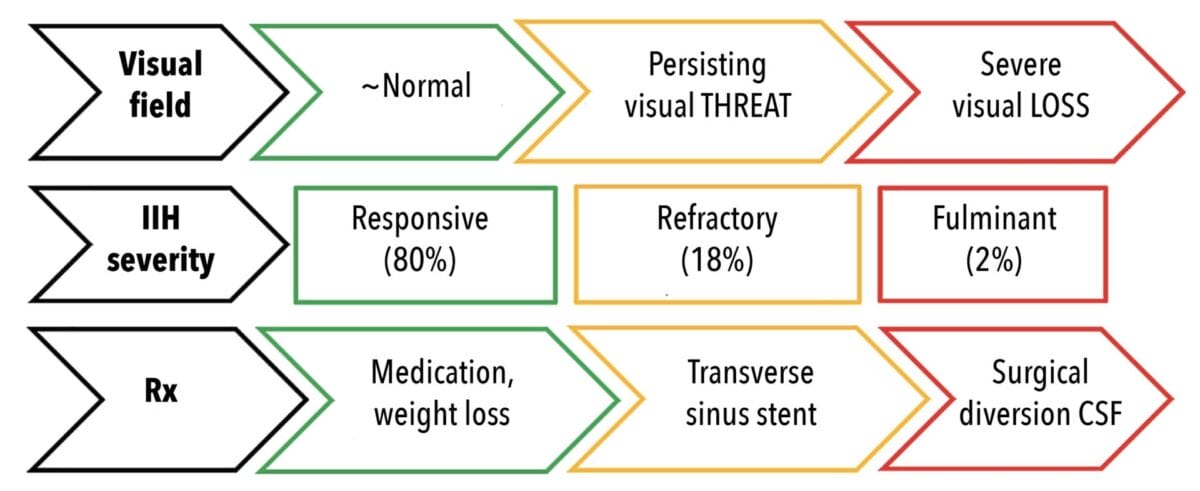
Figure 1. Treatment escalation in IIH is guided by the degree of visual threat evident in the visual fields.
Weight loss is considered a cornerstone of treatment for idiopathic intracranial hypertension (IIH), with the large majority of IIH patients being overweight or obese. At first glance, the advent of semaglutide and similar medications is therefore a major step forward in IIH management. However the new medications carry risks along with multiple benefits, and not all IIH patients respond to weight loss. Some are not even overweight. The role of weight loss in IIH management therefore deserves nuanced consideration.
LEARNING OBJECTIVES
On completion of this CPD activity, participants should:
- Have a refreshed understanding of the principles of diagnosis in idiopathic intracranial hypertension,
- Understand why weight loss assists IIH management in most patients, and
- Be aware of the benefits and risks of GLP-1s for weight loss.
IIH is by far the most common neuro-ophthalmic presentation, accounting in my own practice for almost half of all neuro-ophthalmic consultations. It is the commonest cause of papilloedema,1 namely optic nerve head swelling due to raised pressure in the cerebral spinal fluid (CSF) between the optic nerve and its meningeal sheath.
The stereotypic presentation of a young woman with increased body mass index (BMI), headache, pulsatile tinnitus (‘whooshing’), and papilloedema with no other cause is being seen much more frequently as obesity continues to increase.2 Diagnosis is dealt with at length in the literature,3 and practical diagnostic points are summarised in Table 1. Since papilloedema can eventually cause permanent visual loss,4 IIH treatment aims both to protect vision and to relieve headache, which is the most troublesome aspect of the disease for around half of patients.5

Table 1. Practical points in IIH diagnosis. Abbreviations: OCT – optical coherence tomography; PHOMS – peripapillary hyperreflective ovoid mass-like structures; RNFL – retinal nerve fibre layer; CT – computed tomography; MR – magnetic resonance; CFS – cerebral spinal fluid.
Once the diagnosis is established, the urgency of treatment depends on the degree of visual threat evident in the visual fields. The worse the emerging or established field loss, the more aggressive the intervention (Figure 1, top).
Fortunately, 80% of IIH patients have essentially normal visual fields, other than perhaps mild blind spot enlargement.6 This group generally responds to non-procedural treatment, namely a combination of weight loss and medications that suppress CSF secretion (Diamox/acetazolamide and Topamax/topiramate).
Weight Loss Benefits Many IIH Patients
Why might weight loss assist IIH management? Papilloedema results from increased CSF pressure, and since CSF constantly forms and drains away, anything reducing CSF drainage can cause papilloedema. CSF eventually flows into large veins at the base of the brain, the transverse venous sinuses (Figure 2), so stenosis of the sinuses can obstruct CSF drainage. It is now recognised that transverse sinus stenosis is indeed a major factor in IIH causation, independent of weight.10 Stenosis reduces drainage of venous blood from the head, causing cerebral venous hypertension, which only narrows the sinuses further (Figure 2).

Figure 2. The adverse feedback loop created by transverse sinus stenosis.
However transverse sinus stenosis is not the only factor that can cause cerebral venous hypertension, and therefore papilloedema. Obesity can also reduce venous drainage from the head: intra-abdominal fat increases the intra-abdominal pressure, which is then transmitted to the cerebral venous system.11 Thus it is not only the metabolic changes seen in obesity12 that alter CSF pressure regulation in IIH. Concerningly, the greater the BMI, the worse the headache13 and papilloedema severity.14
It follows that weight loss should lower intracranial pressure, and the IIH Weight Trial has shown this be true.15 Clinical remission of IIH can be achieved in many patients with an average weight loss of 10.5 kg.16 However it is not news that those with increased BMI struggle to lose weight and to maintain that loss – dieters may even regain more weight than they initially lost.17 Weight reduction is especially challenging in polycystic ovary syndrome (PCOS), a common co-morbidity in IIH.18 The advent of the glucagon-like peptide-1 receptor agonist (GLP-1) drugs typified by semaglutide has therefore opened up welcome new possibilities.
GLP-1s in IIH
GLP-1s are synthetic, longer-lasting versions of naturally occurring but very short-lived gut hormones. Originally developed to improve diabetic control, GLP-1s are now even more widely used for weight loss. Reductions of up to 20% of body weight are seen with semaglutide,19 with tirzepatide generating even more weight loss in other studies.20 There are numerous mechanisms (Figure 3) by which weight loss is achieved:
- increased satiety due to slowed gastric emptying,
- central reduction of appetite and food cravings – ‘turning off the food noise’,
- reduced blood sugar and lipids due to increased insulin secretion, and
- spontaneously improved food choices.
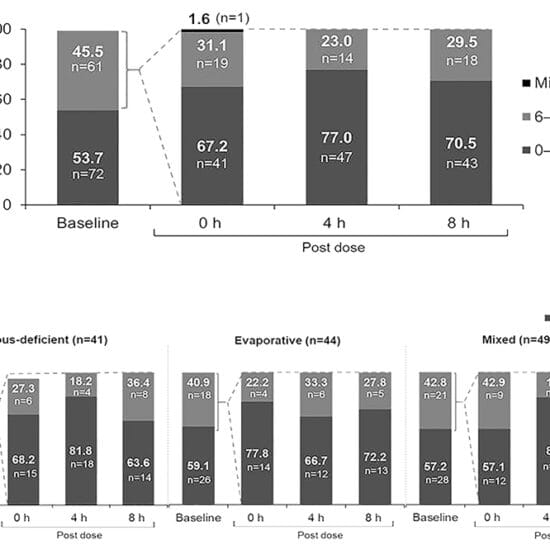
There is also a striking direct effect on CSF pressure (normal <25 cm CSF), at least for exenatide (Byetta), the first drug in class. It reduces CSF secretion and pressure at 2.5 hours, 24 hours, and 12 weeks by some 6 cm CSF,21 and perhaps this direct effect on pressure will prove to be shared by other GLP-1s. It is interesting that metformin, another medication type that reduces blood sugar, also seems to have a benefit in IIH beyond weight loss.22
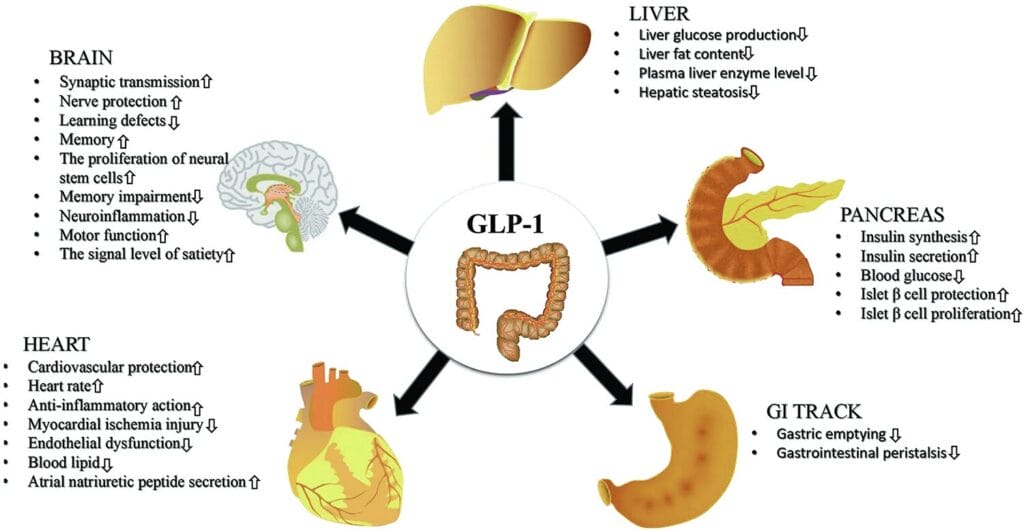
Figure 3. GLP-1s exert influence in multiple sites throughout the body (Image from Zhao X, Wang M, Zhang Y, et al. GLP-1 receptor agonists: Beyond their pancreatic effects. Front. Endocrinol. 12: 721135. doi: 10.3389/fendo.2021.721135. Reproduced under Creative Commons Attribution Licence.)
GLP-1 Benefits Beyond Weight Loss
GLP-1s help IIH patients in other ways. The associated weight loss dramatically improves obstructive sleep apnea;23 perhaps by reducing hypercapnia and its attendant elevation of intracranial pressure, lessened sleep apnea reduces the feedback loop described in Figure 2. GLP-1s are also known to be neuroprotective for the optic nerve. They reduce glaucoma in non-diabetics by an astounding 58% at five years compared to other weight loss drugs,24 and perhaps this neuroprotection will be shown to extend to papilloedema also. Other remarkable neuroprotective outcomes from GLP-1 use (compared to other medications that lower glucose) are reduction of both dry and wet age-related macular degeneration (AMD)25 and dementia26 by around 30%. On average, GLP1-s are discontinued five times less than the IIH drug Diamox.27 They also offer major cardiovascular health benefits to obese patients, with rates of stroke and heart attack decreased by some 20% in non-diabetics.28
GLP-1 Uptake and Cost
GLP-1 prescribing in Australia (Table 2) has increased tenfold since semaglutide was first approved here in 2020.

Table 2. Prescribing indications for the most commonly used GLP-1s.
It is estimated that 1.8% of Australians are using GLP-1s, with one third accessing them privately.29 It is not known how many patients receiving private scripts are seeking health benefits as opposed to ‘the body beautiful’. However it is clear that uptake by diabetics is increasing, with Pharmaceutical Benefits Scheme (PBS) scripts for Ozempic doubling in a year to reach 2.4 million in 2023–24.30
Private scripts are expensive. Costs start at around AU$260 for four weekly injections and rise as the dose increases. Tirzepatide is more expensive than semaglutide, costing as much as $600 for four injections at maximum strength. This does limit affordability for many IIH patients.
GLP-1 Side-effects and Contraindications
Due to gastric slowing, side-effects of GLP-1s include nausea and vomiting, reflux, and constipation. To minimise these gut symptoms, the dose is built up gradually each month, while the delay in gastric emptying requires a 24-hour clear-fluid diet prior to standard fasting for general anaesthesia.31 Hypoglycemia is a risk in diabetics on other medications for blood sugar control. Marked weight loss can age facial appearance through the loss of subcutaneous plumping – ‘Ozempic face’. Limited food intake may cause protein deficiency, leading to muscle loss or sarcopenia, especially in older diabetic patients.32 Discontinuation rates for GLP-1s range from 5 to 20%, due to side effects27 and non-responsiveness.33
GLP-1s are contraindicated in patients with significant renal impairment and can cause renal calculi34 and liver damage.35 There is insufficient data as yet to assess the safety of GLP-1s in pregnancy,36 so this too is a contraindication. There is mixed literature regarding increased risk of thyroid cancer37 and pancreatitis.38 A slightly increased rate of suicidal ideation has been reported,39 possibly because the central effect on the brain’s reward systems can cause anhedonia, a lack of interest and enjoyment in life.40
GLP-1s and NAION
Patients with significant diabetic retinopathy may experience its progression due to rapid tightening of glycemic control. However non-arteritic ischemic optic neuropathy (NAION) has emerged as the more worrying concern for vision. In 2025 the World Health Organization estimated a doubling of NAION incidence in diabetics on semaglutide, but modelled this complication as still very rare at one additional case per 10,000 person-years of treatment.41 This stands in opposition to a 2024 report from the Massachusetts Eye and Ear Hospital, which found a fourfold increase in NAION for diabetic patients on semaglutide.42 Interestingly, the incidence of NAION increases fourfold in the first year after cataract surgery,43 yet this is not regarded as a contraindication to the procedure.
A class action against the manufacturers of Mounjaro for inadequate patient warnings about NAION is already in train.44 However this is a vexing chicken-and-egg problem. Patients prescribed a GLP-1 for obesity have an increased likelihood of obstructive sleep apnea, and sleep apnea by itself creates at least a threefold increased hazard of NAION.45 Further research will be needed to distinguish association from causality in this area. It is clear nevertheless that the many pros but significant cons of GLP-1s must be discussed with patients before prescribing, to obtain and document informed consent. My own advice to patients is to avoid GLP-1s if there is any past history of NAION.
Weight Rebound on Cessation of GLP-1s
Research shows that around 50% of conventional diets are followed by regaining of lost weight within two years,46 and GLP-1s also show discouraging rates of rebound. In one study, after 20 weeks of semaglutide half the subjects remained on it, losing a further 7.9% of body weight, but those who swapped to placebo gained 6.9%.47 This suggests that many will need to continue GLP-1 treatment long-term, burdened by the cost and risks entailed. Some tackle this problem with microdosing regimes,48 using longer intervals between injections and lower doses than usual.
There is an urgent need to pair GLP-1 prescribing with empathetic discussion of lifestyle interventions. These may allow eventual cessation of GLP-1 without major rebound. The ‘intuitive eating’49 approach points out that conventional dieting creates feelings of deprivation, anxiety and guilt about food, setting the stage for emotional eating and weight gain. Instead, the nutritionist authors recommend careful attention to the fundamental biological signals of hunger and fullness, as well as dealing with what makes this difficult – rules, beliefs, and thoughts about food. While it is true that we live in an obesogenic environment, it is my experience that many IIH patients are further disadvantaged by medications for anxiety and depression – it is common for IIH patients to tell me their weight soared after starting on this type of medication.
Attention should also be given to food choices, ideally with input from a nutritionist, and the role of exercise in maintaining weight loss. When all conservative measures fail, there is still a role for bariatric surgery to treat the IIH associated with severe obesity. The IIH Weight Trial showed that bariatric surgery reduces intracranial pressure more than traditional weight loss methods at two years.15
Stenting for IIH Unresponsive to Weight Loss
IIH in some patients proves refractory to weight loss. In one study,6 an average weight loss of 10.5 kg did not achieve remission in 44% of patients. There are also small numbers of patients with medically refractory IIH who are of normal weight, but who presumably have particularly severe transverse venous sinus stenosis. Medically refractory IIH is characterised by some or all of ongoing visual threat, intolerance of medication side effects, and disabling headache – while on maximal medical therapy, and after weight loss (if needed) has failed to improve disease severity.6 Where there is a significant underlying transverse sinus stenosis in refractory IIH, it can be treated with stenting (Figure 4), which props open the stenosis to normalise cerebral venous pressure and hence CSF outflow. Stenting is an extremely effective intervention, with a very acceptable safety profile.50 It reverses papilloedema in 94% of IIH patients with medically refractory disease.51

Figure 4 . Stenting for transverse venous sinus stenosis in medically refractory IIH (Image from Paul H Dressel, BFA. Copyright EI Levy, reproduced with permission.6
Conclusion
The importance of weight loss in IIH depends on IIH severity. In the 2% of fulminant disease that is acutely vision-threatening as assessed on the visual fields, immediate procedural intervention is the priority. In the 18% of disease that is medically refractory, trial of weight loss, by definition, has failed to provide remission, and transverse sinus stenting should be considered. The remaining 80% of IIH patients can be expected to respond to weight loss in combination with CSF-suppressing medication. In this group, GLP-1s are an effective tool for weight reduction, improving IIH control and providing many other health benefits. However, these medications are expensive as private scripts. They are not without risks, particularly NAION, sarcopenia, and weight rebound on cessation. Accompanying lifestyle modifications are therefore essential to prevent long-term dependence.
 Dr Kate Reid MBBS FRANZCO is a neuro-ophthalmologist now in private practice. As the Director of Ophthalmology at Canberra Hospital, she initiated co-management with both public and private optometry, and piloted the first use of Oculo in an Australian public hospital. She is a director of Vision 2020 Australia, an invited speaker for ophthalmology and optometry conferences, and a vision researcher at Australian National University.
Dr Kate Reid MBBS FRANZCO is a neuro-ophthalmologist now in private practice. As the Director of Ophthalmology at Canberra Hospital, she initiated co-management with both public and private optometry, and piloted the first use of Oculo in an Australian public hospital. She is a director of Vision 2020 Australia, an invited speaker for ophthalmology and optometry conferences, and a vision researcher at Australian National University.
References
- Xie J, Donaldson L, Margolin E. Papilledema: A review of etiology, pathophysiology, diagnosis, and management. Survey Ophth. 2022; 67 (4): 1135-1159. doi: 10.1016/j.survophthal.2021.11.007.
- Lichtenberg I, Blackwood E, Hawke S, et al. The prevalence of idiopathic intracranial hypertension and associated co-morbidities in Central Western New South Wales. J Neurol Neurosurg Psychiatry. 2017 88:e1 doi: 10.1136/jnnp-2017-316074.10.
- Mollan S, Davies B, Sinclair AJ, et al. Idiopathic intracranial hypertension: Consensus guidelines on management. J Neurol Neurosurg Psychiatry. 2018; 89:1088-100. doi: 10.1136/jnnp-2017-317440.
- Best J, Silvestri G, Acheson J, et al. the incidence of blindness due to idiopathic intracranial hypertension in the UK. Open Ophthalmol J. 2013; 28:26-9. doi: 10.2174/1874364101307010026.
- Chandran A, Pulhorn H, McMahon C. IIH VISION (venous intervention versus shunting in IIH for optic nerve disc swelling) trial: patient perspective questionnaire. Br J Neurosurg. 2019;33(1):71-75. doi: 10.1080/02688697.2017.1374349.
- Optic Disc Drusen: An international research alliance dedicated to advancing the field. Available at: opticdiscdrusen.com/ [accessed 2 Mar 2026].
- Heath JR, Chen F. Peripapillary hyperreflective ovoid mass-like structures: Multimodal imaging—A review. Clin Experiment Ophthalmol. 2023; 51(1): 67-80. doi: 10.1111/ceo.14182.
- Ma J, Nguyen P, Reid K, et al. Arnold–Chiari malformation is associated with increased likelihood of a procedure in idiopathic intracranial hypertension. Front. Ophthalmol. 2025; 5:1668498. doi: 10.3389/fopht.2025.1668498.
- Patsalides A, Oliveira C, Drinkin M, et al. Venous sinus stenting lowers the intracranial pressure in patients with idiopathic intracranial hypertension. J Neurointerv Surg (2019); 11:175-8. doi: 10.1136/neurintsurg-2018-014032.
- Sugerman H, DeMaria J, Sismanis A, et al. Increased intra-abdominal pressure and cardiac filling pressures in obesity-associated pseudotumor cerebri. Neurology 1997;49(2):507-11. doi: 10.1212/wnl.49.2.507.
- Hornby C, Mollan S, Sinclair A, et al. Metabolic concepts in idiopathic intracranial hypertension and their potential for therapeutic intervention. J Neuroophthalmol. 2018;38(4):522-530. doi: 10.1097/WNO.0000000000000684.
- Adderley N, Subramanian A, Sinclair A, et al. Association between idiopathic intracranial hypertension and risk of cardiovascular diseases in women in the United Kingdom. JAMA Neurol. 2019;76:1088-1098. doi: 10.1001/jamaneurol.2019.1812.
- Mollan S, Wakerley B, A Sinclair A, et al. Intracranial pressure directly predicts headache morbidity in idiopathic intracranial hypertension. J Headache Pain. 2021; 22, 118. doi: 10.1186/s10194-021-01321-8.
- Szewka A, Bruce B, Newman N, Biousse V. Idiopathic intracranial hypertension: relation between obesity and visual outcomes. J Neuroophthalmol. 2013;33:4-8. doi: 10.1097/WNO.0b013e31823f852d.
- Mollan S, Mitchell J, Sinclair AJ, et al. Effectiveness of bariatric surgery vs community weight management intervention for the treatment of IIH: a randomized clinical trial. JAMA Neurol. 2021;78:678-686. doi: 10.1001/jamaneurol.2021.0659.
- Ang J, Teo K, Fraser C. Weight loss in idiopathic intracranial hypertension: A retrospective review of outcomes in the clinical setting. J Neuroophthalmol. 2021 1;41(4):e458-e463. doi: 10.1097/WNO.0000000000001107.
- Mann T, Tomiyama AJ, Chatman J, et al. Medicare’s search for effective obesity treatments: diets are not the answer. Am Psychol. 2007;62:220-233. doi: 10.1037/0003-066X.62.3.220.
- Barber T, Hanson P, Weickert M, Franks S. Obesity and polycystic ovary syndrome: Implications for pathogenesis and novel management strategies. Clin Med Insights Reprod Health. 2019 9;13:1179558119874042. doi: 10.1177/1179558119874042.
- Mosenzon O, Garvey W, Le Roux CW, et al. Clinically-relevant weight loss is achieved independently of early weight loss response to once-weekly subcutaneous semaglutide 2.4 MG J Endocr Soc. 2021;5(Suppl 1):A7. doi: 10.1210/jendso/bvab048.013.
- Aronne L, Horn DB, Dunn J, et al. SURMOUNT-5 Trial Investigators. Tirzepatide as compared with semaglutide for the treatment of obesity. N Engl J Med. 2025 3;393(1):26-36. doi: 10.1056/NEJMoa2416394.
- Mitchell J, Lyons H, Sinclair AJ, et al. The effect of GLP-1RA exenatide on idiopathic intracranial hypertension: a randomized clinical trial. Brain. 2023;146(5):1821-1830. doi: 10.1093/brain/awad003. doi: 10.1093/brain/awad003.
- Azzam A, Nassar M, Altschul DJ, et al. Safety and efficacy of metformin for idiopathic intracranial hypertension. A U.S-based real-world data retrospective multicenter cohort study. ASIDE Intern Med. 2025;1(1):12-19. doi: 10.71079/2024001001.
- Malhotra A, Grunstein R, Bednarik J, et al. SURMOUNT-OSA Investigators. Tirzepatide for the Treatment of Obstructive Sleep Apnea and Obesity. N Engl J Med. 2024;391(13):1193-1205. doi: 10.1056/NEJMoa2404881.
- Vasu P, Dorairaj E, Bednarik, et al; SURMOUNT-OSA Investigators, Risk of glaucoma in patients without diabetes using a glucagon-like peptide 1 receptor agonist. Ophthalmology. 2025; 132 (8): 859-868. doi: 10.1016/j.ophtha.2025.03.021.
- Allan K, Joo J, Rachitskaya A, et al. Glucagon-like peptide-1 receptor agonist impact on chronic ocular disease including age-related macular degeneration. Ophthalmology. 2025; 132 (7): 748-757. doi: 10.1016/j.ophtha.2025.01.016.
- Tang H, Donahoo W, Guo J, et al. GLP-1RA and SGLT2i medications for type 2 diabetes and alzheimer disease and related dementias. JAMA Neurol. 2025;82(5):439-449. doi: 10.1001/jamaneurol.2025.0353.
- Lange M, Vickers A, Lee AG, et al. Pro-Con: Antiobesity drugs such as glucagon-like peptide-1 receptor agonists should be a first-line treatment in idiopathic intracranial hypertension. J Neuroophthalmol. 2026;46(1):117-127. doi: 10.1097/WNO.0000000000002431.
- Lincoff A, Brown-Frandsen K, Ryan D, et al. SELECT Trial Investigators. Semaglutide and Cardiovascular Outcomes in Obesity without Diabetes. N Engl J Med. 2023;389(24):2221-2232. doi: 10.1056/NEJMoa2307563.
- Falster M, Costa J, Hardt-Lindberg S, et al; for the SELECT Trial Investigators. The GLP-1 RA boom: Trends in publicly subsidised and private access in Australia, 2020-2025. medRxiv. Preprint 2025. doi: 10.1101/2025.10.30.25339120.
- Attwooll J. Are we at a ‘watershed moment’ for weight-loss drugs, RACGP, 27 May 2025. Available at www1.racgp.org.au/newsgp/professional/are-we-at-a-watershed-moment-for-weight-loss-drugs [accessed 8 Mar 2026].
- Australian and New Zealand College of Anaesthetists GLP-1 receptor agonists – clinical practice recommendations. 2025. Available at: anzca.edu.au/safety-and-advocacy/standards-of-practice/clinical-practice-recommendations-regarding-patients-taking-glp-1 [accessed 8 Mar 2026].
- Ren Q, Zhi L, Liu H. Semaglutide therapy and accelerated sarcopenia in older adults with type 2 diabetes: A 24-month retrospective cohort study. Drug Des Devel Ther. 2025;19:5645-5652. doi: 10.2147/DDDT.S531778.
- Tzoulis P, Batavanis M. Predictors of poor response to semaglutide for weight management. Endocrine AbAbstracts. 2024;99RC12.2 2024; 99 RC12.2. doi: 10.1530/endoabs.99.RC12.2.
- Xie Y, Choi T, Al-Aly Z. Mapping the effectiveness and risks of GLP-1 receptor agonists. Nat Med 2025; (31) 951-962. doi: 10.1038/s41591-024-03412-w.
- Kalsi H, Arora SS, Brar TS, et al. Semaglutide-induced liver injury. ACG Case Rep J. 2025;12(8):e01776. doi: 10.14309/crj.0000000000001776.
- Drummond R, Seif K, Reece E. Glucagon-like peptide-1 receptor agonist use in pregnancy: a review. Am J Obstet Gynecol. 2025;232(1):17-25. doi: 10.1016/j.ajog.2024.08.024.
- Feier C, Vonica R, Muntean C, et al. Assessment of thyroid carcinogenic risk and safety profile of GLP1-RA semaglutide (Ozempic) therapy for diabetes mellitus and obesity: A systematic literature review. Int J Mol Sci. 2024; 15;25(8):4346. doi: 10.3390/ijms25084346.
- Ayoub M, Chela H, Daglilar E, et al. Pancreatitis risk associated with GLP-1 receptor agonists. J Clin Med. 2025;14(3):944. doi: 10.3390/jcm14030944.
- Schoretsanitis G, Weiler S, Gastaldon C, et al. Disproportionality analysis from World Health Organization data on semaglutide, liraglutide, and suicidality. JAMA Network Open. 2024;7(8):e2423385. doi: 10.1001/jamanetworkopen.2024.23385.
- Hari J, Magic Pill. 1st ed. Bloomsbury Publishing 2024.
- European Medicines Agency. PRAC concludes eye condition NAION is a very rare side effect of semaglutide medicines Ozempic, Rybelsus and Wegovy, available at: ema.europa.eu/en/news/prac-concludes-eye-condition-naion-very-rare-side-effect-semaglutide-medicines-ozempic-rybelsus-wegovy [accessed 8 Mar 2026].
- Hathaway JT, Shah MP, Rizzo III JF et al. Risk of nonarteritic anterior ischemic optic neuropathy in patients prescribed semaglutide. JAMA Ophthalmol. 2024;142(8):732–739. doi: 10.1001/jamaophthalmol.2024.2296.
- Shew W, Wang M, Danesh-Meyer H. Nonarteritic anterior ischemic optic neuropathy after cataract surgery: A systematic review and meta-analysis. J Neuroophthalmol. 2023;43(1):17-28. doi: 10.1097/WNO.0000000000001625.
- King Law, Mounjaro eye side effects lawsuit, available at: robertkinglawfirm.com/personal-injury/mounjaro-lawsuit/mounjaro-eye-side-effects-lawsuit/ [accessed 7 Mar 2026].
- Archer EL, Pepin S. Obstructive sleep apnea and nonarteritic anterior ischemic optic neuropathy: evidence for an association. J Clin Sleep Med. 2013;9(6):613-8. doi: 10.5664/jcsm.2766.
- Khattab, R. Weight loss programs: Why do they fail? A multidimensional approach for obesity management. Curr Nutr Rep 2024;13, 478–499. doi: 10.1007/s13668-024-00551-x.
- Rubino D, Abrahamsson N, Dicker D, et al; for the STEP 4 Investigators. Effect of continued weekly subcutaneous semaglutide vs placebo on weight loss maintenance in adults with overweight or obesity: The STEP 4 randomized clinical trial. JAMA. 2021;325(14):1414-1425. doi: 10.1001/jama.2021.3224.
- Komé A, Chandran M, Klein K et al. One size does not fit all: Understanding microdosing semaglutide for diabetes in multidose pens. Diabetes Care 2025; 48 (3): e25-e27. doi: 10.2337/dc24-2575.
- Tribole E, Resch E. Intuitive eating. 3rd ed. St Martin’s Press 2012.
- Reid K, Winters HS, Halmagyi GM, et al. transverse sinus stenting reverses medically refractory idiopathic intracranial hypertension. Front. Ophthalmol. 2022; 2:885583. doi: 10.3389/fopht.2022.885583.
- Townsend R, Jost A, Fargen K, et al. Major complications of dural venous sinus stenting for idiopathic intracranial hypertension: case series and management considerations. J Neurointerv Surg. 2022;14(1):neurintsurg-2021-017361. doi: 10.1136/neurintsurg-2021-017361.
- Nicholson P, Brinjikji W, Lenck S, et al. Venous sinus stenting for idiopathic intracranial hypertension: a systematic review and meta-analysis J Neurointerv Surg. 2019;11:380-385. doi: 10.1136/neurintsurg-2018-014172.