

Flarex (fluorometholone acetate 0.1%) suspension eye drops were withdrawn from the Australian pharmaceutical market on 30 June 2024, with the remaining supply continuing to be available until exhausted. Manufacturer Novartis Pharmaceuticals Australia Pty Ltd cited changes to commercial viability as justification for the discontinuation.1 This change has implications for clinical practice and the effective management of ophthalmic disease. Thomas Ford considers the alternative topical corticosteroid preparations available to Australian optometrists.
Faced with a dwindling supply of Flarex (fluorometholone acetate 0.1%) suspension eye drops in Australia, it is beholden on clinicians to familiarise themselves with alternative topical corticosteroid preparations that elucidate a similar therapeutic effect in cases where Flarex was previously indicated, while being mindful of the consequences of doing so.
Publicly available data from Services Australia indicates the total number of pharmaceutical benefits scheme (PBS) and repatriation PBS (RPBS) prescriptions issued, though does not account for private prescriptions. Figure 1 presents PBS/RPBS topical corticosteroid prescribing data by Australian optometrists between July 2023 and June 2024.2
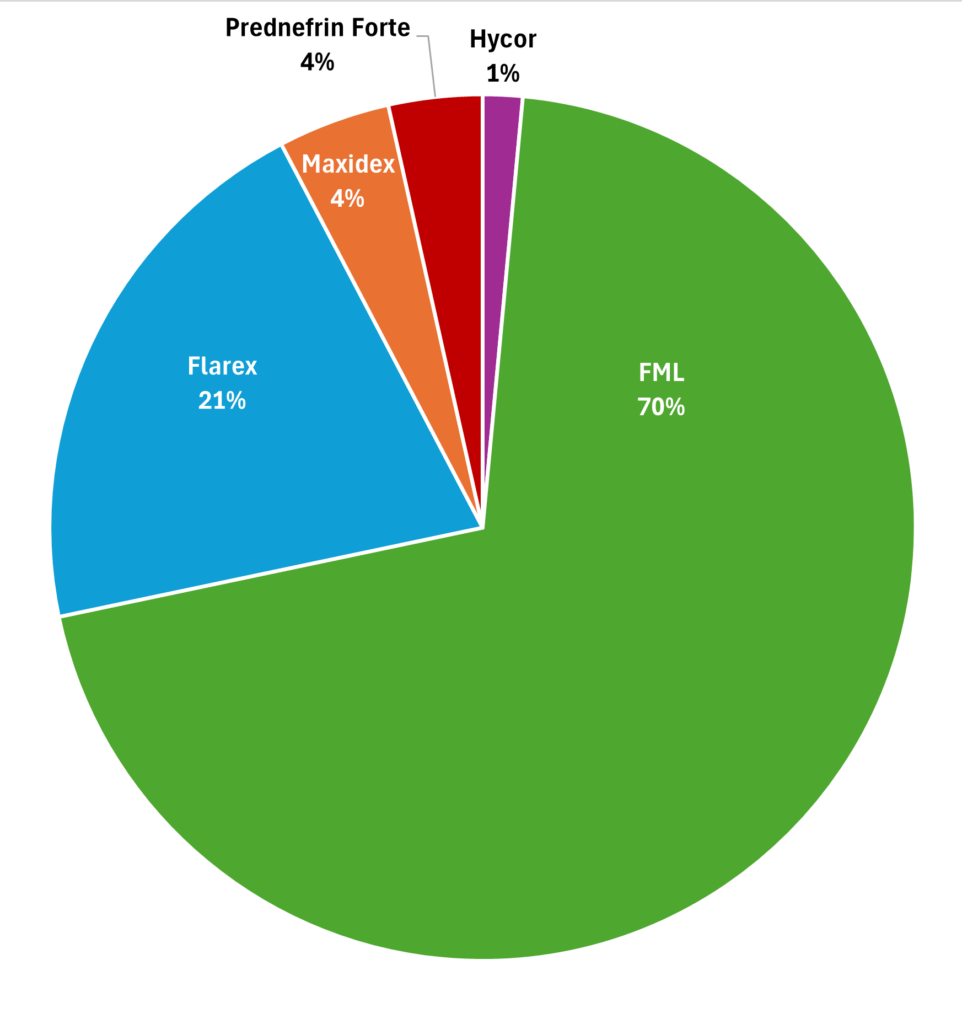
Figure 1. PBS/RBPS topical corticosteroid prescribing by Australian optometrists from July 2023 to June 2024.2
A predominance of FML (fluorometholone alcohol 0.1%) prescribing was subsidised by Services Australia during this period, accounting for 70% of PBS/RPBS prescriptions in the 2023–24 financial year. This was followed by Flarex at 21%, which has steadily declined in popularity since July 2022, with almost 7,000 fewer Flarex prescriptions filled in the last financial year compared to 2021–22. In contrast, Maxidex (dexamethasone alcohol 0.1%) and Prednefrin Forte (prednisolone acetate 1%, phenylephrine 0.12%) each contributed 4%, followed by Hycor ointment (hydrocortisone acetate 1%) at 1%.
Treatment Philosophy
The philosophy underpinning the prescribing of topical corticosteroids requires clinicians to consider a balanced regimen, that is, the most appropriate drug dosage to produce the maximum therapeutic effect with minimum adverse effects. Practitioners should consult evidence-based resources and seek expert counsel in instances where their scope of knowledge, confidence or experience is exceeded.
Pharmaceutical Formulation
Topical formulations may be prepared as a suspension, solution or ointment in the presence or absence of preservative. Acetates and alcohols form suspensions, whereas solutions are composed of phosphates. Critically, the efficacy of each preparation depends not only on the intrinsic potency of the active drug(s), but also on its penetration and durability.3
Potency Versus Penetrance
A core tenet in the prescribing of corticosteroids is the relationship between potency and penetrance. Penetrance is dependent upon drug concentration, chemical formulation and vehicle composition; where greater penetrance allows for lower corticosteroid concentrations to be considered, given its direct therapeutic action at the site of ocular inflammation.4,5
Lipophilic acetate bases, such as Flarex, allow increased binding to glucocorticoid receptors and possess greater penetration of the intact cornea than alcohols, such as FML and Maxidex.6 Further, suspensions are advantageous in that their properties allow prolonged precorneal resident time, aiding transcorneal penetration and prolonged duration of action.7
Pharmacological Properties
Flarex Legacy
Flarex was primarily indicated in steroid-responsive inflammatory conditions of the conjunctiva, cornea, and anterior segment. As an acetate derivative, Flarex reduced inflammation at a greater rate than the alcohol-based FML within the corneal stroma, given its lipophilic properties, thus allowing more effective transcorneal penetration. Further, Flarex was more effective within the corneal stroma, both in the presence and absence of a corneal epithelial defect, compared to Maxidex.8,9
Therefore, given its discontinuation, clinicians must prescribe an alternative that contains sufficient potency and penetrance properties to elucidate an appropriate therapeutic benefit, while reducing the risk of adverse effects.
FML versus Maxidex
Despite FML being 1.6-times the relative potency of Maxidex, poor penetrance of the intact corneal epithelium results in FML having approximately half the corneal stromal therapeutic effect of Maxidex. In instances of epithelial compromise, however, FML has a similar efficacy to that of Maxidex.10,11
The mean peak concentration of Maxidex within the aqueous humour is over six-times greater than FML (Table 1). Further, significant concentrations of active drug from FML and Maxidex preparations remain detectable within the aqueous following administration; totalling four hours and 12 hours, respectively.10-12
Prescribing Decisions in Ocular Disease
FML is effective within the corneal epithelium, anterior stroma, and episclera, whereas Maxidex exhibits its greatest efficacy within the posterior corneal stroma and anterior chamber. This is key to guiding the therapeutic management of ocular diseases.
FML is indicated for moderate to severe ocular surface inflammation, where therapy is expected to be short term without potent posterior stromal penetrance. However, its low adverse effect profile makes it suitable for use in cases of prolonged ocular surface and anterior corneal disease.15
For instance, symptomatic moderate to severe inflammatory dry eye would be appropriately managed via a course of FML, as per the TFOS DEWS II Reports.16 FML would also be indicated in the presence of a central anterior stromal scar, following metallic foreign body removal. Whereas Maxidex would be more appropriate in cases of posterior stromal disease.17
Similarly, sterile subepithelial infiltrates present in cases of contact lens-associated red eye would be appropriately managed via FML, in conjunction with prophylactic antibacterial agents. In contrast, peripheral stromal infiltrates secondary to marginal keratitis may result in the clinician opting for a short, titrated course of Maxidex, following an appropriate period of topical antibiotic use to limit bacterial colonisation.18 Of course, in such cases, infiltrative aetiology must be considered prior to commencing treatment, where prescribers should proceed with caution in the presence of an epithelial defect.
Post-surgical inflammation following cataract or refractive laser procedures tends to result in the prescribing of Maxidex, however, post-corneal graft and bouts of acute anterior uveitis indicate the use of preparations with greater penetrance, such as Prednefrin Forte.17-20 The penetrance properties of Prednefrin Forte are also of benefit in severe, central bacterial keratitis, and stromal or endothelial herpes simplex keratitis, as described in the SCUT and HEDS trials, respectively.21-23
Conclusion
Corticosteroids play an important role in the effective management of ophthalmic disease. As such, clinicians must remain cognisant of alternative topical corticosteroid preparations that elucidate a similar therapeutic effect in cases where Flarex was previously indicated, while being mindful of the consequences of doing so. Practitioners should also seek expert counsel in instances where their scope of knowledge, confidence or experience is exceeded.
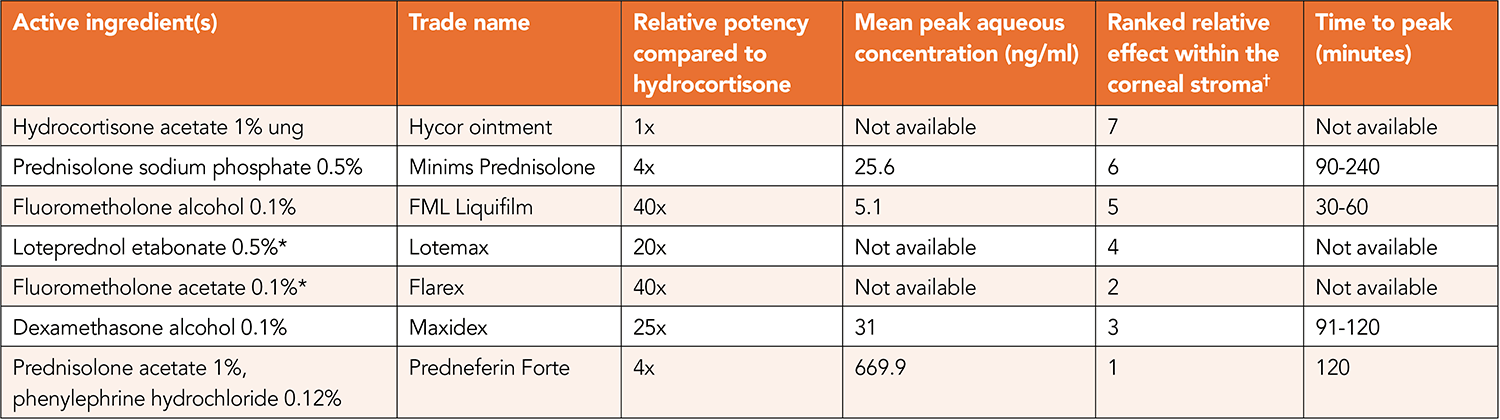
Table 1. Topical corticosteroids approved for prescribing by therapeutically endorsed optometrists in Australia.10,11,13,14
* Indicates preparations not commercially available in Australia. † Ranking where 1 indicates greatest corneal stromal penetrance with 7 being the lowest.
Practitioners should also seek expert counsel in instances where their scope of knowledge, confidence or experience is exceeded.
The full CPD version of this article will feature in mivision’s April 2025 issue.
The author wishes to acknowledge Dr Alex Hui from the University of New South Wales School of Optometry and Vision Science, for review of this article.
Thomas Ford BMedSc(VisSc) MOptom AdvCertGlauc is a therapeutically endorsed optometrist with George and Matilda Eyecare. He has experience in private ophthalmology and has completed further studies in paediatric eye care and glaucoma. Interests include the therapeutic management of ophthalmic disease and myopia control, where he frequently co-manages complex cases with ophthalmology. In 2024, Mr Ford was awarded the South Australian Rural Health Award for outstanding clinical excellence and patient care.
References
- Therapeutic Goods Administration. Fluorometholone acetate – medicine shortage information 2024. apps.tga.gov.au/shortages/Search/Details/fluorometholone%20acetate [accessed October 2024].
- Services Australia. Pharmaceutical Benefits Schedule Item Reports 2024. Available from: medicarestatistics.humanservices.gov.au/statistics/pbs_item.jsp [accessed October 2024].
- Price G, Patel D. Drug bioavailability: StatPearls Publishing; 2023.
- Agarwal P, Rupenthal ID. Non-aqueous formulations in topical ocular drug delivery – A paradigm shift? Advanced Drug Delivery Reviews. 2023;198:114867.
- McGhee C, Danesh-Meyer H. Locally administered ocular corticosteroids: benefits and risks. Drug Safety. 2002;25(1):33-55.
- Sheppard J, Comstock T, Cavet M. Impact of the topical ophthalmic corticosteroid loteprednol etabonate on intraocular pressure. Advanced Therapeutics. 2016;33(4):532-52.
- Grassiri B, Zambito Y, Bernkop-Schnürch A. Strategies to prolong the residence time of drug delivery systems on ocular surface. Advances in Colloid and Interface Science. 2021;288:102342.
- Therapeutic Goods Administration. Flarex fluorometholone acetate 1mg/mL eye drops suspension 2024. tga.gov.au/resources/artg/25278 [accessed October 2024].
- Leibowitz H, Hyndiuk R, Lindsey C, Rosenthal A. Fluorometholone acetate: clinical evaluation in the treatment of external ocular inflammation. Annals of Ophthalmology. 1984;16(12):1110-5.
- McGhee C, Midgley J, Fern A, et al. Penetration of synthetic corticosteroids into human aqueous humour. Eye. 1990;1990(4):526-30.
- Watson D, Dutton G, Midgley J, Healey T. Penetration of topically applied dexamethasone alcohol into human aqueous humor. Archives of Ophthalmology. 1988;106(5):686-7.
- Awan MA, Agarwal PK, Dutton GN, et al. Penetration of topical and subconjunctival corticosteroids into human aqueous humour and its therapeutic significance. British Journal of Ophthalmology. 2009;93(6):708.
- McGhee C, Noble M, Healey T, et al. Penetration of topically applied prednisolone sodium phosphate into human aqueous humour. Eye. 1989;1983(3).
- Pavan-Langston D. Manual of ocular diagnosis and therapy. Sixth edition: Taylor & Francis; 2009.
- Therapeutic Goods Administration. FML fluorometholone 1mg/mL eye drops 2024 tga.gov.au/resources/artg/23212 [accessed October 2024].
- Craig JP, Nichols KK, Joo C-K, et al. TFOS DEWS II definition and classification report. The Ocular Surface. 2017;15(3):276-83.
- Mofidfar M, Abdi B, Abbasi F, et al. Drug delivery to the anterior segment of the eye: A review of current and future treatment strategies. International Journal of Pharmacy. 2021;25(607).
- Mazet R, García-Otero X, Bossard F, et al. Biopharmaceutical assessment of dexamethasone acetate-based hydrogels combining hydroxypropyl cyclodextrins and polysaccharides for ocular delivery. Pharmaceutics. 2020;12(8):717.
- Roth M. Optometry in Australia is a therapeutic profession. Clinical and Experimental Optometry. 2007;90(2):67-9.
- Gutteridge I, Hall A. Acute anterior uveitis in primary care. Clinical and Experimental Optometry. 2007;90(2):70-82.
- Srinivasan M, Mascarenhas J, Glidden D, et al. Corticosteroids for bacterial keratitis: the Steroids for Corneal Ulcers Trial (SCUT). Archives of Ophthalmology. 2012;130(2):143-50.
- Srinivasan M, Mascarenhas J, Lalitha P, O’Brien K, et al. The steroids for corneal ulcers trial (SCUT): secondary 12-month clinical outcomes of a randomized controlled trial. Americal Journal of Ophthalmology. 2014;157(2):327-33.
- Wilhelmus K, Hauck W, Jones D, et al. Herpetic Eye Disease Study. A controlled trial of topical corticosteroids for herpes simplex stromal keratitis. Ophthalmology. 1994;101(12):1883-96.





