
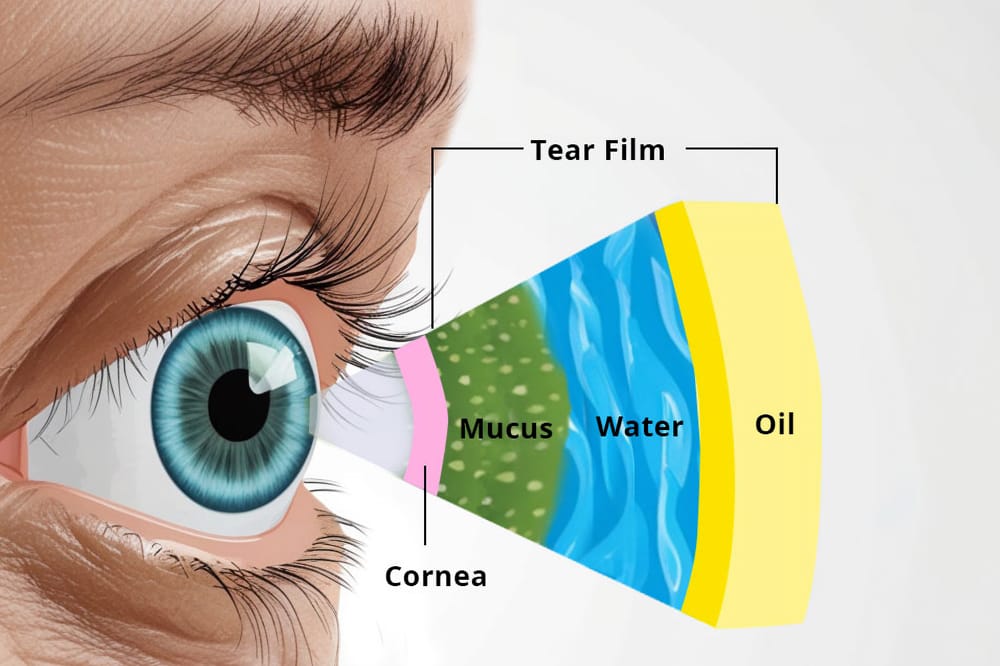
Figure 1. Layers in normal tear film.
With the burden of dry eye disease increasing, intense pulsed light (IPL) treatment and quantum molecular resonance (QMR) electrotherapy are proving to be useful tools in the dry eye armamentarium.
In this article, Adjunct Associate Professor Tze Lai and Dr Nicholas Ong review both the science behind the technology, and provide a useful guide as to how it has been incorporated into clinical practice at WA Eye Specialists.
Dry eye disease (DED) affects up to 50 million people worldwide and is driven by tear film hyperosmolarity (hyper-concentration of salts), structural instability, and rapid evaporation.1,2 In a normal tear film, there are three different layers of meibum (oil), aqueous (water), and mucous (proteins/carbohydrates) at fixed compositions that work in conjunction to lubricate and nourish the ocular surface.3 The meibum produced by the meibomian glands just beneath the eyelids is of a free-flowing olive oil texture that coats the surface of the eye, keeping the moisture locked in and preventing rapid evaporation.3-5 The aqueous produced by the lacrimal gland maintains the proper balance of electrolytes within the tear film, while the mucous produced by the goblet cells of the conjunctiva helps to provide additional lubrication.3
The causes for DED are multifactorial and range from various environmental factors, medical conditions/procedures, medications, diet, and changes to physiology,3 summarised in Table 1.8 The disease itself can be segregated into three different categories; aqueous deficient dry eye (ADDE), evaporative dry eye (EDE) or a combination of both.8 ADDE is characterised by a dysfunction in the production of aqueous by conditions affecting the lacrimal gland, resulting in hyper concentration of the salt content within the tear film, leading to early break down, and rapid evaporation.8 EDE, on the other hand, is primarily due to reduced meibum production, either from gland drop out or thickening of the meibum, which can subsequently occlude and cause the remaining glands to atrophy.9-12 Similar to the unstable tear film in ADDE, the loss of the moisture retaining oil also results in quicker evaporation, tear film instability, and hyper concentration of the salt content within the tear film.3,13
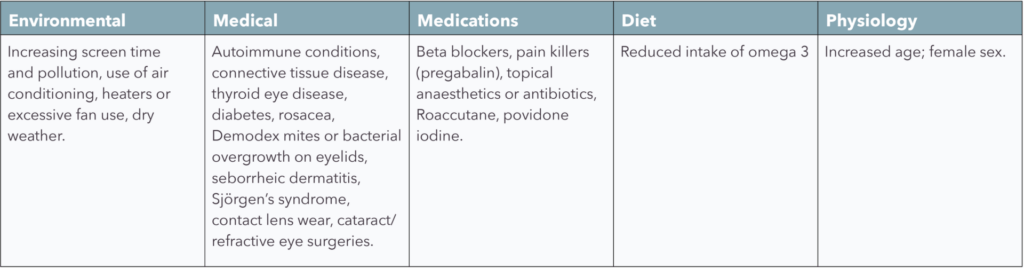
Table 1. Common causes of DED.8
Meibomian Gland Dysfunction
As most DED globally is caused by EDE and characterised by meibomian gland dysfunction (MGD),4,5,8,14,15 this article focusses on the causes of MGD and treatment.
While initially unnoticeable, prolonged MGD can lead to symptoms typical of dry eye disease such as: grittiness, burning, itch, pain, blurry vision, excessive tears, redness, foreign body sensation, and abnormal blood vessel growth (telangiectasias).16,17 If MGD is allowed to continue untreated, the remaining glands that become occluded can further atrophy, resulting in worsening dry eye symptoms.14,15,17
All forms of DED are associated with poorer quality of life scores. In a cross-sectional study of 78,165 participants, DED was associated with poorer physical and mental health outcomes compared to those that did not suffer from DED.18
At our own dry eye clinics at WA Eye Specialists, we have noted that 60% of clients have reported symptoms that were subjectively moderate to severe, with 48% reporting that their DED had a significant impact on quality of life, either limiting function or affecting the performance of tasks (Table 2).
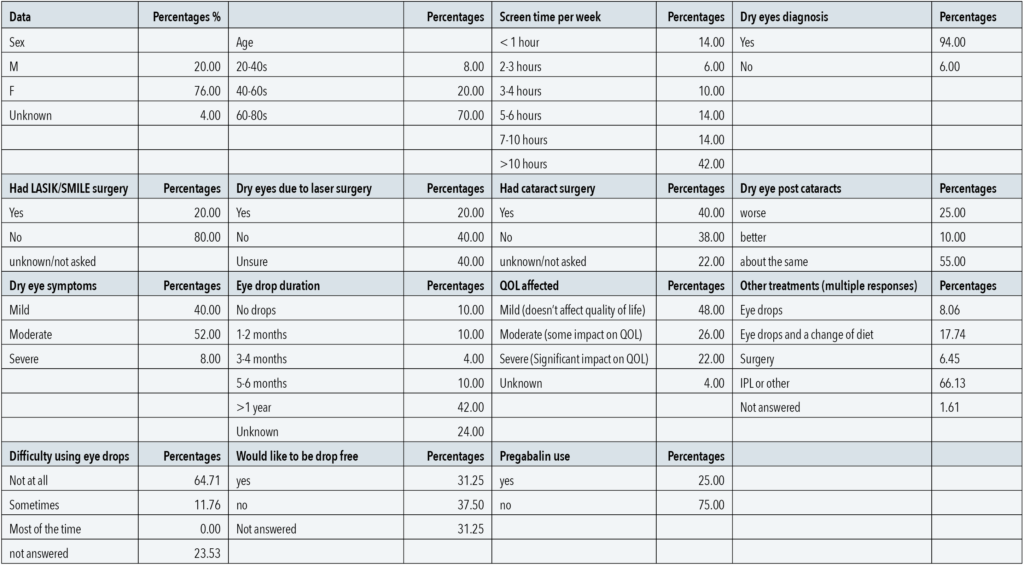
Table 2. Summary of data from WA Eye Specialists’ patient questionnaire. QOL = quality of life.
Unmodifiable Risk Factors
DED is more common in females (76%) compared with males (20%).8 Since the meibomian glands are regulated by circulating androgen sex hormones that are higher in concentration in men, it is not surprising that comparatively more women experience DED.8,19,20 Increasing age was also a risk factor for MGD associated DED.8 As people age, circulating androgen levels tend to decline, which can further compound the dysregulation of the meibomian glands.19-21 This could explain why most (70%) of the clients attending our dry eye clinics are between 60–80 years old.22
Meibomian gland dysfunction is the leading cause of dry eye disease with risk factors being female sex, age, cataract/ LASIK surgeries, increased screen time and other factors
Modifiable Risk Factors
Increased screen time is a modifiable risk factor for MGD8,23-26 as use of screens affects blinking characteristics by reducing blink rate and complete blinks, which in turn reduces the lipid spread over the ocular surface, resulting in increased evaporation.24 Not just limited to adults, increased screen time has also been associated with MGD in children as young as four years old.16,25-27
Given screens are now ubiquitous, it is important to provide patients with advice regarding the importance of taking short breaks from extensive screen use.28
From our own patient questionnaires, we found that 20–25% of clients experienced subjective worsening of their DED post cataract or LASIK (laser assisted in situ keratomileusis) surgery, a well-known phenomenon.29,30 As patients undergoing cataract surgery tend to be older (pre-existing risk factor) with other medical comorbidities such as diabetes, they are already predisposed to developing post-surgical exacerbations of their DED.8,31 Moreover, intraoperative preparation of the eye with povidone iodine for longer than 30 seconds has been associated with ocular toxicity that may further precipitate MGD.32,33
Manipulation of the cornea during surgery has been shown to disrupt the corneal nerve plexus, reducing corneal sensitivity, increasing blink rate, and worsening tear film instability.30,34 On top of the pre-operative and intra-operative risk factors, the use of topical anti-inflammatory or topical antibiotics is common practice after surgeries, which can damage the ocular surface if used for prolonged periods of time.32
Treatments
Given the link between surgery and worsening of DED symptoms discussed above, improvement of client satisfaction may require optimisation of all conditions before, during, and after the operation. For example, studies have shown improvement in symptoms of post-operative DED through three intense pulsed light (IPL) sessions spaced two weeks apart prior to eye surgery.35,36 Proper counselling, screening for DED with meibography, treatment with perioperative IPL, and reduction of the duration of ocular toxic medications may aid with symptom reduction and client satisfaction post-operatively.32
Additionally, there may also be a role in early treatment and regeneration of the meibomian glands with novel therapies, such as IPL therapy or quantum molecular resonance electrotherapy (QMR or Rexon-Eye).37-47
Currently, the mainstay of treatments for MGD includes lid hygiene wipes, topical antibacterial drops, topical lubricant drops, topical anti-inflammatories, or supplementation with foods rich in omega 3, which only results in a temporary resolution of symptoms.15,41,43,46,48,49 In our patient survey, we found 42% of clients were still using eye drops after one year, with 31% hoping to reduce their dependence on drops for symptom control. One study has reported that adherence to prescribed therapies such as eye drops could be as low as 10%.48 Oftentimes, because of the combinations of short-term relief, lack of commitment, poor adherence or sudden cessation, the return of dry eye symptoms is not uncommon.50
Intense Pulsed Light and Rexon-Eye
Use of IPL or Rexon-Eye in conjunction with other dry eye therapies has been shown in numerous studies to improve overall meibomian gland flow and function, as well providing secondary anti-bacterial and anti-inflammatory effects over an extended period of time.39-46
Initially used for dermatology and skin rejuvenation, the use of IPL was also noted to incidentally improve dry eye symptoms.42,51 By pulsing a light through a 500 nm filter in contact with the skin, the light is absorbed as heat in the meibomian glands, liquefying the viscous oil making the flow easier.42,51 Apart from enhancing oil flow, IPL is also useful in the treatment of blepharitis or eye lid inflammation caused by accumulation of bacteria and mites known as demodex along the lid margins.52 The associated inflammatory responses of the body to the bacteria or mites are a well-known cause of MGD.40,42,51 In IPL, the intense light and heat generated eradicates the demodex and bacteria and coagulates abnormal blood vessels, through which flow various pro-inflammatory mediators, which can occlude and further damage the existing meibomian glands.42,51 This creates a conducive environment for the damaged meibomian glands to recuperate and to be restored to original viability.42,51 With Rexon-Eye, instead of light, heat is generated through high frequency electric currents.53 Rexon-Eye’s QMR technology employs low-power, high-frequency electric fields to stimulate cellular metabolism and natural regeneration as well as reduce inflammation. It treats both meibomian glands as well as the lacrimal glands and has the benefit of treating clients who suffer from a combination of both ADDE and EDE.38,47,54
Treatment Plans
At a patient’s first visit to the clinic, an initial assessment is performed to assess the overall health of the ocular surface. This should include measuring the tear break-up time (TBUT), tear meniscus height, meibography, close up photos of telangiectasias/eye lid pathologies, and measuring the damage to the cornea with fluorescein dye.
After assessment, the treating dry eye clinician would generally recommend four initial sessions spaced two to four weeks apart and then four booster IPL sessions, with appointments for boosters separated across a period of three months to a year, depending on a client’s symptoms.37 The treatment schedule for Rexon-Eye is similar, with a recommendation for four initial treatments, each spaced one week apart.38 If a weekly session is not possible, the treatment for Rexon-Eye can be conducted every second week.
What Happens During Treatment?
At each treatment for IPL, the eyes are covered with eye shields and medical grade gel is applied to the malar region of the face. The appropriate filter is installed into the machine and the power settings can be adjusted up or down according to client comfort. The IPL probe is placed on a client’s lower lids and individual pulses of light are delivered at regularly spaced intervals from tragus to tragus. This is known as the first ‘pass’ and there two passes for each treatment.
For the Rexon-Eye treatment, the eyes are covered with a disposable tissue and the eye mask is fitted snugly. The power settings are adjusted, starting with ‘5’ and the eye mask is left on for 20 minutes.38 The eyes are treated one at a time with short intervals between each eye.
Sunscreen is applied after both treatment options and clients must be educated to avoid excess sun exposure/heat after treatment.40,47
Effects
Most effects of improved meibomian gland function with IPL and Rexon-Eye can be seen immediately, with effects lasting anywhere from days to weeks after the first two sessions. The effectiveness of the treatments extends with each session, with relief of symptoms lasting for six to eight months after completion of the four treatments.37,38
Comparing the Two
Currently, there are no studies comparing benefits between IPL and Rexon-Eye for the treatment of MGD and DED. Both treatments are very safe with most clients only reporting a slight increased warmth of the skin.37,38,42 When deciding on the treatments, there are a few features of each modality to consider, which I have outlined below.
Intense Pulsed Light
The intense light of IPL is absorbed by pigments within the skin, which helps to rejuvenate meibomian glands as well as lighten dark spots.55 Another advantage of IPL is that it is a quick procedure, taking only 10 to 20 minutes from set up to treatment.42,51 Unfortunately, the advantage that IPL has in lightening dark pigments also becomes its disadvantage. Since all pigments absorb light which is then converted to heat, IPL cannot be used in clients with Fitzpatrick IV skin types and above, as the heat absorbed may be too intense, leading to severe burns.42
Rexon-Eye
As mentioned above, Rexon-Eye uses high frequency electric currents instead of light. The heat generated is localised and can therefore be used in all skin tones. Another added benefit of Rexon-Eye is that it stimulates and promotes the natural regeneration of cells, which may improve both meibomian and lacrimal gland function.47,53,56
Take Home Points
DED causes significant stress to clients and can significantly impact quality of life.
Meibomian gland dysfunction is the leading cause of dry eye disease with risk factors being female sex, age, cataract/LASIK surgeries, increased screen time and other factors.
Given the large burden of DED, which will only increase over time, it is important to optimise ocular surface health by offering screening processes, providing good perioperative counselling, advising on screen time reduction/taking more frequent breaks, reducing duration of ocular toxic chemicals, and making referrals for perioperative IPL/Rexon-Eye treatments.
The use of novel treatments like IPL and Rexon-Eye, together with conventional DED treatments, have been shown to improve long-term control of symptoms by reducing eyelid inflammation and liquefying the meibum within the glands. Sessions spaced two to four weeks apart have shown good symptom relief for up to 18 months and early referral should be considered.
Adjunct Associate Professor Tze Lai MBBS BMedSc MPHC FRANZCO completed her ophthalmology specialist training in Western Australia prior to undertaking an internationally renowned surgical fellowship sub-specialising in complex cataract and glaucoma surgery (including minimal invasive glaucoma surgery), in Toronto, Canada. She practises in Perth at WA Eye Specialists and St John of God Healthcare.
Dr Nicholas Ong is a medical doctor who graduated from the University of Western Australia and practises at the Saint John of God health groups in Perth. He has a special interest in ophthalmology and is currently working on a dry eye disease research project with Adj Prof Lai at the WA Eye Specialists.
Figure 1. Layers in normal tear film.

Figure 2: Normal meibomian gland, with glands running parallel and for the full length of the eye lid. Images courtesy of the Clinical Research Centre, University of California Berkley.6

Figure 3: Tear system: a. tear gland / lacrimal gland, b. superior lacrimal punctum, c. superior lacrimal canal, d. tear sac / lacrimal sac, e. inferior lacrimal punctum, f. inferior lacrimal canal, g. nasolacrimal canal.7

Figure 4. Black arrows show abnormal blood vessels, grey arrows show meibomian gland obstruction.12








References
- Medzhitov R. Inflammation 2010: New adventures of an old flame. Cell. Mar 19 2010;140(6):771-6. doi: 10.1016/j.cell.2010.03.006.
- Rhee MK, Mah FS. Inflammation in dry eye disease: How do we break the cycle? Ophthalmology. Nov 2017;124(11S):S14-S19. doi: 10.1016/j.ophtha.2017.08.029.
- Yokoi N, Georgiev GA. Tear film-oriented diagnosis and tear film-oriented therapy for dry eye based on tear film dynamics. Invest Ophthalmol Vis Sci. Nov 1 2018;59(14):DES13-DES22. doi: 10.1167/iovs.17-23700.
- Fenga C, Aragona P, Cacciola A, et al. Meibomian gland dysfunction and ocular discomfort in video display terminal workers. Eye (Lond). Jan 2008;22(1):91-5. doi: 10.1038/sj.eye.6703025.
- Korb DR, Blackie CA. Meibomian gland therapeutic expression: quantifying the applied pressure and the limitation of resulting pain. Eye Contact Lens. Sep 2011;37(5):298-301. doi: 10.1097/ICL.0b013e31821bc7c5.
- Images courtesy of the Clinical Research Centre, University of California Berkeley. Distributed under Creative Commons licence. Originally appeared in Yeh TN, Lin MC. Risk factors for severe Meibomian gland atrophy in a young adult population: A cross-sectional study. PLoS One. 2017 Sep 28;12(9):e0185603. doi: 10.1371/journal.pone.0185603.
- Image by Silversmith, E. Distributed under Creative Commons licence. Available at: en.wikipedia.org/wiki/Lacrimal_gland [accessed September 2024].
- Craig JP, Nelson JD, Azar DT, et al. TFOS DEWS II Report Executive Summary. Ocul Surf. Oct 2017;15(4):802-812. doi: 10.1016/j.jtos.2017.08.003.
- Perra MT, Lantini MS, Sirigu P, et al. Human meibomian glands: a histochemical study for androgen metabolic enzymes. Invest Ophthalmol Vis Sci. Apr 1990;31(4):771-5.
- Sullivan DA, Rocha EM, Ullman MD, et al. Androgen regulation of the meibomian gland. Adv Exp Med Biol. 1998;438:327-31. doi: 10.1007/978-1-4615-5359-5_46.
- Krenzer KL, Dana MR, Ullman MD, et al. Effect of androgen deficiency on the human meibomian gland and ocular surface. J Clin Endocrinol Metab. Dec 2000;85(12):4874-82. doi: 10.1210/jcem.85.12.7072.
- Sullivan DA, Sullivan BD, Ullman MD, et al. Androgen influence on the meibomian gland. Invest Ophthalmol Vis Sci. Nov 2000;41(12):3732-42.
- Pflugfelder SC, Stern ME. Biological functions of tear film. Exp Eye Res. Aug 2020;197:108115. doi: 10.1016/j.exer.2020.108115.
- Bu J, Guo Y, Wu Y, et al. Models for meibomian gland dysfunction: In vivo and in vitro. Ocul Surf. Mar 13 2024; doi: 10.1016/j.jtos.2024.03.003.
- Deo N, Nagrale P. Dry eye disease: An overview of its risk factors, diagnosis, and prevalence by age, sex, and race. Cureus. Feb 2024;16(2):e54028. doi: 10.7759/cureus.54028.
- Yang I, Sacho IBI, Lopes GA, et al. Dry eye prevalence and main risk factors among brazilian medical students. Invest Ophthalmol Vis Sci. 2019;60(2740).
- Golden MI, Meyer JJ, Patel BC. Dry eye syndrome. StatPearls. 2024.
- Morthen MK, Magno MS, Vehof J, et al. The physical and mental burden of dry eye disease: A large population-based study investigating the relationship with health-related quality of life and its determinants. Ocul Surf. Jul 2021;21:107-117. doi: 10.1016/j.jtos.2021.05.006.
- Lienert JP, Tarko L, Schaumberg DA, et al. Long-term natural history of dry eye disease from the patient’s perspective. Ophthalmology. Feb 2016;123(2):425-433. doi: 10.1016/j.ophtha.2015.10.011.
- Chhadva P, Goldhardt R, Galor A. Meibomian gland disease: The role of gland dysfunction in dry eye disease. Ophthalmology. Nov 2017;124(11S):S20-S26. doi: 10.1016/j.ophtha.2017.05.031.
- Swerdloff RS, Wang C. Androgen deficiency and aging in men. West J Med. 1993;159(5):579-585.
- Wiedemann J, Kashgari G, Lane S, et al. The effects of age and dysfunction on meibomian gland population dynamics. Ocul Surf. Aug 8 2024;34:194-209. doi: 10.1016/j.jtos.2024.08.005.
- Iyer JV, Lee SY, Tong L. The dry eye disease activity log study. Scientific World Journal. 2012;2012:589875. doi: 10.1100/2012/589875.
- Argiles M, Cardona G, Perez-Cabre E, Rodriguez M. Blink rate and incomplete blinks in six different controlled hard-copy and electronic reading conditions. Invest Ophthalmol Vis Sci. Oct 2015;56(11):6679-85. doi: 10.1167/iovs.15-16967.
- Kocamis O, Temel E, Asikgarip N, Ornek K. electronic device screen time and meibomian gland morphology in children. J Ophthalmic Vis Res. Oct-Dec 2021;16(4):531-537. doi: 10.18502/jovr.v16i4.9741.
- Muntz A, Turnbull PR, Kim AD, et al. Extended screen time and dry eye in youth. Cont Lens Anterior Eye. Oct 2022;45(5):101541. doi: 10.1016/j.clae.2021.101541.
- Gupta PK, Stevens MN, Kashyap N, Priestley Y. Prevalence of meibomian gland atrophy in a pediatric population. Cornea. Apr 2018;37(4):426-430. doi: 10.1097/ICO.0000000000001476.
- Neurosurgery OaSs, PC. 5 Compelling Reasons to Reduce Screen Time for Better Health. Available at: nossmd.com/5-compelling-reasons-to-reduce-screen-time-for-better-health/#:~:text=Excessive%20screen%20time%20often%20results,improve%20posture%20and%20alleviate%20discomfort [accessed June 2024].
- Naderi K, Gormley J, O’Brart D. Cataract surgery and dry eye disease: A review. Eur J Ophthalmol. Sep 2020;30(5):840-855. doi: 10.1177/1120672120929958.
- Kim JH, Chung JL, Seo KY, et al. Change in corneal sensitivity and corneal nerve after cataract surgery. Cornea. 2009;28(11):20-25. doi: 10.1097/ICO.0b013e3181aea0e3.
- Chentli F, Azzoug S, Mahgoun S. Diabetes mellitus in elderly. Indian J Endocrinol Metab. Nov-Dec 2015;19(6):744-52. doi: 10.4103/2230-8210.167553.
- Giannaccare G, Barabino S, Di Zazzo A, Villani E. Preventing and managing iatrogenic dry eye disease during the entire surgical pathway: A study focusing on patients undergoing cataract surgery. J Clin Med. Jan 27 2024;13(3). doi: 10.3390/jcm13030748.
- Pels E, Vrensen GF. Microbial decontamination of human donor eyes with povidone-iodine: penetration, toxicity, and effectiveness. Br J Ophthalmol. Sep 1999;83(9):1019-26. doi: 10.1136/bjo.83.9.1019.
- Rahman EZ, Lam PK, Chu CK, Moore Q, Pflugfelder SC. Corneal Sensitivity in Tear Dysfunction and its Correlation With Clinical Parameters and Blink Rate. Am J Ophthalmol. Nov 2015;160(5):858-866 e5. doi:10.1016/j.ajo.2015.08.005
- Mencucci R, Mercuri S, Cennamo M, Morelli A, Favuzza E. Efficacy of vector thermal pulsation treatment in reducing postcataract surgery dry eye disease in patients affected by meibomian gland dysfunction. J Cataract Refract Surg. Apr 1 2023;49(4):423-429. doi: 10.1097/j.jcrs.0000000000001124.
- Martínez-Hergueta MC, Cantó-Cerdán M, Amesty MA, et al. Perioperative intense pulsed light to prevent and improve symptoms of post-laser corneal refractive surgery dry eye. A randomized clinical trial. Asia-Pacific Journal of Ophthalmology. 2024;13(1). doi: 10.1016/j.apjo.2023.100029.
- Eyetek. TearStim world leading dry eye management. 2024 (webpage). Available at: eyetek.com.au/product/ipl-dry-eye-tearstim.html [accessed Sept 2024].
- Eyetek. Rexon-Eye Reinvent Dry Eye Treatment. 2024 (webpage). Available at: eyetek.com.au/product/rexon-eye.html [accessed Sept 2024].
- Craig JP, Chen YH, Turnbull PR. Prospective trial of intense pulsed light for the treatment of meibomian gland dysfunction. Invest Ophthalmol Vis Sci. Feb 12 2015;56(3):1965-70. doi: 10.1167/iovs.14-15764.
- Rong B, Tang Y, Tu P, et al. intense pulsed light applied directly on eyelids combined with meibomian gland expression to treat meibomian gland dysfunction. Photomed Laser Surg. Jun 2018;36(6):326-332. doi: 10.1089/pho.2017.4402.
- Giannaccare G, Taroni L, Senni C, Scorcia V. intense pulsed light therapy in the treatment of meibomian gland dysfunction: Current perspectives. Clin Optom (Auckl). 2019;11:113-126. doi: 10.2147/OPTO.S217639.
- Toyos R, Toyos M, Willcox J, Mulliniks H, Hoover J. Evaluation of the safety and efficacy of intense pulsed light treatment with meibomian gland expression of the upper eyelids for dry eye disease. Photobiomodul Photomed Laser Surg. Sep 2019;37(9):527-531. doi: 10.1089/photob.2018.4599.
- Cote S, Zhang AC, Ahmadzai V, et al. Intense pulsed light (IPL) therapy for the treatment of meibomian gland dysfunction. Cochrane Database Syst Rev. Mar 18 2020;3(3):CD013559. doi: 10.1002/14651858.CD013559.
- Wu Y, Mou Y, Zhang Y, et al. Efficacy of intense pulsed light combined blood extract eye drops for treatment of nociceptive pain in dry eye patients. J Clin Med. Feb 27 2022;11(5). doi: 10.3390/jcm11051312.
- Qin G, Chen J, Li L, et al. Efficacy of intense pulsed light therapy on signs and symptoms of dry eye disease: A meta-analysis and systematic review. Indian J Ophthalmol. Apr 2023;71(4):1316-1325. doi: 10.4103/IJO.IJO_2987_22.
- Gade A, Vasile GF, Rubenstein R. Intense pulsed light (IPL) therapy. StatPearls. 2024.
- Shemer A, Altarescu A, Nusbaum L, et al. quantum molecular resonance effects on patients with dry eye disease: A randomized controlled trial. Cornea. Dec 28 2023. doi: 10.1097/ICO.0000000000003443.
- Uchino M, Yokoi N, Shimazaki J, Hori Y, Tsubota K, On behalf of the Japan Dry Eye S. Adherence to eye drops usage in dry eye patients and reasons for non-compliance: A web-based survey. J Clin Med. Jan 12 2022;11(2). doi: 10.3390/jcm11020367.
- Sheppard J. Dry eye symptoms return with cyclosporine cessation. Ophthalmology Times 2024. Available at: ophthalmologytimes.com/view/dry-eye-symptoms-return-cyclosporine-cessation [accessed Sept 2024].
- Semp DA, Beeson D, Sheppard AL, Dutta D, Wolffsohn JS. Artificial tears: A systematic review. Clin Optom (Auckl). 2023;15:9-27. doi: 10.2147/OPTO.S350185.
- Toyos R, McGill W, Briscoe D. Intense pulsed light treatment for dry eye disease due to meibomian gland dysfunction; A 3-year retrospective study. Photomed Laser Surg. Jan 2015;33(1):41-6. doi: 10.1089/pho.2014.3819.
- Barnett M, Simmons B, Vollmer P, et al. The impact of Demodex blepharitis on patient symptoms and daily life. Optom Vis Sci. Mar 1 2024;101(3):151-156. doi: 10.1097/OPX.0000000000002111.
- Foo VHX, Liu YC, Tho B, Tong L. Quantum molecular resonance electrotherapy (Rexon-Eye) for recalcitrant dry eye in an Asian population. Front Med (Lausanne). 2023;10:1209886. doi: 10.3389/fmed.2023.1209886.
- Ophthalmic R. 2024. Available at: resono.it/rexon-eye/ [accessed Sept 2024].
- Tan JM, Joonho Jo J, Chelnis J. Effects of IPL and RF treatment on meibomian gland regeneration and patient experience of dry eye disease. presented at: ARVO annual meeting abstract; 2023; Available at: iovs.arvojournals.org/article.aspx?articleid=2790039&resultClick=1 [accessed Sept 2024].
- Fraccalvieri M, Salomone M, Bruschi S, et al. Quantum molecular resonance technology in hard-to-heal extremity wounds: histological and clinical results. Int Wound J. Dec 2017;14(6):1313-1322. doi: 10.1111/iwj.12805.





