

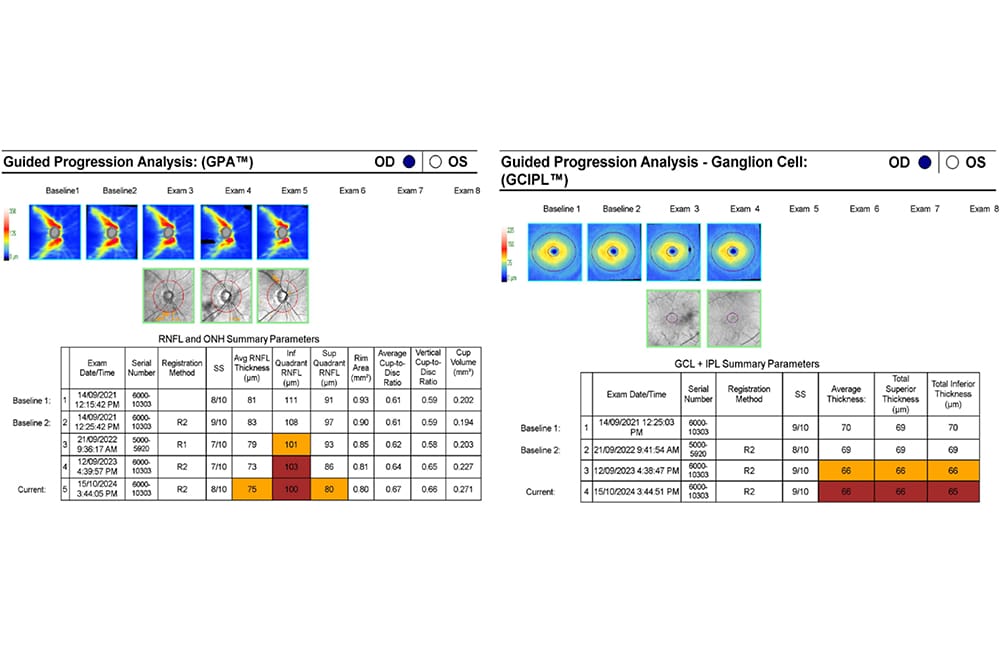
Figure 1. Guided progression analysis (RNFL and ganglion cell). Right eye results only are shown.
The landscape of glaucoma care in Australia faces significant challenges. With only 50% of people with glaucoma diagnosed and a mere 30% of these patients remaining compliant with monotherapy eye drops after two years, there is a pressing need for more effective care delivery models.1 Is collaborative care the answer?
The prevalence of glaucoma in Australia ranges from 2.2% to 3.0% of persons older than 50 years, with numbers predicted to reach 379,000 by 2025.2 This means the challenges that eye care professionals face in ensuring early identification of glaucoma suspects, and treatment non-compliance of those who are diagnosed with the disease, are likely to increase.
Fortunately, collaborative care models offer a proven solution. Collaborative care programmes have been developed and implemented in Australia that draw on successful international programmes, particularly the United Kingdom’s National Health Service (NHS) schemes, which have been operating since the mid-2000s. These Australian programmes demonstrate both improved patient outcomes and healthcare efficiencies.3
Collaborative care is a broad term that can have a wide range of definitions and interpretations, depending on the context. The World Health Organization states that “collaborative practice happens when multiple health workers from different professional backgrounds work together with patients, families, carers, and communities to deliver the highest quality of care”, and that “collaborative practice strengthens health systems and improves health outcomes”.4
There are a wide range of glaucoma collaborative care models and programmes currently operating in both community and hospital settings around Australia. While all have their advantages and disadvantages, it is generally agreed and specifically recognised in the Optometry Board of Australia Guidelines for the use of scheduled medicines5 that models of collaborative care will vary to suit the local environment.
Clear communication between practitioners is crucial to the success of any collaborative care arrangement
Current Australian Collaborative Programmes
Collaborative management of both glaucoma suspects and patients with glaucoma is a common part of routine community optometry and ophthalmology practice. This is typically done on an informal ad hoc basis, coordinated through referral letters and reports. However, more formalised and structured programmes are in place in some locations.
The nature of these community arrangements varies markedly, based on local circumstances such as the availability of imaging and functional testing, the presence of ophthalmology coverage in the region, and patient socioeconomic and demographic factors.
There are a number of formal glaucoma collaborative care programmes currently operating in public hospitals around the country, all working towards the same overarching goal of ensuring timely patient care given the current scarcity of public ophthalmology resources.
Current public hospital programmes fall into three broad structures, with notable variations between existing programmes in each of these categories:
- In-hospital optometry or orthoptic led clinics with either direct or indirect (telehealth or virtual) ophthalmology oversight,
- Public hospital affiliated external optometry clinics with either direct or indirect ophthalmology oversight, and
- Community optometry practice monitoring models, either through a discharge or with ongoing telehealth oversight.
A further model, not currently in place in the Australian public system but previously used and with potential to be re-introduced, involves optometrists working within a public hospital in a private capacity under a right to occupy arrangement.
Key Elements of a Glaucoma Specific Collaborative Programme
The diagnosis and ongoing management of glaucoma involves a wide range of clinical investigations with the key elements for ongoing monitoring being applanation intraocular pressures (IOPs), disc assessment including photography, visual field assessment, and optical coherence tomography (OCT). The nature of these investigations means that results are, in most cases, amenable to telehealth or virtual review. There are, however, several essential elements to a formalised glaucoma collaborative care model that need to be in place to ensure success. Initially, the patient’s consent to participate in shared care is required. The following chief elements then need to be established to tailor the programme to local requirements.
- Identify Suitable Patients for the Model of Care
There are a range of glaucoma staging and grading systems that have been published, however models are often based on the degree of visual field loss. This is typically done through utilisation of the Hodapp-Parish-Anderson criteria or variations thereof.6 Other considerations that need clarification, with regards to suitability for inclusion in specific collaborative care models, include secondary glaucomas, angle closure, monocular patients, and previous surgical treatment.7
- Identify Patient Physical Review Schedules
Glaucoma is typically reviewed on a six-monthly basis. Models of care can include ongoing physical reviews in the collaborative location with referral back to ophthalmology as required, or alternate reviews in the collaborative location and ophthalmology clinic.
- Determine Ophthalmology Review Method and Schedules
Ophthalmology oversight via telehealth or virtual review can be performed either on an as requested basis or at each visit, depending on the model requirements.
- Document Triggers for Ophthalmology Review
If the model of care does not include ophthalmology review (either physical or virtual) at each visit, it is important to determine clinical and patient criterion that indicate a need for further ophthalmology input. This may include elements such as IOPs not on target, structural or functional progression, or adverse drug responses.5
- Establish a Communication Platform
Clear communication between practitioners is crucial to the success of any collaborative care arrangement. There are multiple communication platforms and services currently available for sending routine reports and referrals with technology rapidly developing in this space. It is also important that a communication method is established for prompt and urgent physical referrals or virtual referrals if required. There should also be processes in place that enable feedback between practitioners.
- Ensure Clear Responsibilities
While collaborative care is typically set up to deal with a specific condition such as glaucoma, patients will inevitably have other eye care needs and co-morbidities. As a result, it is critical that it is clear to all parties who is responsible for each aspect of the patient’s care in a collaborative arrangement. Determining how and when to include the patient’s general medical practitioner and other related health practitioners in communications is a key part of coordinated patient-centric collaborative care. Similarly, determining who is responsible for follow-up of patients who miss appointments is a key factor in ensuring appropriate care, particularly in programmes involving public hospitals due to the added complication of a larger administration burden.
- Define Information to Include
Pro-forma templates to include in reports, referrals etc. provide consistency and assist with ease of review for all parties.
- Agree on a Funding Model
It is important that all parties are aware of revenue sources for the collaborative care model including the Medicare Benefits Schedule (MBS) and private fees. Patients obviously also need to be aware of any out-of-pocket costs, in particular if they are part of a public hospital collaborative programme.
- Establish a Feedback Loop
Quality control, consistency, and ongoing improvements are essential to ensuring a robust and successful collaborative programme. As a result, it is important to ensure that there is regular review of the model, as well as processes put in place to identify and learn from situations where there are differences in clinical or management opinions.
Barriers to Scalable Implementation
Despite evidence supporting the efficiency and efficacy of existing models of glaucoma collaborative care in Australia, the rollout of widespread formalised programmes in public hospitals across the country has been limited to date. There are many reasons for this, including: the nature and source of funding; the need for local governance and champions given the structure of public hospitals as well as fragmented information systems; and an increased administrative burden.3 These are currently being addressed through collaboration between peak bodies, documentation of existing programmes, industry input, and government advocacy.
Clinical Example: Westmead Hospital
The Community-Eye-Care (C-Eye-C) Programme at Westmead Hospital in Sydney is a service delivery model for those with, or at risk of developing glaucoma and/or diabetic retinopathy. It was developed after extensive consultation with a wide range of stakeholders and included an initial pilot programme and subsequent evaluation with published analysis and outcomes. The model of care is extensively outlined in a document produced by the Agency for Clinical Innovation.8
The programme currently includes two optometric practices in western Sydney – one in Blacktown and one in Parramatta. A total of 1,975 appointments were undertaken through this programme in the 2023 calendar year, freeing up a substantial amount of time and resources that could subsequently be allocated to servicing patients with more complex care needs within the hospital.
There are nine key elements specific to the C-Eye-C glaucoma programme operating model:
- Eligibility for inclusion includes new referrals for (non-urgent) glaucoma and existing patients who are glaucoma suspects or have mild or moderate disease, based on the model proposed by White and Goldberg in 2014.9
- Patients with glaucoma are typically reviewed every six months in the C-Eye-C optometrist’s practice.
- Every consultation is reviewed virtually by a Westmead ophthalmology fellow or consultant.
- Given this, triggers for returning to Westmead for physical review are based on the outcome of the virtual review.
- Microsoft Teams is used as a communication platform with reports sent as a PDF by the optometric practice to Westmead following each appointment.
- The optometric practice is responsible for all aspects of the patient’s ocular health, however collaboration with the patient’s regular community optometrist is used for many aspects of their care such as dry eye, refractive care etc. The C-Eye-C optometric practice also includes GPs in reports when the patient has diabetes or other systemic complications related to their ocular health.
- A pro-forma PDF report is used, with attached fundus photos, Cirrus OCT, and Humphrey visual field results. Other imaging is included if appropriate, including wide field retinal imaging, autofluorescence, anterior OCT, OCT-angiography, and gonioscopic photography.
- Funding of the community practices is through Medicare bulk-billing. The hospital uses ophthalmologists’ non-clinical time through opportunity cost to review the reports. A part-time administration officer is employed to manage the daily operations.
- A monthly report is sent to each of the community practices detailing any differences in outcomes following ophthalmology review.
Key Benefits of the Model
Case One
A 59-year-old male, Li Yu,* presented to the C-Eye-C associated optometrist for an annual review of bilateral ocular hypertension. He is also on the waiting list for an assessment for cataract surgery following a previous C-Eye-C assessment.
At this review, he had findings as shown in Table 1.

Table 1.
Cirrus OCT Guided Progression Analysis results (Figure 1) showed a downward trend in the right ganglion cell analysis (GCA) and retinal nerve fibre layer (RNFL) with no change in the left.
The marked increase in right IOP in conjunction with the suspicious structural findings prompted the C-Eye-C aligned optometrist to explain to the patient that treatment was recommended. Mr Yu was initially reluctant to undergo treatment, however following further discussion, an expedited review at Westmead to consider selective laser trabeculoplasty (SLT) was agreed upon.
Following ophthalmology review of the optometrist’s report via telehealth, Mr Yu was seen promptly at the Westmead Eye Clinic by the consultant glaucoma specialist. It was confirmed that Mr Yu had open angles but his eyes were behaving like occult pseudo-exfoliation. While SLT was a viable treatment option, given that Mr Yu was already waitlisted for a cataract assessment, the recommended course of management was expedited cataract surgery combined with minimally invasive glaucoma surgery. The Hydrus was selected to mitigate the risk of a post-surgical IOP spike.
This case illustrates the way in which collaborative care involving telehealth can be used to expedite care where clinically appropriate, helping to facilitate the best possible patient outcome.
Case Two
An 84-year-old female, Emma Carmichael,* was commenced on Xalatan treatment at Westmead Hospital for pseudoexfoliation syndrome in the right eye and pseudoexfoliation glaucoma in the left. Pre-treatment IOPs were 30 mmHg in both eyes. She was transferred to the C-Eye-C programme for six monthly reviews once stable.
At her first C-Eye-C review in March 2024, Ms Carmichael was using eye drops and reported excellent compliance with no notable adverse effects. Her initial testing results were as shown in Table 2.

Table 2
At a subsequent review in the C-Eye-C programme six months later, the IOPs had increased to 30 mmHg in each eye. While no structural progression was evident on disc photos or OCT, visual field testing showed repeatable functional progression with a widening of the previously recorded inferior arcuate defect (Figure 2).

Figure 2. SITA Faster 24-2 visual field for Ms Carmichael showing the initial and six- month follow-up results.
Based on the increase in IOP and functional progression, and given no contra-indications, the C-Eye-C optometrist prescribed Xalacom to be used once daily in both eyes and arranged for review six weeks later. At this appointment, the IOP had reduced to 19 mmHg (OD) and 21 mmHg (OS). Results were reviewed via telehealth by a glaucoma consultant at Westmead Hospital with a subsequent review scheduled for six months at the C-Eye-C associated optometrist.
This case illustrates the public resourcing benefit of collaboration between therapeutically qualified optometrists and ophthalmology. Minimising hospital visits through community collaborative care programmes with telehealth oversight from ophthalmology helps to ensure public hospital ophthalmology services are more readily available to those requiring a higher level of intervention or care.
*Patient names changed for anonymity.
Michael Yapp BOptom(Hons) MOptom GradCertOcTher FAAO is the Head of Clinical Operations at the Centre for Eye Health in Sydney.
Dr John Yek BBmed MCHD FRANZCO is a glaucoma specialist practising ophthalmology out of PersonalEyes in Sydney and at Westmead Hospital.
Dr Yen Cheng MMed(OphthSc) MBBS BMedSc(Hons) is a Clinical Glaucoma Fellow at Westmead Hospital.
Andrew White BMedSci(Hons) MBBS PhD FRANZCO is a Clinical Associate Professor at the University of Sydney and Conjoint Associate Professor at the School of Optometry and Vision Sciences, University of New South Wales. He is the Co-Chair, Agency for Clinical Innovation: Ophthalmology Network Governing Body; and the Head of both the Department of Ophthalmology at Westmead Hospital and the Centre for Vision Research at the Westmead Institute for Medical Research. Assoc Prof White is also the Director of the Community Eye Care Centre in western Sydney and a Director of PersonalEyes.
References
- Kell M. Glaucoma management: Overcoming the challenges, mivision 2017 Mar (121); 24-28.
- Keel S, Xie J, Dirani M, et al. Prevalence of glaucoma in the Australian National Eye Health Survey. Br J Ophthalmol. 2019;103(2):191-195. doi: 10.1136/bjophthalmol-2017-311786.
- Ford BK, Angell B, Liu H, et al. Implementation and scalability of shared care models for chronic eye disease: A realist assessment informed by health system stakeholders in Finland, the United Kingdom, and Australia. Eye. 2023; 37, 2934-2945. doi: 10.1038/s41433-023-02444-9.
- World Health Organization. Framework for action on interprofessional education and collaborative practice. Available at: iris.who.int/bitstream/handle/10665/70185/WHO_HRH_HPN_10.3_eng.pdf?sequence=1 [accessed Dec 2024].
- Optometry Board of Australia, Optometry guidelines on for the use of scheduled medicines. Available at: optometryboard.gov.au/Policies-Codes-Guidelines.aspx [accessed Dec 2024].
- Hodapp E, Parrish RK II, Anderson DR. Clinical decisions in glaucoma. St Louis: The CV Mosby Co; 1993; 52-61. Available at: api.semanticscholar.org/CorpusID:56639770 [accessed Dec 2024].
- RANZCO, Clinical practice guidelines for the collaborative care of glaucoma patients and suspects by ophthalmologists and optometrists in Australia, 2019. Available at ranzco.edu/wp-content/uploads/2018/11/Guidelines-for-the-Collaborative-Care-of-Glaucoma-Patients.pdf [accessed Dec 2024].
- Agency for Clinical Innovation Ophthalmology Network, Community Eye Care Model for Glaucoma and Diabetic Retinopathy. Available at: aci.health.nsw.gov.au/__data/assets/pdf_file/0006/501675/ACI-Opthal-c-eye-c-model-of-care.pdf [accessed Dec 2024].
- White A, Goldberg I; Australian and New Zealand Glaucoma Interest Group and the Royal Australian and New Zealand College of Ophthalmologists. Guidelines for the collaborative care of glaucoma patients and suspects by ophthalmologists and optometrists in Australia. Clin Exp Ophthalmol. 2014 Mar;42(2):107-17. doi: 10.1111/ceo.12270.





