

Until recently there has been no treatment available for patients with geographic atrophy (GA), which can have a significant impact on the quality of life for patients. However, this changed earlier this year with the Therapeutic Goods Administration (TGA) approving the first intravitreal injection for GA treatment, and more emerging therapies in the pipeline.
Geographic atrophy (GA) is an advanced form of age-related macular degeneration (AMD) that can lead to irreversible central blindness. The prevalence of GA is around 0.3–0.5% globally, with an age-related increase, where one in five people aged 85 and above have GA in at least one eye.1 Its prevalence varies by region and ethnicity, with higher rates among white people.
GA has a variable rate of progression influenced by several factors including multimodality, foveal involvement, and the pattern of autofluorescence. Its expansion is often asymmetric with slower involvement of the fovea.
Pathophysiology
Geographic atrophy is a chronic progressive degeneration with the loss of retinal pigment epithelium (RPE) and photoreceptors alongside damage to the choriocapillaris. Due to the nature of retinal destruction, GA results in central scotomas and permanent visual loss. The pathophysiology of GA is multi-faceted, with current theories centring on intrinsic and extrinsic oxidative stress, chronic inflammation, and complement cascade dysfunction.
Many of these processes are progressive with a positive feedback loop, leading to a cascade of destructive reactions, resulting in retinal atrophy. Physiological damage to the eye can occur due to a variety of causes. Oxidative stress can be intrinsic in nature, due to the highly metabolic nature of photoreceptors in the retina. It can also be extrinsic in nature, due to environmental toxins such as cigarette smoking. Other risk factors include age, family history, hypertension, hypercholesterolaemia, and low choroidal blood flow. All these factors can impair mitochondrial function in RPE, generating increased reactive oxygen species and activating apoptotic pathways in the tissue. The resultant defects in the RPE lead to the accumulation and formation of drusen deposits in the retina.
The presence of drusen is one of the clinical hallmarks of AMD. While drusen are not the direct cause of AMD, their size classification is integral in the staging of AMD as their presence prognosticates the risks of AMD progression. Drusen are composed of host body cells and their products, lipids and lipoproteins, but can also be accompanied by the presence of other molecules, such as advanced glycation end-products generated from oxidative stress. These deposits lie between the RPE and Bruch’s membrane, precipitating a chronic inflammatory state. The exact pathophysiology for drusen formation and accumulation is not well understood, but it is known that the complement pathway and cascade play a critical role in its regulation such as complements C3, C5, complement factor H (CFH), and complement factor I (CFI). Numerous studies have shown that genetic alterations to C3 and CFH can reduce the inflammatory inactivation response typically generated by host cells.2,3 CFH Y402H is a variant that has been shown to account for nearly half of all AMD risk,4 while CFH R1210C and C3 K155Q have been shown to restrict the inhibitory interaction between CFH and C3b.5 This correlates with the elevated levels of complement activation products (C3, C5, CFH) found in drusen, Bruch’s membrane, and choriocapillaris in patients with AMD. In fact, drusen production is also thought to be upregulated by the presence of complement.
Studies have shown that reading rate in GA patients can decrease by over 50% from baseline within two years
Clinical Examination
While best corrected visual acuity (BCVA) is an integral part of any ophthalmic examination and is easily performed in the clinic, it is well known that visual acuity is not an optimal clinical marker to assess and monitor GA. This is because studies have shown that the fovea may initially be spared in GA, with visual acuity remaining largely unchanged until subfoveal involvement occurs. This can result in rapid deterioration of central vision within one to two years. Therefore, alternative markers of vision, such as contrast sensitivity and reading ability, are superior early markers of loss in visual function. Studies have shown that reading rate in GA patients can decrease by over 50% from baseline within two years, while patients who only had drusen deposits experienced a 10% decline.3 Low luminance visual acuity (LLVA) can be contrasted with BCVA to develop a low-luminance deficit score, which helps expose weaknesses in contrast sensitivity in low light conditions, a prognostic factor for future loss of acuity in GA.
Other ancillary tests that can be used to assess and monitor GA include an Amsler grid and microperimetry. An Amsler grid can be more reliable than BCVA as it is an easy-to-use self-monitoring tool to identify visual field distortions and scotomas across the visual field. Microperimetry is another tool that can provide functional assessment of vision quality in patients with GA. It combines perimetry and retinal imaging to allow direct mapping of functional vision and anatomical function in the area of interest. This allows clinicians to monitor changes in GA lesion size and monitor the rates at which these changes occur with extreme accuracy and objectivity. However, microperimetry is rarely used in the clinical setting and is largely used in an academic setting.
Multimodal Imaging
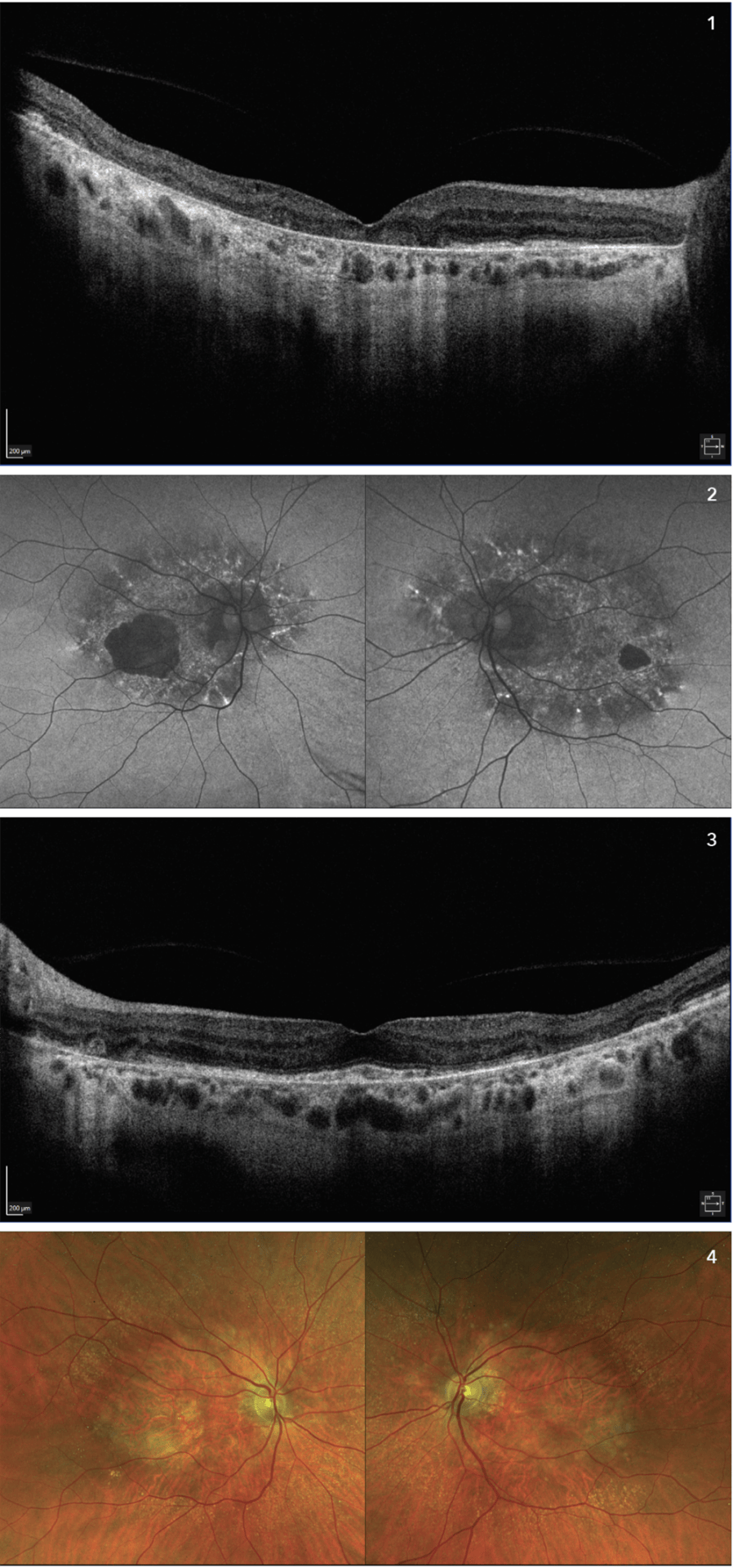
Figures 1–4. Multimodal imaging features of geographic atrophy. Right eye shows extensive GA with foveal
involvement, left eye shows extrafoveal atrophy.
Currently, there is a wide variety of fundal imaging techniques available, including colour fundus photography (CFP), fundus autofluorescence (FAF), and optical coherence tomography (OCT). CFP was the original standard for assessing GA. It allows for assessment of RPE hypopigmentation, identification of drusen and lipofuscin deposits, and qualitative assessment of choroidal vessels. However, it is unable to quantitatively assess and monitor changes in lesions over time, or differentiate simple drusen deposits from lesions with stronger associations with GA. It is also extremely difficult to determine the characteristics of lesions deep in the retina. Therefore, other imaging modalities, such as FAF and OCT have become more prominent.
FAF is the current gold standard for assessing GA in clinical and research settings. This modality relies on the interaction between the short wavelengths of light and the intrinsic fluorophore and lipofuscin in the RPE and photoreceptors. Hypoautofluorescence is observed in areas of retinal atrophy found in GA, while hyperautofluoresence is observed in ‘sick’ areas of the retina where there is an accumulation of lipofuscin. This is the result of RPE and photoreceptor migration, and usually occurs in the periphery of the atrophic areas where progression is most likely.
OCT uses infrared light to construct a cross-sectional assessment of the ultrastructures in the retina using differing reflectivity of the retinal layers. Its development has been pivotal in the treatment paradigm of many retinal diseases as it allows the detection of retinal changes that were previously difficult to detect on clinical examination, such as the presence of intra- and sub-retinal fluids. This has allowed us to refine the atrophy classification, now most commonly based on the ‘Classification of Atrophy Meetings’ (CAM) definition.6 These are complete RPE and outer retinal atrophy (cRORA), incomplete RPE and outer retinal atrophy (iRORA), complete outer retinal atrophy (cORA), and incomplete outer retinal atrophy (iORA). This classification has clinical implications as more significant tissue loss, such as cRORA, indicates a worse prognosis with quicker progression and a higher risk of significant vision loss.
With the increasing development and use of deep learning and artificial intelligence algorithms, recent studies have investigated whether these can aid in diagnosis and classification of GA. Treder et al. managed to develop an algorithm with 96% validation accuracy comparing GA and healthy patients, and with 77% accuracy in differentiating diffuse-trickling pattern GA from other patterns.7 Although only 20 untrained images were used for testing (compared to 200 for training), these results still demonstrate the ability to improve our use of current imaging modalities. This is reflected in a review from Arslan et al. that looked at 27 artificial intelligence studies for GA. With sensitivities ranging from 0.47 to 0.98 and specificities from 0.73 to 0.99, it’s clear that although its use is in novel stages, the role of artificial intelligence in assessment of ocular pathology has significant potential.8
Treatment
Previously, there was no treatment available for GA, except for lifestyle modifications such as smoking cessation and a diet rich in leafy green vegetables. This is a devastating, chronic disease with variable rates of progression and poor prognosis. However, intravitreal pegcetacoplan injection (Syfovre) has recently been approved by the TGA for every-other-month treatment (EOM) in patients with an intact fovea where central vision is threatened by expanding GA lesion size. Another medication, avacincaptad pegol (Izervay) has also obtained Food and Drug Administration (FDA) approval in the US.
intravitreal pegcetacoplan injection (Syfovre) has recently been approved by the TGA for every-other-month treatment (EOM) in patients with an intact fovea where central vision is threatened by expanding GA lesion size
Anticomplement Therapies
Dysregulation of the complement pathway causes chronic inflammation and cell death in key components of the retina including photoreceptors, retinal pigment epithelium, and underlying choriocapillaris. By blocking the recruitment of inflammasomes and eventual formation of the membrane attack complex (MAC), drugs such as pegcetacoplan and avacincaptad pegol may restore the complement system to equilibrium and preserve retina health.9
Pegcetacoplan is a modified pegylated peptide that inhibits C3, a key factor in which all complement pathways – classical, alternative and lectin – converge. Three randomised controlled trials used FAF to demonstrate monthly and EOM intravitreal pegcetacoplan reduction of GA lesion growth.
The Phase 2 FILLY study showed a statistically significant reduction of 29% (p=0.008) and 20% (p=0.067) in the growth rate of GA in the monthly and EOM arm compared to patients with sham treatment after 12 months.9 However, 22.4% of patients (n=246) either exited early (n=28) or discontinued treatment (n=27) due to adverse effects including increased frequency of exudative AMD (20.9% and 8.9% in monthly and EOM group respectively, compared to sham). As these patients had less time for lesions to grow, the lesion size recorded would likely be less than if observations were made at 12 months, inflating treatment efficacy.
The OAKS and DERBY Phase 3 studies further assessed the risks and benefits of pegcetacoplan.10 The OAKS trial demonstrated a statistically significant reduction in lesion growth compared to sham of 21% (p=0.0004) and 16% (p=0.0055) in monthly and EOM at 12 months, and 22% (p<0.0001) and 18% (p=0.0002) for monthly and EOM respectively at 24 months. The DERBY trial did not reach a statistically significant reduction at 12 months (12%; p=0.0528 and 11%; p=0.0750 for monthly and EOM respectively) but achieved this by 24 months (19%; p=0.0004 and 16%; p=0.0030 for monthly and EOM respectively). A combined sub-analysis of both trials identified greater reduction in GA lesion growth in participants with non-subfoveal lesions (26% and 22% for monthly and EOM respectively) compared to sub-foveal lesions (19% and 16% for monthly and EOM respectively).9 Although generally well tolerated in both studies, with low rates of endophthalmitis and intraocular inflammation, new-onset choroidal neovascularisation was reported in OAKS (11%, 8%, and 2% in monthly, EOM and sham) and DERBY (13%, 6% and 4% in monthly, EOM, and sham). Unlike FILLY, these patients were administered anti-vascular endothelial growth factor treatment and continued in the study, better estimating the side effect profile of pegcetacoplan. Furthermore, more studies are required to investigate outcomes such as BCVA, maximum reading speed, and functional reading independence-index to demonstrate its functional benefits in addition to anatomical gains.
Avacincaptad pegol (ACP) is another anticomplement treatment that has gained FDA approval. ACP is a pegylated ribonucleic acid aptamer that binds to C5, inhibiting cleavage into C5a and C5b. C5b is responsible for MAC precipitation in Bruch’s membrane and choriocapillaris that contributes to cell death. As C5 is a terminal component of the complement cascade, ACP may preserve upstream defence mechanisms including C3a which may be crucial in modulating inflammation.9
The efficacy and tolerability of ACP was best evaluated in two double-masked clinical trials (GATHER1 and GATHER2).11 Unlike the OAKS and DERBY trials, the Phase 2 GATHER1 trial included only patients with non-subfoveal GA lesions.9,11 When participants were administered monthly 2 mg and 4 mg over 12 months, there was a significant reduction of 27% (p=0.0072) and 28% (p=0.0051) respectively, compared to sham. The subsequent Phase 3 GATHER2 trial yielded a lower GA growth reduction of 14% (p=0.0064) between 2 mg and sham monthly injections over 12 months.12 The adverse event analysis of both trials demonstrated minimal adverse events and cases of inflammation. Like pegcetacoplan, the ACP 2 mg treatment arm displayed greater incidence of macular neovascularisation. This may be a consequence of complement inhibition causing inefficient removal of damaged cells that secrete vascular endothelial growth factor. ACP approval by the FDA was also purely based on anatomic endpoints, with further studies needed to demonstrate its functional benefit.
Oral Antioxidants
In 2001, the AREDS oral supplementation with vitamins C and E, beta carotene, and zinc plus copper demonstrated reduced risk of developing advanced AMD by 25% at five years for high-risk patients having extensive intermediate drusen, large drusen, non-central geographic atrophy (GA), or vision loss due to AMD in one eye.13 The later AREDS2 replaced beta-carotene with lutein/zeaxanthin as beta-carotene was associated with a near two-fold increased risk of lung cancer.13 As such, AREDS supplements are recommended in two groups of patients; patients with intermediate AMD to slow the progress to late AMD, or patients with late AMD in one eye, to slow the progression of AMD in the other eye. The AREDS supplement was not initially recommended for patients with bilateral severe GA.
However, a recent post-hoc analysis in 2025 evaluated the efficacy of AREDS and AREDS2 supplements in halting GA in terms of area-based progression (i.e., change in GA area over time) and proximity-based progression (i.e., change in GA proximity to macular centre-point over time).14 The AREDS study showed the rate of GA progression to the central macula was significantly slower in those randomised to antioxidants versus no antioxidants at 50.7 μm/year and 72.9 μm/year respectively (p=0.012). This treatment effect was similarly demonstrated in the AREDS2 study where GA progression toward the central macula was significantly slower in eyes randomised to lutein/zeaxanthin versus no lutein/zeaxanthin, at 84.5 μm/year and 105.3 μm/year respectively (p=0.017).
As for area-based progression, no significant difference was observed between those randomised to antioxidants versus no antioxidants, as well as between zinc versus no zinc in the AREDS group. However, when the area-based analysis was repeated using a smaller subgroup of participants with incident non-central GA, a significantly slower progression rate was demonstrated for those with antioxidants versus without, at 0.258 mm/year and 0.379 mm/year respectively (p=0.007). The suggested explanation for the differential efficacy in the prevalent and incident cohort was that area-based efficacy would be preferentially detected in eyes with early non-central GA where any progression into the central macula would affect the GA area metric.
Overall, this post-hoc analysis suggested oral micronutrient supplement delays the progression of GA toward the central macula and augments the natural phenomenon of ‘foveal sparing’. Preserving a peripheral configuration of GA would likely be valuable in preserving visual acuity in the long term. However, this study is limited as no data is available to allow a direct comparison between those randomised to the current AREDS2 supplements versus placebo as all study participants in AREDS2 took the vitamins C and E doses used in AREDS. A prospective study specifically investigating its effect on GA is necessary to draw more conclusive results. If proven, oral supplements offer unique advantages over alternative invasive treatments given their favourable cost and the lack of complications associated with intravitreal injections.
Overall, this post-hoc analysis suggested oral micronutrient supplement delays the progression of GA toward the central macula and augments the natural phenomenon of ‘foveal sparing’
Emerging Therapies
There are multiple other emerging therapies that have shown potential to prevent or slow the progression of GA, and to preserve and restore vision. These emerging strategies include other anti-complement therapies, ocular gene therapies, cell-based treatment options, and neuroprotective agents.15
The management of geographic atrophy remains a challenge for eye care professionals due to its severe and irreversible nature. Fortunately, this is a rapidly evolving area with newly approved medication such as peacetacoplan as well as other emerging therapies, offering new treatment options for a previously untreatable condition. However, these new treatment options bring about other challenges including patient selection, and treatment side effects such as conversion to neovascular AMD and uveitis, as well as optimal treatment interval and duration. Therefore, further research and real-world data will be necessary to navigate this newfound territory to provide optimal patient outcomes.
To earn your CPD hours from this article visit: mieducation.com/2025/05/geographic-atrophy-shifting-the-treatment-goalposts/.

Dr Christopher Go
Dr Christopher Go is a Sydney-based fellowships-trained vitreoretinal surgeon with extensive experience in medical and surgical management of retinal and macular disorders. He has completed four clinical retinal fellowships in Liverpool UK, Hong Kong, Melbourne, and Taiwan.
Dr Go is an examiner for the Royal Australian and New Zealand College of Ophthalmologists (RANZCO), Adjunct Associate Lecturer at the University of New South Wales, and Conjoint Clinical Lecturer at Sydney University. He practises with Vision Eye Institute.

Dr Alexander Maloof
Dr Alexander Maloof is a junior doctor in his first post-graduate year of clinical medicine with a keen interest in ophthalmic research and practice. Dr Maloof graduated with first class honours from the University of New South Wales, and hopes to improve his well-roundedness as a clinician by continuing to engage with both surgical and medical research while concurrently undertaking full-time clinical work at Prince of Wales Hospital in Sydney.
References
- Schmitz-Valckenberg S, Sahel J-A, Danis R, et al. Natural history of geographic atrophy progression secondary to age-related macular degeneration (Geographic Atrophy Progression Study). Ophthalmology. 2016;123(2):361-368. doi: 10.1016/j.ophtha.2015.09.036.
- Boyer DS, Schmidt-Erfurth U, Brittain C, et al. The pathophysiology of geographic atrophy secondary to age-related macular degeneration and the complement pathway as a therapeutic target. Retina. 2017;37(5):819-835. doi: 10.1097/IAE.0000000000001392.
- Rajanala K, Dotiwala F, Upadhyay A. Geographic atrophy: pathophysiology and current therapeutic strategies. Front Ophthalmol (Lausanne). 2023;3:1327883. doi: 10.3389/fopht.2023.1327883.
- Schramm EC, Clark SJ, Atkinson JP, et al. Genetic variants in the complement system predisposing to age-related macular degeneration: a review. Mol Immunol. 2014;61(2):118-125. doi: 10.1016/j.molimm.2014.06.032.
- Bakri SJ, Bektas M, Khan S, et al. Geographic atrophy: Mechanism of disease, pathophysiology, and role of the complement system. J Manag Care Spec Pharm. 2023;29(5-a Suppl):S2-S11. doi: 10.18553/jmcp.2023.29.5-a.s2.
- Sadda SR, Guymer R, Holz FG, et al. Consensus definition for atrophy associated with age-related macular degeneration on OCT: classification of atrophy report 3. Ophthalmology. 2018;125(4):537-548. doi: 10.1016/j.ophtha.2018.10.038.
- Treder M, Lauermann JL, Eter N. Deep learning-based detection and classification of geographic atrophy using a deep convolutional neural network classifier. Graefes Arch Clin Exp Ophthalmol. 2018;256:2053-2060. doi: 10.1007/s00417-018-4098-2.
- Arslan J, Samarasinghe G, Benke KK, et al. Artificial intelligence algorithms for analysis of geographic atrophy: a review and evaluation. Transl Vis Sci Technol. 2020;9(2):57-57. doi: 10.1167/tvst.9.2.57.
- Flaxel CJ, Adelman RA, Bailey ST, et al. Age-related macular degeneration preferred practice pattern. Ophthalmology. 2020;127(1):P1-P65. doi: 10.1016/j.ophtha.2020.06.047.
- Goldberg R, Heier JS, Wykoff CC, et al. Efficacy of intravitreal pegcetacoplan in patients with geographic atrophy (GA): 12-month results from the phase 3 OAKS and DERBY studies. Investigative Ophthalmology & Visual Science. 2022;63(7):1500-1500.
- Patel SS, Lally DR, Hsu J, et al. Avacincaptad pegol for geographic atrophy secondary to age-related macular degeneration: 18-month findings from the GATHER1 trial. Eye. 2023;37(17):3551-3557. doi: 10.1038/s41433-023-02497-w.
- Khanani AM, Patel SS, Staurenghi G, et al. Efficacy and safety of avacincaptad pegol in patients with geographic atrophy (GATHER2): 12-month results from a randomised, double-masked, phase 3 trial. Lancet. 2023;402(10411):1449-1458. doi: 10.1016/S0140-6736(23)01583-0.
- Chew EY, Clemons TE, Agrón E, et al. Long-term effects of vitamins C and E, β-carotene, and zinc on age-related macular degeneration: AREDS report no. 35. Ophthalmology. 2013;120(8):1604-1611. e4. doi: 10.1016/j.ophtha.2016.10.026.
- Chew EY, Clemons TE, Agrón E, et al. Long-term outcomes of adding lutein/zeaxanthin and ω-3 fatty acids to the AREDS supplements on age-related macular degeneration progression: AREDS2 report 28. JAMA Ophthalmol. 2022;140(7):692-698. doi: 10.1001/jamaophthalmol.2022.1640.
- de Oliveira Figueiredo EC, Bucolo C, Eandi CM. Therapeutic innovations for geographic atrophy: A promising horizon. Curr Opin Pharmacol. 2024;78:102484. doi: 10.1016/j.coph.2024.102484.





