

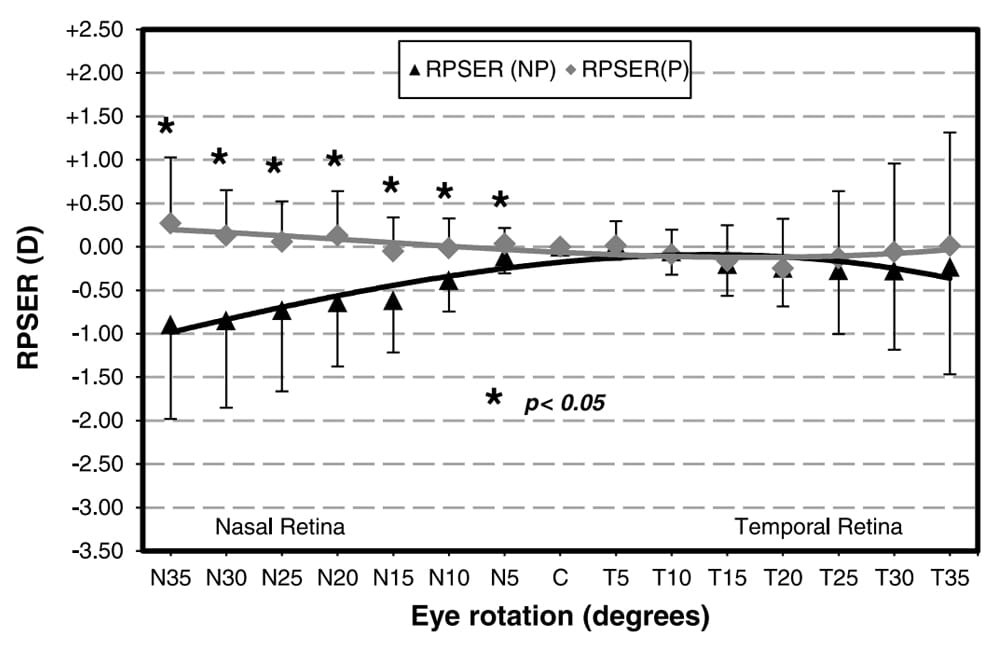
Figure1. Difference in relative peripheral spherical equivalent refraction (RPSER) between non-progressing and progressing myopes.
The increasing prevalence of myopia and its significant impact on vision and eye health has prompted global researchers to investigate strategies for its management, including specially designed myopia management spectacle lenses.
CR Labs’ Dr Fiona Om provides this deep dive into MyoMe and MyoStock, two innovative products that not only address the broader issue of myopia but also cater to specific demographics within the population.
In recent years, the alarming rise of myopia among children has become a subject of growing concern, particularly when left undiagnosed and when management is delayed. The Brien Holden Vision Institute predicts that by 2050, approximately five billion individuals will be diagnosed with myopia, with one in five developing severe myopia.1 People with severe myopia have a higher risk of developing sight-threatening conditions including myopic maculopathy, retinal detachment, glaucoma, and cataract.2
Consequently, myopia is predicted to be one of the main contributors to irreversible blindness in the world.
The rise in myopia prevalence, along with its profound negative impact on vision and eye health, has sparked considerable interest and motivation among eye care practitioners to integrate myopia management strategies into their standard practices.
Studies have reported that reducing the progression of myopia by one dioptre (D) during childhood can potentially lead to a 40% reduction in developing sight-threatening conditions such as myopic maculopathy.3
PERIPHERAL DEFOCUS THEORY
It has been hypothesised that peripheral hyperopic defocus plays a role in myopia progression.4 Before the introduction of myopia management spectacles, conventional negative lenses were prescribed. Standard negative lenses worked by shifting images onto the retinal plane, precisely at the fovea, to ensure clear and sharp vision. Subsequently, the images formed in the periphery fell behind the retinal plane, providing a stimulus for axial length elongation, known as peripheral hyperopic defocus.
As the retina is asymmetrical, there is a difference in anatomical neural characteristics,5 peripheral hyperopic defocus, and peripheral refraction4 between the nasal and temporal retinal hemifields. It has been suggested that the nasal retina is more involved in driving eye growth in the presence of hyperopic defocus.6
Faria-Riberio et al. investigated the difference in relative peripheral refraction between progressing (P) and non-progressing (NP) young adults with myopia.6 The authors reported the P group had a statistically significant amount of peripheral hyperopia in the nasal hemifield, compared to the NP group (p<0.002) (Figure 1). Additionally, the overall retinal contour in the nasal quadrant among the P group was steeper than the NP group (p-0.001).
Therefore, it has been proposed that peripheral hyperopic defocus acts as a stimulus to promote axial length elongation, and that this should be considered when designing lenses to reduce myopia progression.
MYOME
Design Characteristics
MyoMe was designed to consider the morphological characteristics of the myopic retina. It is made up of a central viewing zone that fully corrects refractive error at the fovea, providing clear and sharp vision (Figure 2). The central viewing zone is an oval shape, measuring 7 mm horizontally, and extending vertically towards the upper portion of the lens.

Figure 2. MyoMe seamlessly incorporates the central viewing zone, nasal and temporal peripheral treatment zones, and reading addition.
The central correction area is surrounded by a progressive power distribution. Myopic defocus is induced by distributing positive power in the peripheral lens. In particular, the nasal and temporal areas of the lens are assigned asymmetric additions to compensate for retinal asymmetry. The nasal area of the lens has an addition value of +1.50 dioptre sphere (DS) at 25 mm, providing a moderate level of defocus in the temporal retina. The temporal area of the lens has an addition value of +1.80DS at 25 mm, providing a slightly higher level of defocus in the nasal retina. The inferior area of the lens has an addition value of +2.00DS, delivering a large useable area at the lower part of the lens for near-work tasks.
Research studies in myopic children7,8 have found an association between high accommodative convergence/accommodation (AC/A) ratios and myopia. A high AC/A ratio is associated with common binocular vision disorders such as accommodative lags.
Due to the association between binocular vision disorders and myopia, studies have investigated the effectiveness of bifocal9 or progressive addition lenses10 in slowing myopia progression among children. These studies have reported a slight but significant effect. Hence, an alternative solution is required to address binocular vision issues like accommodative lags and spasms while slowing down myopia progression. MyoMe uses Myo-Freeform technology to seamlessly incorporate the central viewing zone with the peripheral treatment zones and near add, to form a lens that provides better comfort and maximises user compliance with treatment.
Benefits of Myo-Freeform Technology
One of the advantages of this design is that the astigmatism distribution induced by the progressive power variation is minimal. The critical regions for distance and near vision are primarily freeform astigmatism. The astigmatism distribution peaks are located laterally, which helps to increase blur in the lateral peripheral retina.
Another advantage of this design is that the smooth progressive power distribution creates a natural and aesthetically pleasing lens, with no obvious patterns or imprints. Due to the positive power increments in the peripheral area, MyoMe is thinner than the standard negative lens, contributing to its appealing cosmetic appearance.
Lastly, it is available in a wide range of materials and coatings. These features combine to provide an ideal balance between the central correction area and treatment zone, thereby enhancing comfort and promoting friendly useability while maintaining optimal treatment efficacy.
MyoMe Clinical Trial
A MyoMe clinical trial examined the efficacy of MyoMe in mitigating myopia progression in European children, in comparison to a control group wearing single-vision lenses (SVL).11 The study involved 83 myopic children aged five to 12 with a prescription of -0.50D and above, astigmatism, and anisometropia under 1.50D, with best corrected visual acuity of 6/6. The participants were randomly assigned to either the study group (MyoMe) or the control group (SVL). Myopia progression was monitored by measuring axial length (AL) growth over a year.
Following 12 months of treatment, the study group exhibited reduced AL elongation compared to the control group (0.16 ± 0.16 mm vs 0.24 ± 0.16 mm, p=0.034). MyoMe significantly decreased absolute AL growth by 39% (p=0.014) over 12 months compared to the control group.11
MYOSTOCK
Addressing the Rising Cost of Living
Many Australian families are currently affected by the rising cost of living. In the 12 months prior to March 2024, the ‘living cost index’ increased up to 6.5%.12 Research surveys conducted by the Salvation Army revealed that 94% of respondents found it challenging to afford household essentials, medical expenses, and utilities.13
Studies have reported that as healthcare costs rise, individuals may forgo fundamental healthcare services.14 Consequently, delayed health care increases the risk of health complications,15 affecting not only the individual and family members but also straining the healthcare system and contributing to its cost.
For many families, the expense of myopia management lenses poses a significant hurdle. The costs associated with the production and supply of myopia management lenses are significantly higher compared to conventional single vision correction lenses. According to the April–June 2024 edition of the Optical Distributors and Manufacturers Association’s EyeTalk Reference Guide, a set of myopia management lenses can cost an individual up to AU$818. Although early adoption of myopia management strategies can mitigate future health risks and financial burdens associated with severe myopia, the initial investment is deemed to be a barrier for some individuals.
In response to the rising cost of living and the challenges posed by the current myopia landscape, a more affordable solution called MyoStock has been developed and introduced into the market.
Design Characteristics
MyoStock is a new and emerging myopia management lens disrupting the optical industry. It features distinctive hexagon-implicated defocus segments (HIDS) technology to address near-sightedness, while slowing down the progression of myopia.
The lens is made of a central viewing zone with a width of 12.4 mm to ensure ease of adaptability and to provide clear and comfortable vision.
Surrounding the central viewing zone are hundreds of micro-hexagonal segments, which promote myopic defocus in the peripheral retina (Figures 3 and 4). In particular, the defocus power surrounding the central viewing zone is +3.50DS, and towards the peripheral lens is +4.50DS. The defocus power is higher in the peripheral regions of the lens to compensate for the refraction changes in the peripheral retina. The uniform arrangement of the micro-hexagonal segments promotes continual myopic defocus.

Figure 3. MyoStock features a central viewing zone and micro-hexagonal segments with HIDS technology.

Figure 4. MyoStock’s HIDS technology.
Therefore, the main features of MyoStock include its central viewing zone and defocus segments with HIDS technology, offering comfortable vision, while slowing down axial length elongation and reducing the risk of myopia progression.
Benefits of HIDS Technology and Results
MyoStock was developed based on the principles of simultaneous defocus, allowing for objects to be comfortably viewed at both distance and near. The central viewing zone ensures one plane sharply focusses on the retina and provides clear vision. The defocus segments with HIDS technology results in another plane to focus in front of the retina, promoting myopic defocus.
As well as its exceptional design, the lens comes in a 1.6 high index material and automatically comes with a blue filter and an ‘Ultra Super Hydrophobic’ multicoat.
An unpublished study was conducted to investigate the effect of MyoStock on myopia progression. The study involved 150 children of Chinese ethnicity between the ages of eight to 15 years with a prescription of -1.00DS to -6.00DS and less than -1.50 dioptre cylinder (DC). In the experiment, half the participants were prescribed conventional single vision distance lenses; the other half were prescribed MyoStock and were asked to wear the lenses full time. The study lasted 18 months and at the end of the experiment, the rate of myopia progression in the cohort wearing MyoStock lenses had decreased by 45% and the rate of axial length elongation had decreased by 53%.
Even though the research has not been formally published, the HIDS technology was developed based on well-established principles and reports promising results in managing myopia progression.
CONCLUSION
MyoMe and MyoStock represent two distinct lenses, each adopting unique technologies to address the pressing issue of myopia while catering to specific demographics.
MyoMe takes into consideration retinal asymmetry and accordingly, incorporates this information into its peripheral treatment zones. It features a near add, which is beneficial for patients with accommodative issues, potentially contributing to their myopic progression. MyoMe is available in a broad range of prescriptions, materials, and coatings.
On the other hand, MyoStock is one of the most cost-effective myopia management lenses, reducing the barriers of cost for families struggling with the cost of living. It uses HIDS technology to slow down myopia progression and comes in a tougher, thinner, lighter material with a blue filter and easy-to-clean multicoat.
Both lenses share a unique place in the realm of myopia management lenses, aiming to provide comprehensive care for every myopic child.
Dr Fiona ‘Fi’ Om is the Professional Service Manager at CR Labs, manufacturer of MyoMe and MyoStock.. Dr Om started her career in the optical industry in 2017 as an optical dispenser. In 2019, she attained her Doctor of Optometry degree from the University of Melbourne and has been working as an optometrist in corporate and independent practices.
During her time in the corporate sector, she was awarded inaugural ‘Optometrist of the Year’ and has been globally recognised for her customer service. In mid-2023 she started her role at CR Labs, providing education and training to practices on CR’s range of specialty lenses.
 References
References
- Holden, B.A., Fricke, T.R., Resnikoff, S., et al., Global prevalence of myopia and high myopia and temporal trends from 2000 through 2050. Ophthalmology. 2016 May;123(5):1036–42. DOI: 10.1016/j.ophtha.2016.01.006.
- Flitcroft, D.I., The complex interactions of retinal, optical and environmental factors in myopia aetiology. Prog Retin Eye Res. 2012 Nov;31(6):622–60. DOI: 10.1016/j. preteyeres.2012.06.004.
- Bullimore, M.A., Brennan N.A. Myopia control: Why each diopter matters. Optom Vis Sci. 2019 Jun;96(6):463–465. DOI: 10.1097/OPX.0000000000001367.
- Erdinest, N., London, N., Levinger, N., et al., Peripheral defocus and myopia management: A mini-review. Korean J Ophthal. 2023 Feb;37(1):70–81. DOI: 0.3341/ kjo.2022.0125.
- Verkicharla, P.K., Mathur, A., Atchison, D.A., et al., Eye shape and retinal shape, and their relation to peripheral refraction. Ophthalmic Physiol Opt. 2012 May;32(3):184– 99. DOI: 10.1111/j.1475-1313.2012.00906.x.
- Faria-Ribeiro, M., Queirós, A., González-Méijome, J.M., et al., Peripheral refraction and retinal contour in stable and progressive myopia. Optom Vis Sci. 2013 Jan;90(1):9–15. DOI: 10.1097/OPX.0b013e318278153c.
- Gwiazda, J., Grice, K., Thorn, F., Response AC/A ratios are elevated in myopic children. Ophthalmic Physiol Opt. 1999 Mar;19(2):173–9. DOI: 10.1046/j.1475-1313.1999.00437.x.
- Mutti, D.O., Jones, L.A., Moeschberger, M.L., Zadnik, K., AC/A ratio, age, and refractive error in children. Invest. Ophthalmol. Vis. Sci. 2000;41(9):2469–78.
- Fulk, G.W., Cyert, L.A., Parker, D.E., A randomized trial of the effect of single-vision vs. bifocal lenses on myopia progression in children with esophoria. Optom Vis Sci. 2000 Aug;77(8):395–401. DOI: 10.1097/00006324- 200008000-00006.
- Gwiazda, J., Hyman, L., Scheiman, M., et al., A randomized clinical trial of progressive addition lenses versus single vision lenses on the progression of myopia in children. Invest Ophthalmol Vis Sci. 2003 Apr;44(4):1492– 500. DOI: 10.1167/iovs.02-0816.
- Sánchez-Tena, M.Á., Cleva, J.M., Alvarez-Peregrina, C., et al., Effectiveness of a spectacle lens with a specific asymmetric myopic peripheral defocus: 12-month results in a Spanish population. Children (Basel). 2024 Feb 1;11(2):177. DOI: 10.3390/children11020177.
- Australian Bureau of Statistics. Selected Living Cost Indexes, Australia [Internet]. Canberra: ABS; 2024 March. Available at: abs.gov.au/statistics/economy/price-indexesand- inflation/selected-living-cost-indexes-australia/latestrelease [accessed May 2024].
- Salvation Army, I’m having to go days without eating so my kids can eat. [Internet]. 1 May 2024. Available at: salvationarmy.org.au/about-us/news-and-stories/medianewsroom/ im-having-to-go-days-without-eating-so-mykids- can-eat/ [accessed May 2024].
- Aron-Dine, A., Einav, L., Finkelstein, A., The RAND health insurance experiment, three decades later. J Econ Perspect. 2013 Winter;27(1):197–222. DOI: 10.1257/jep.27.1.197.
- Chen, J., Rizzo, J.A., Rodriguez, H.P., The health effects of cost-related treatment delays. Am J Med Qual. 2011 Jul- Aug;26(4):261–71. DOI: 10.1177/1062860610390352.





