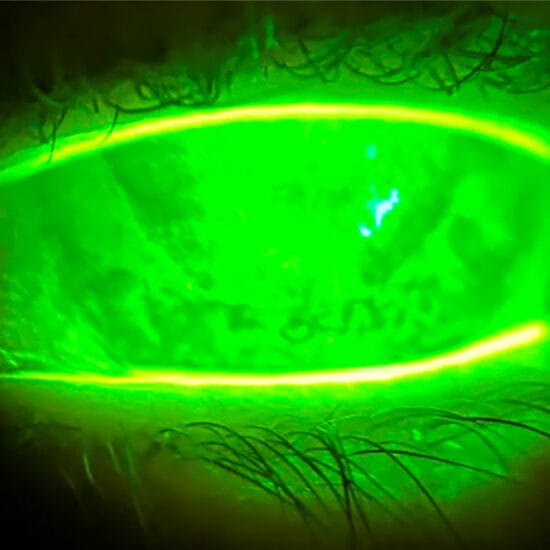
Figure 1. PHPV stalk from the optic disc to the posterior lens surface.
Visual disorders can impact a child’s educational, social, emotional, and physical development, especially if there is a delayed diagnosis. Dr Margaret Lam asked Dr Craig Donaldson AM about paediatric eye health, and the advice to offer parents.
Q: What protocols do you recommend for early screening to catch common vision disorders in children, such as amblyopia or refractive errors, and what are the critical age checkpoints?
Ideally, screening of children for visual disorders should be undertaken as soon as practicable. Newborns are given paediatrician review and can be relatively easily evaluated for any obvious ocular misalignment or anterior segment abnormality. Assessment of the red reflex with an indirect ophthalmoscope is crucial, as it can help rule out ocular media opacities such as cataract, as well as serve as a rough screening test for posterior segment abnormalities including retinoblastoma.
Assessing vision in young children is problematic as specialised tools and experience are necessary due to the variable ability of children to perform vision tests. Various screening programs are currently employed around Australia, such as the StEPS (Statewide Eyesight Preschooler Screening) in New South Wales. This occurs in four-year-olds at pre-school and has proven successful in identifying children with refractive error, strabismus, amblyopia, etc., with subsequent referral to eye care health professionals.
It is crucial for parents and guardians to understand the importance of vision screening, particularly when there is a family history of ocular abnormalities. Earlier eye examinations for children can be conducted by an optometrist or ophthalmologist.
Q: How do factors like outdoor time and exposure to natural light impact visual development in children, and what recommendations do you make to parents on this front?
It has been established that exposure to outdoor light plays a beneficial role in reducing the probability of developing myopia and axial elongation. Various myopia risk factors have been identified, and exposure to outdoor light for less than 14 hours per week correlates with a higher chance of myopia. I discuss this information with parents and encourage them to try and have their children spend some time outdoors. Wearing a hat and or sunglasses does not stop the beneficial effect. I ask children if, while at school, they spend morning tea and lunch outdoors or if they stay indoors. If they stay indoors, I encourage them to go outside. Parents may not be aware of their child’s morning tea and lunchtime habits.
Q: With the rising prevalence of myopia, particularly in younger populations, what are the most promising preventative strategies or interventions that you currently recommend?
Firstly, routine screening of children, especially if there is a family history of myopia. We know that some children are highly likely to become myopic and that includes those with affected parents, lower hyperopia for age than expected, as well as greater than three hours per day with near visual tasks. Early diagnosis of myopia and pre-myopia, followed by implementation of treatment strategies, is more likely to reduce the chance of myopic progression. Exposure to outdoor light, as mentioned earlier, is inexpensive and relatively easy to obtain given Australia’s climate. Parental education regarding myopia and therapeutic options is critical. Treatment strategies for myopia vary between practitioners. I generally commence the myope with peripheral defocus lenses and review in three months. If progression has occurred as established by vision, cycloplegic refraction, and axial length measurements, I add low dose atropine eye drops. Other options include orthokeratology and repeated low dose red light therapy. Recent meta-analyses have shown only a relatively low risk of infection with orthokeratology and a beneficial effect on myopia control.1,2,3 Further research is continuing on red light therapy with promising results thus far.
Q: Given children’s increasing use of digital devices, what guidelines do you provide to reduce digital eye strain, and how concerned should parents be about the potential long-term effects on their child’s vision?
Parents of myopic children almost routinely mention or enquire about the effects of close work and particularly digital devices. An enormous amount of research has been undertaken to try to establish the effects of digital devices on the visual system. Close reading distance (≤20 cm) and continuous reading (>45 mins) have, in some research, been shown to increase the odds of myopia,4 however the benefits of extending the viewing distance have yet to be proven. Meta-analyses of the use of smart devices have largely been limited to Asian populations, however a more recent review did show an association between myopia and the use of smart devices in combination with a computer.5,6 Behavioural changes with less outdoor activity may be contributory.
The problem is, that with normal schooling and social interaction, it is near impossible to avoid digital devices and computers. Young children should have very limited screen time and older children should be persuaded to engage in outdoor activities rather than remaining indoors with digital devices. Despite the lack of proven benefit, I still recommend viewing screens at preferably a distance greater than 30 cm.
Q: How do you approach cases where there is a family history of serious eye conditions, and what preventive measures or genetic screenings are particularly useful in these situations?
There are numerous systemic conditions associated with ocular abnormalities and a genetic cause has been established for nearly all of these. Refractive error, cataract, ocular dysgenesis, strabismus, glaucoma, and so forth can all have underlying genetic and systemic links. As an example, retinoblastoma has a very well-established genetic basis – the RB1 tumour suppressor gene on chromosome 13 – and approximately 40% of cases are hereditary. This is a cancer of young children. Affected parents need to be educated regarding the need for prenatal and early post-natal evaluation of their children by an ophthalmologist. The same general rule applies for other ocular conditions with early, and perhaps repeated, assessments performed on children of parents known to be affected with genetic disorders.
Case Study
A six-month-old baby boy, otherwise in good health and of term birth, was noted by his mother to have a left white pupil. The child had been reviewed by the paediatrician soon after birth and no abnormalities were detected. There was no family history of ocular abnormalities in childhood. The child was taken to the family general practitioner who confirmed leukocoria and referred for immediate ophthalmic review. On examination, the left globe was found to have a corneal diameter of 10.0 mm and right 11.0 mm. Figure 1 (above) shows the left posterior segment.

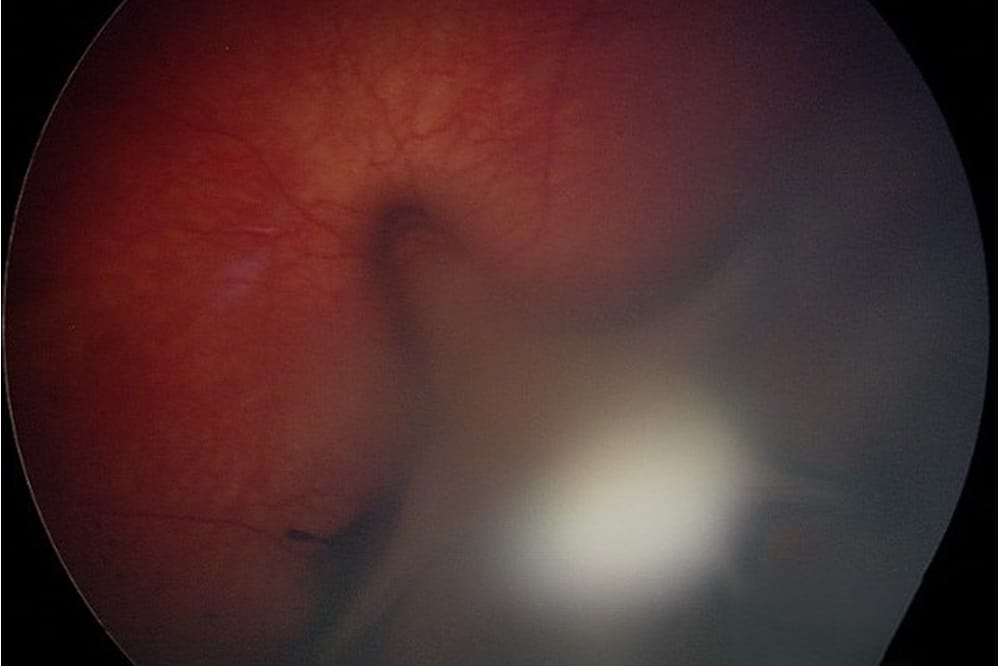
Figure 2. Numerous large retinoblastomas in a six-month-old child.
An ultrasound of the left eye confirmed persistent hyperplastic primary vitreous (PHPV), also known as persistent foetal vasculature, with a vascular chord extending from the optic disc to the posterior surface of the lens, which was developing a cataract. Surgery was organised to remove the cataract and dissect the PHPV. The leukocoria became more apparent as the cataract developed.
PHPV is a rare condition, essentially representing an arrest in the development of the eye with lack of resorption of the early tissues of the vitreous body. It is typically unilateral. It is associated with microphthalmia, cataract, retinal haemorrhages and detachment, refractive error, and amblyopia. It is one of the most common causes of infantile leukocoria and can be confused with retinoblastoma. To aid in the differentiation, retinoblastoma is usually not associated with cataract (unless iatrogenic) nor microphthalmia.
 Dr Margaret Lam BOptom UNSW Post Grad OcTherapy practises optometry at 1001 Optometry in Bondi Junction in Sydney and teaches at the School of Optometry at The University of New South Wales (UNSW) as an Adjunct Senior Lecturer. She is the immediate past National President of Optometry Australia.
Dr Margaret Lam BOptom UNSW Post Grad OcTherapy practises optometry at 1001 Optometry in Bondi Junction in Sydney and teaches at the School of Optometry at The University of New South Wales (UNSW) as an Adjunct Senior Lecturer. She is the immediate past National President of Optometry Australia.
 Dr Craig Donaldson AM MBBS FRANZCO FRACS completed the Sydney Eye Hospital training program before undertaking strabismus and paediatric ophthalmology fellowship training at the Hospital for Sick Children in Toronto, Canada. Dr Donaldson is a senior staff specialist at The Children’s Hospital at Westmead, a Visiting Medical Officer at Sydney Eye Hospital and Sydney Children’s Hospital, and head of the Strabismus and Paediatric Unit at Sydney Eye Hospital. From 2012–2018 he was president of the Australian and New Zealand Strabismus Society. He is RANZCO NSW State Branch Treasurer and a Federal Councillor. Dr Donaldson has authored numerous journal articles, book chapters and lectured extensively in Australia and internationally.
Dr Craig Donaldson AM MBBS FRANZCO FRACS completed the Sydney Eye Hospital training program before undertaking strabismus and paediatric ophthalmology fellowship training at the Hospital for Sick Children in Toronto, Canada. Dr Donaldson is a senior staff specialist at The Children’s Hospital at Westmead, a Visiting Medical Officer at Sydney Eye Hospital and Sydney Children’s Hospital, and head of the Strabismus and Paediatric Unit at Sydney Eye Hospital. From 2012–2018 he was president of the Australian and New Zealand Strabismus Society. He is RANZCO NSW State Branch Treasurer and a Federal Councillor. Dr Donaldson has authored numerous journal articles, book chapters and lectured extensively in Australia and internationally.
In 2019 he was awarded a Member of the Ordern of Australia (AM) for services to ophthalmology and medicine and the APAO prevention of blindness award in Asia.
References
- Liu YM, Xie P. The safety of orthokeratology – A systematic review. Eye Contact Lens. 2015 Dec 28;42(1):35–42. doi: 10.1097/ICL.0000000000000219.
- Sartor L, Hunter DS, Vo ML, Samarawickrama C. Benefits and risks of orthokeratology treatment: A systematic review and meta-analysis. Int Ophthalmol. 2024 Jun 21;44(1):239. doi: 10.1007/s10792-024-03175-w.
- Bullimore MA, Mirsayafov DS, Gorev VV, et al. pediatric microbial keratitis with overnight orthokeratology in Russia. Eye Contact Lens. 2021;47(7):420-425. doi: 10.1097/ICL.0000000000000801.
- Foreman J, Salim AT, Dirani M, et al. Association between digital smart device use and myopia: a systematic review and meta-analysis. Lancet Digit Health. 2021 Dec;3(12):e806-e818. doi: 10.1016/S2589-7500(21)00135-7.
- Wolffsohn JS, Jong M, Ohno-Matsui K, et al. IMI 2021 reports and digest – reflections on the implications for clinical practice. Invest Ophthalmol Vis Sci. 2021 Apr 28;62(5):1. doi: 10.1167/iovs.62.5.1.
- Dahlmann-Noor AH, Ghorbani-Mojarrad N, Young AL, et al. 2024 UK and Ireland modified Delphi consensus on myopia management in children and young people. Ophthalmic Physiol Opt. 2024 Nov;44(7):1368-1391. doi: 10.1111/opo.13381.