina. 2004 Feb 1;24(1):57–62.
- Yazici, A.T., Çekiç, O., Yilmaz, Ö.F., et al., Idiopathic and secondary epiretinal membranes: do they differ in terms of morphology? An optical coherence tomography–based study. Retina. 2011 Apr 1;31(4):779–84.
- Kanukollu, V.M., Agarwal, P., Epiretinal membrane. InStatPearls [Internet] 2023 Jul 24. StatPearls Publishing.
- Midena, E., Vujosevic, S., Metamorphopsia: an overlooked visual symptom. Ophthalmic research. 2015 Nov 11;55(1):26–36.
- Tanikawa, A., Shimada, Y., Horiguchi, M., Comparison of visual acuity, metamorphopsia, and aniseikonia in patients with an idiopathic epiretinal membrane. Japanese Journal of Ophthalmology. 2018 May;62:280–5.
- Harthan, J.S., Opitz, D.L., Fromstein, S.R., Morettin, C.E., Diagnosis and treatment of anterior uveitis: optometric management. Clinical Optometry. 2016 Mar 31:23–35.
- Vidne-Hay, O., Fogel Levin, M., Moisseiev E., et al., Blunt ocular trauma in patients over 70: clinical characteristics and prognosis. European Journal of Ophthalmology. 2021 Sep;31(5):2705–9.
- Do, D.V., Cho, M., Haller J.A., et al., The impact of optical coherence tomography on surgical decision making in epiretinal membrane and vitreomacular traction. Transactions of the American Ophthalmological Society. 2006 Dec;104:161.
- Mao, J., Lao, J., Shen L., et al., A study analyzing macular microvasculature features after vitrectomy using OCT angiography in patients with idiopathic macular epiretinal membrane. BMC Ophthalmology. 2020 Dec;20(1):1–8.
- Hsia Y., Hsieh Y.T., Associations between macular retinal vasculature and severity of idiopathic epiretinal membrane. BMC Ophthalmology. 2023 May 5;23(1):200





