

Gonzalo Jacome
Our knowledge of diabetes has expanded in recent years. But what do we need to consider when managing the eye health of people with diabetes? Dr Margaret Lam spoke to Gonzalo Jacome from Centre for Eye Health Australia (CFEH) to find out.
Q. In the context of recent learnings, what is important for eye care professionals to understand about managing diabetic retinopathy?
For eye care practitioners looking after patients with diabetes mellitus (DM), it’s essential to have a clear grasp of the risk factors associated with diabetic eye disease. A good understanding of these factors will ensure patients are counselled accordingly, and that communication with their general practitioner, and / or endocrinologist, is targeted to optimise modifiable systemic risk factors that can help preserve vision.
According to a recent Cochrane review,1 elevated Hba1c is the most significant risk factor with regards to both incidence and progression of diabetic retinopathy in patients with type 1 and 2 diabetes. The risk of incidence of diabetic retinopathy also increases, the longer a patient has been diagnosed with type 1 or 2 DM.
Other notable risk factors include suboptimal control of hypertension (specifically for type 2), kidney disease (high protein level in the urine), and current pregnancy (due to the increased fluctuations in Hba1c). Ethnicity is an independent risk factor for people with type 2 diabetes in population groups such as African Americans, Hispanics, South Asians, and Aboriginal and Torres Strait Island peoples.
Age at diagnosis of DM is also a risk factor. People diagnosed with type 1 diabetes before the age of 12 are more likely to develop diabetic retinopathy; and in type 2, the older a person is at diagnosis, the greater the risk for proliferative diabetic retinopathy (PDR).
Q. Are there any notable changes to the way we grade retinopathy and macular oedema?
Most clinicians grade retinopathy according to the International Clinical Diabetic Retinopathy and Diabetic Macular Edema Disease Severity Scales.2 In recent times, several optical coherence tomography (OCT) grading scales have also been proposed for diabetic macula oedema (DMO).3,4 While there is no ‘new or notable learning’ in this space, what we need to emphasise is that grading retinopathy correctly is important because it helps to stratify risk for developing advanced disease, sets recall periods, and promotes timely referral for treatment when required. For example, according to the Early Treatment Diabetic Retinopathy Study (ETDRS) on ‘Progression to high-risk PDR’,5 even patients diagnosed with mild DR can have up to 20% chance of ending up with PDR at seven years. That number increases with higher gradings of retinopathy; rising to a 45% chance in moderateto- severe non-proliferative PDR (NPDR) cases.
This is incredibly relevant to optometry, given that most cases we see in practice have NPDR.
Q. Should we be including peripheral retinopathy when grading DR?
Given that the grading system commonly used is based on the ETDRS seven standard fields (7SF), which measures about 30% of the entire retina, invariably we will find retinopathy beyond these boundaries and sometimes with minimal or no 7SF involvement.
In a recent review of the literature undertaken by the vascular department at the Centre for Eye Health, some studies found peripheral haemorrhages in up to 40% of patients/eyes, outside the 7SF. Neovascularisation was found outside the 7SF in a significant number of cases as well. In patients with DR, the most common peripheral quadrant where retinopathy was identified was temporal, followed by superior, inferior, and nasal. Intraretinal haemorrhages were observed to occur in areas of capillary nonperfusion, and at the boundaries of perfused and non-perfused zones. These lesions may play a role as a prognostic marker for DR worsening.6,7
This reminds us about the importance of looking outside the posterior poles to assess and grade DR correctly and triage management. Patients with notable peripheral retinopathy, even with minimal or no central retinopathy, should be monitored closely.
Q. Is there any link between DR and cardiovascular disease risk?
Another recent learning revolves around cardiovascular health. It has long been considered that the presence and level of DR represents a marker for cardiovascular risk. A recent paper8 confirmed that the presence of DR in type 2 diabetes is significantly associated with future risk of cerebrovascular accidents, myocardial infarctions, congestive heart failure, and even death. Furthermore, more severe DR posed greater risk for each outcome.
Clinicians should, therefore, recognise that DR presence and severity may be considered as a marker for future risk of systemic complications. Practically, this reinforces the importance of holistic and personalised multidisciplinary management of disease risk with two-way communication between optometrists, general practitioners, endocrinologists, and other members of the diabetes care team.
Q. How do you use fenofibrate in the management of DR?
The available research on fenofibrate suggests that it slows the progression of DR and reduces the need for laser pan retinal photocoagulation (PRP) and vitrectomy surgery in type 2 diabetes.9,10 However, there is no clear protocol on how to use it. For example, do we recommend it to everyone who has moderate NPDR, or should we wait to see if they are progressing?
In practice, I normally refer patients to their physician to see if they are suitable and check for any contraindications. This is normally done after a few follow-up visits where the moderate NPDR appears to be somewhat progressing or is just recalcitrant, particularly in situations where they already have poor lipid metabolism. However, I always start by reinforcing the importance of optimal glycemic control rather than believing fenofibrate is a silver bullet.
Q. What do you see as important advances in diabetic management for the eye care space?
The rise in the use of glucagon-like peptide 1 (GLP-1) receptor agonists, such as Ozempic, has been a game changer for many people managing type 2 diabetes. This is due to its ability to lower Hba1c in patients and reduce the risk of cardiovascular events in those with type 2 diabetes and cardiovascular disease. A recent meta-analysis11 of 25 papers showed an increased risk in the occurrence of DR-related events in people older than 60 years and with DM for more than 10 years; this is thought to be due to rapid lowering of the blood glucose having a rebound ischaemic effect on the retina. There was no significant difference in patients under 60 or with DM less than 10 years. However, it should be noted that studies were restricted to short follow-up periods and long-term benefits or risks to the eye are not known.
Q. How should we manage DMO in the context of good visual acuity?
Traditionally, patients with DMO were expected to be referred to an ophthalmologist regardless of the level of visual acuity (VA). There was no data on what to do with patients who maintained good VA and whether they would benefit from laser or anti-VEGF.
At the CFEH, we have embraced the recent research from the DRCR.net group, named Protocol V,12 which concluded that close observation of these patients, while concurrently ensuring good control of systemic risk factors for DR, was reasonable as the majority retain good VA at 24 months.
Another study13 found similar findings at 12 months. They also identified which OCT biomarkers may predict VA loss in the observation group and would benefit from earlier referral for therapy.14
These included hyper-reflective foci (HRF), disorganisation of the retinal inner layers (DRIL), and ellipsoid zone disruption (EZ) (Figure 1).
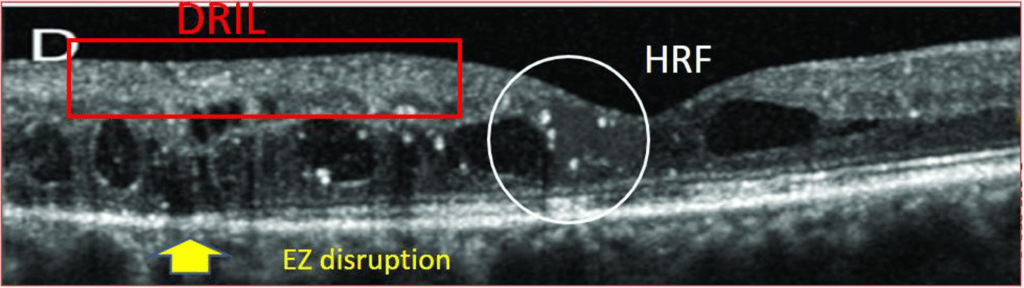
Figure 1. An example of OCT predictive biomarkers.
Q. In conclusion, how would you recommend interested optometrists proceed with managing patients who have diabetes?
As always, I would encourage clinicians to work within the scope of optometry they are competent with. Should they review these patients themselves, follow a clear protocol, including clear communication with the patient’s general practitioner and / or endocrinologist, and refer on to a medical retina ophthalmologist as soon as treatment is indicated.

Dr Margaret Lam
Dr Margaret Lam BOptom UNSW Post Grad OcTherapy is the National President of Optometry Australia. She practises optometry at 1001 Optical in Bondi Junction in Sydney and teaches at the School of Optometry at The University of New South Wales as an Adjunct Senior Lecturer.
Gonzalo Jacome received his Bachelor of Optometry and Graduate Certificate in Ocular Therapeutics from the UNSW. He has worked in full scope private practice since 1992 and is a Senior Staff Optometrist at the Centre for Eye Health Australia. He has particular interests in dry eye management, diabetic eye disease, glaucoma and contact lenses. His interest also extends to public health with specific concern for improving accessibility to the latest diagnostic ocular imaging and treatment services for the general community. He believes in a mentoring model inspiring junior optometrists to keep developing their clinical expertise.
References
- Perais, J., Agarwal, R., Lois, N., et al., Prognostic factors for the development and progression of proliferative diabetic retinopathy in people with diabetic retinopathy. Cochrane Database Syst Rev. 2023 Feb 22;2(2):CD013775. DOI: 10.1002/14651858.CD013775.pub2.
- Wilkinson, C.P., Ferris, F.L. 3rd, Verdaguer, J.T, Global Diabetic Retinopathy Project Group. Proposed international clinical diabetic retinopathy and diabetic macular edema disease severity scales. Ophthalmology. 2003 Sep;110(9):1677-82. DOI: 10.1016/S0161-6420(03)00475-5.
- Hui V.W.K., Szeto S.K.H., Cheung C.Y., et al., Optical coherence tomography classification systems for diabetic macular edema and their associations with visual outcome and treatment responses – An updated review. Asia Pac J Ophthalmol (Phila). 2022 Jun 1;11(3):247-257. DOI: 10.1097/APO.0000000000000468. PMID: 34923521.
- Panozzo, G., Cicinelli, M.V., Augustin, A.J., et al., An optical coherence tomography-based grading of diabetic maculopathy proposed by an international expert panel: The European School for Advanced Studies in Ophthalmology classification. European Journal of Ophthalmology. 2020;30(1):8–18. DOI:10.1177/1120672119880394.
- Davis, M.D., Fisher, M.R., Knatterud, G.L.. Risk factors for high-risk proliferative diabetic retinopathy and severe visual loss: Early Treatment Diabetic Retinopathy Study Report #18. Invest Ophthalmol Vis Sci. 1998 Feb;39(2):233–52. PMID: 9477980.
- Marcus D.M., Silva P.S., Sun J.K., et al., DRCR Retina Network. Association of predominantly peripheral lesions on ultra-widefield imaging and the risk of diabetic retinopathy worsening over time. JAMA Ophthalmol. 2022 Oct 1;140(10):946–954. DOI: 10.1001/jamaophthalmol.2022.3131. Erratum in: JAMA Ophthalmol. 2023 Jan 1;141(1):104. PMID: 35980608; PMCID: PMC9389433.
- Silva, P.S., Cavallerano, J.D., Aiello, L.P., Peripheral lesions identified on ultrawide field imaging predict increased risk of diabetic retinopathy progression over 4 years. Ophthalmology. 2015 May;122(5):949–56. DOI i: 10.1016/j.ophtha.2015.01.008. Epub 2015 Feb 19. PMID: 25704318.
- Modjtahedi, B.S., Wu, J., Chen, W., Severity of diabetic retinopathy and the risk of future cerebrovascular disease, cardiovascular disease, and all-cause mortality. Ophthalmology. 2021 Aug;128(8):1169–1179. DOI: 10.1016/j.ophtha.2020.12.019.
- Keech, A.C., Mitchell, P., Colman, P.G., et al., FIELD study investigators. Effect of fenofibrate on the need for laser treatment for diabetic retinopathy (FIELD study): A randomised controlled trial. Lancet. 2007 Nov 17;370(9600):1687–97. DOI: 10.1016/S0140-6736(07)61607-9.
- ACCORD Study Group; ACCORD Eye Study Group; Chew, E.Y., Ambrosius, W.T., Fine, L.J., Effects of medical therapies on retinopathy progression in type 2 diabetes. N Engl J Med. 2010 Jul 15;363(3):233–44. DOI: 10.1056/NEJMoa1001288. Epub 2010 Jun 29. Erratum in: N Engl J Med. 2011 Jan 13;364(2):190. Erratum in: N Engl J Med. 2012 Dec 20;367(25):2458.
- Wang, F., Mao Y., Wang, H., Liu, Y., Huang P., Semaglutide and Diabetic Retinopathy Risk in Patients with Type 2 Diabetes Mellitus: A Meta-Analysis of Randomized Controlled Trials. Clin Drug Investig. 2022 Jan;42(1):17-28. DOI: 10.1007/s40261-021-01110-w. Epub 2021 Dec 11. PMID: 34894326.
- Baker, C.W., Glassman, A.R., Sun, J.K., DRCR Retina Network. Effect of initial management with aflibercept vs laser photocoagulation vs observation on vision loss among patients with diabetic macular edema involving the center of the macula and good visual acuity: A randomized clinical trial. JAMA. 2019 May 21;321(19):1880–1894. DOI: 10.1001/jama.2019.5790.
- Busch, C., Fraser-Bell S., Rehak M., et al., International Retina Group. Real-world outcomes of observation and treatment in diabetic macular edema with very good visual acuity: the OBTAIN study. Acta Diabetol. 2019 Jul;56(7):777–784. DOI: 10.1007/s00592-019-01310-z.
- Busch, C., Okada, M., Rehak M., et al., International Retina Group. Baseline predictors for visual acuity loss during observation in diabetic macular oedema with good baseline visual acuity. Acta Ophthalmol. 2020 Nov;98(7):e801-e806. DOI: 10.1111/aos.14390. Epub 2020 Mar 1.
CASE STUDY
A 54-year-old male was referred to the Centre for Eye Health. He reported:
- No current or recent vision concerns,
- Type 2 diabetes diagnosed in 2016, with the most recent HbA1c reading of 7.6%
(previously 11%),
- He was on treatment for systemic hypertension.
- BCVA R 6/6 L 6/4.8,
On his first visit in 2023, the patient was diagnosed with bilateral moderate NPDR and centre involving diabetic retinopathy (CIDMO) in his right eye. Since then, he has been reviewed at regular intervals with no evidence of progression to the CIDMO, with only hyper-reflective foci as a potential biomarker for progression.
The OCT line scans clearly show persistent CIDMO in the right eye with hyperreflective foci and the maintenance of good visual acuity.
His management included optimisation of blood glucose levels, blood pressure, and cholesterol with the help of his GP as well as weight loss.
He attends regular reviews at CFEH where a very good recall program means that he is followed up if he fails to attend.





