


When dry eye disease progresses slowly, patients can start to normalise their symptoms, writes Melbourne optometrist Jessica Chi.
Vanessa Bartos* first presented to the practice 12 years ago, complaining of eye strain performing near tasks with her progressive spectacles as she struggled to locate the correct zone to see through for each task. She was fitted with monthly disposable multifocal contact lenses and found them to be significantly more comfortable to wear than spectacles.
These lenses served her well for seven years, but she eventually began experiencing intermittent blurriness, especially when the lenses were over two weeks old. Upon examination, she was found to have dry eye disease with meibomian gland dysfunction (MGD) and anterior blepharitis. She was instructed to perform lid scrubs and hot compresses, and was refitted into multifocal daily disposable contact lenses (Dailies Total 1 Multifocal).
Ms Bartos managed well with these lenses until she returned three years later, now aged 68, complaining of intermittent blurry vision in the left eye noted over the past month. She described it as if she had moisturiser in her eye.
DED is a chronic, slowly progressive condition and she was unconscious of her other symptoms of dryness as… she had normalised her symptoms
Vision with her contact lenses was R 6/6, N5; L 6/7.5, N8, however vision was variable in the left. Ms Bartos reported that her vision would come in and out of focus with blinking. Examination revealed patchy contact lens surfaces with poor wettability, particularly in the left.
Tear film break-up time was four seconds in the right eye and three seconds in the left with MGD L>R. The glands were not easily expressible and the meibum that was expressed was thick and cloudy. Meibography with the Medmont Meridia revealed significant meibomian gland tortuosity and drop out (Figure 1).
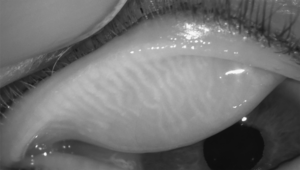



Figure 1. Meibography prior to treatment.
Ms Bartos’ ocular surface disease index (OSDI) score was 29, indicating moderate ocular surface disease. The OSDI is a 12-item questionnaire that evaluates ocular symptoms of ocular surface disease. The questions encompass ocular symptoms, vision-related function, and environmental triggers. The scores categorise patients into having a normal (0–12 points), mild (13–22 points), moderate (23–32 points) or severe (33–100 points) ocular surface disease.1
Ms Bartos had initially performed her hot compresses and lid hygiene for a brief period three years prior, however ceased once her symptoms improved. She was instructed to resume home treatment. She reported having a good diet, which followed a ‘Mediterranean diet’. A discussion was also held regarding intense pulsed light (IPL) treatment with debridement.
Treatment with Intense Pulsed Light
Ms Bartos returned two weeks later with minimal improvement and expressed frustration as she disliked wearing her spectacles and was struggling to see with her contact lenses. Two passes of IPL with the Lumenis M22 over the cheeks below the eyes as well as over the nose were performed, followed by lid margin debridement and manual meibomian gland expression.
She returned for three more sessions spaced a fortnight apart. By the third treatment Ms Bartos reported far less blur, and far less awareness of her eyes. She said she had not previously realised that they were uncomfortable – she had felt the discomfort was ‘normal’.
At the review following her fourth and final treatment, she reported dramatic improvement. Her OSDI score reduced to 21. She was still aware of some blur on some days upon waking in the morning, however this rarely lasted more than half an hour whereas in the past it could last all day, even without contact lens wear.
Examination revealed a tear film break-up time of seven seconds in the right and five seconds in the left. The glands were more easily expressible than at the commencement of treatment. Meibography revealed an improvement in the meibomian glands; there was filling of previously ghosted meibomian glands, as well as lengthening and straightening of glands (Figure 2).
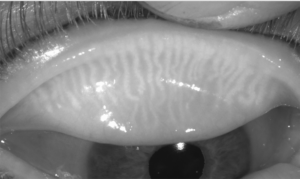



Figure 2. Meibography after treatment.
Dry Eye Disease
Dry eye disease (DED) has been classified by the Tear Film and Ocular Surface Society (TFOS) as “a multifactorial disease, characterised by a loss of homeostasis of the tear film, and accompanied by ocular symptoms, in which tear film instability and hyperosmolarity, ocular surface inflammation and damage, and neurosensory abnormalities play etiological roles”.2
The pathophysiology of DED is either aqueous deficient dry eye (ADDE) or evaporative dry eye (EDE), with the latter being the more common cause, however both aetiologies may be present. The leading causes for ADDE are Sjögren’s and lacrimal disease, whereas the main aetiology for EDE is meibomian gland dysfunction (MGD). The prevalence of DED has been reported from five to 50% with incidence increasing with age, and women being more affected than men.2
MGD results in tear film instability, which may manifest with symptoms such as dry, gritty, sore, and burning eyes. Tear film instability may also produce symptoms of fluctuating or blurry vision as was the case for Ms Bartos. Her main complaint was the blurry vision, and she assumed it was due to a change in her prescription. DED is a chronic, slowly progressive condition, and she was unconscious of her other symptoms of dryness as they had gradually come on and she had normalised her symptoms.
Treatments for DED should be tailored to target the cause. Treatments range from conservative self-management including artificial tears, warm compresses, lid scrubs, omega 3, and other dietary supplementation as well as modifying diet. Topical therapeutics such as corticosteroids, and immunosuppressive agents such as ciclosporin and autologous serum, may be administered but there can be potential complications or difficulties tolerating or obtaining these.
In-office treatments such as IPL, thermal massage devices such as Lipiflow, and low-level red light therapy have been shown to improve DED in many individuals.
When combined with meibomian gland expression, IPL has proven to be a safe and effective tool in our
armoury in managing the signs and symptoms of DED caused by EDE
Intense Pulsed Light
IPL is a non-invasive treatment that delivers broad-spectrum light pulses to deliver targeted heat. When applied to the periorbital area, IPL is believed to liquefy thickened meibum, improving meibomian gland secretions and promoting better gland function. It may also help reduce the bacterial load on the eyelid margin and surrounding adnexa, and induce photothermal damage to abnormal vessels, thus reducing inflammation and potentially disrupting the cycle of chronic inflammation. Additionally, IPL has been postulated to stimulate the parasympathetic nerves that innervate the meibomian glands, thereby further improving meibomian gland function.3,4
When combined with meibomian gland expression, IPL has proven to be a safe and effective tool in our armoury in managing the signs and symptoms of DED caused by EDE3-5 as seen in this case with Ms Bartos. There is often reluctance to invest time in diagnosing and managing DED, especially in patients who do not initially present with dry eye complaints. Additionally, the cost burden of treatment and new technologies such as IPL, as well as associated chair time, may deter patient and practitioner alike. However, dedicating time and effort to educate and treat these patients can dramatically improve a patient’s quality of life and foster long-term patient loyalty.
*Patient name changed for anonymity.
Jessica Chi is the Director of Eyetech Optometrists, an independent specialty contact lens practice in Melbourne. She is the current Victorian, and a past National President of the Cornea and Contact Lens Society, and an invited speaker at meetings throughout Australia and beyond. She is a clinical supervisor at the University of Melbourne, a member of Optometry Victoria Optometric Sector Advisory Group and a Fellow of the Australian College of Optometry, the British Contact Lens Association, and the International Academy of Orthokeratology and Myopia Control.
References
- Schiffman RM, Christianson MD, Reis BL, et al. Reliability and validity of the Ocular Surface Disease Index. Arch Ophthalmol. 2000 May;118(5):615-21.doi: 10.1001/archopht.118.5.615.
2. Craig JP, Nelson JD, Sullivan DA, et al. TFOS DEWS II Report Executive Summary. Ocul Surf. 2017 Oct;15(4):802-812. doi: 10.1016/j.jtos.2017.08.003.
3. Toyos R, McGill W, Briscoe D. Intense pulsed light treatment for dry eye disease due to meibomian gland dysfunction: A 3-year retrospective study. Photomed Laser Surg.2015 Jan;33(1):41-6. doi: 10.1089/pho.2014.3819.
4. Karaca EE, Evren Kemer Ö, Özek D. Intense regulated pulse light for the meibomian gland dysfunction. Eur J Ophthalmol. 2020 Mar;30(2):289-292. doi: 10.1177/1120672118817687.
5. Craig JP, Chen YH, Turnbull PR. Prospective trial of intense pulsed light for the treatment of meibomian gland dysfunction. Invest Ophthalmol Vis Sci, 2015;56(3):1965-70. doi: 10.1167/iovs.14-15764.





