

The demographic landscape of dry eye disease (DED) is shifting, yet women navigating the menopausal transition continue to represent a significant cohort with ocular surface complaints.1
In our main article, Assistant Professor Chris Lim explores the distinct challenge that menopause poses to ocular surface homeostasis. In a second article, Megan Zabell reviews recent research that evaluated real‑world, short‑term efficacy and tolerability of a single dose of Systane Complete administered to adults presenting with aqueous-deficient, evaporative, and mixed DED symptoms.
LEARNING OBJECTIVES
On completion of this CPD article, participants should be able to:
- Understand the specific roles of sex steroids (androgens, oestrogens, and progestogens) in maintaining ocular surface homeostasis,
- Describe why systemic hormone replacement therapy often fails to alleviate, or even exacerbates, dry eye symptoms, and
- Implement targeted management strategies that address the root cause of menopausal dry eye.
One of the most compelling features of DED is its sex predilection; female sex is a significant, independent risk factor for its development.2 There is a further increase in DED prevalence in this patient cohort that is not simply due to ageing, but rather distinct hormonal changes occurring at the cellular level.3 The menopausal transition represents complex hormonal shifts where withdrawal of sex steroids precipitates ocular surface dyshomeostasis.
To understand this demographic, we must be familiar with the physiological stages involved. Perimenopause is the transitional phase, often beginning in a woman’s mid-to-late 40s, characterised by erratic hormonal fluctuations.4 During this period, oestrogen levels can fluctuate unpredictably, while androgen levels begin a steady, linear decline. The transition from pre-menopause to perimenopause can be marked by various vasomotor symptoms, including night sweats and hot flushes.5 Menopause is defined retrospectively as 12 consecutive months of amenorrhea, marking permanent cessation of ovarian function.4
Large-scale epidemiological studies provide robust evidence. Population-based studies, such as the Women’s Health Study, report that women have a roughly 1.5 to twofold higher age-adjusted risk of DED compared to men.6 Similarly, the Beaver Dam Offspring Study reported a higher prevalence of dry eye symptoms in women (17.9%) compared to men (10.5%).7 The prevalence of DED climbs steadily during perimenopause and peaks in the post-menopausal years, with 50–70% of peri- and postmenopausal women reporting significant symptoms in clinic cohorts, although general population estimates are lower at between 15–20%.8,9
The impact of disease burden on quality of life (QoL) is profound. Menopausal women frequently report that DED significantly impairs daily activities such as prolonged reading, driving, and digital screen use. The associated chronic pain and visual fluctuation also carries a well-documented psychological burden, correlating with higher rates of anxiety and depressive symptoms.10
Effective management of this patient subset requires us to look beyond the generic label of ‘dry eye’ and understand specific endocrine deficiencies underpinning these changes.
The Endocrine Regulation of the Ocular Surface
To understand why the menopausal eye fails, we must first recognise the ocular surface as a sex-steroid-responsive tissue. Historically, oestrogen has received the lion’s share of attention in women’s health, yet contemporary research increasingly recognises androgens as the primary regulators of meibomian gland function.11
Meibomian glands are large sebaceous glands, and like their skin counterparts, they are androgen-dependent target organs. Androgens exert a profound impact, regulating expression of numerous genes in human meibomian gland epithelial cells.12 Specifically, they stimulate dozens of ontologies concerned with lipid biosynthesis and transport, while simultaneously suppressing genes related to keratinisation.12 Androgens also exert anti-inflammatory effects, downregulating pro-inflammatory pathways including cytokines such as TNF-α, IL-1β, and IL-6 in-vitro and in animal models.13
During the menopausal transition, circulating levels of androgens and their precursors decline progressively.3 This results in glandular atrophy, altered lipid profiles, and meibomian gland orifice metaplasia.14
Oestrogen can counter some androgen-mediated pathways in the meibomian gland and exert anti-sebaceous effects, though its net impact is complex.11 This creates a treatment paradox where systemic hormone replacement therapy, particularly oestrogen-only formulations, have been associated with worsening dry eye symptoms.6 In the Women’s Health Study, women using oestrogen-only postmenopausal hormone therapy had a 69% increased risk of DED compared to non-users.6 This underscores the risk that systemic oestrogen delivery may exacerbate tear instability.
The Vicious Cycle of Evaporation
This hormonal cascade triggers a specific sequence of events on the ocular surface. The primary insult is androgen deprivation, which causes meibomian glands to atrophy and fail.15 This hyposecretory meibomian gland dysfunction (MGD), characterised by dwindling meibum secretion and an altered lipid profile, causes the tear film lipid layer to thin and break down, accelerating evaporative loss.16
Rapid evaporation leads to a hyperosmolar and hostile environment for the ocular surface. This hyperosmotic stress initiates an inflammatory cascade, damaging goblet cells, and further destabilises the tear film.16 Clinically, this manifests as fluctuating and blurred vision, burning, and grittiness. Paradoxically, patients may report epiphora, which represents a reflex tearing response triggered by ocular surface desiccation in an attempt to compensate for the poor lipid layer quality.
Clinical Evaluation
The diagnosis of dry eye disease can be established by a positive symptom score, combined with at least one biophysical marker of homeostasis loss.
Symptom-sign dissociation is common in DED and menopausal women report more severe symptoms.10 Use of symptom questionnaires facilitates documentation of these signs. These questionnaires facilitate validation of the patient’s subjective experience, which is often dismissed, while repeating this at follow up provides a tangible metric to monitor treatment efficacy.
Ocular Surface Disease Index-6 (OSDI-6). The shortened OSDI-6 is validated in patients with dry eye disease and is a highly efficient alternative for busy clinical practices.17 It focuses on six discriminatory questions regarding visual function and ocular discomfort. A score >13 indicates symptomatic disease.18
Standard Patient Evaluation of Eye Dryness (SPEED). SPEED was validated specifically for the evaluation of evaporative dry eye disease and MGD. Unlike the OSDI, which prioritises visual function, SPEED focuses on the frequency and severity of symptoms such as dryness, grittiness, and soreness. A score ≥8 is indicative of symptomatic disease.19
Dry Eye Questionnaire 5 (DEQ-5). This five-item screening tool, with demonstrated sensitivity in distinguishing DED from healthy eyes, measures the frequency of watery eyes and discomfort, as well as the intensity of symptoms. A score >6 indicates dry eye disease, while a score >12 should trigger suspicion for Sjögren’s syndrome.20
A diagnosis is confirmed when a patient presents with positive symptoms alongside any one of these biophysical markers: tear film instability, which is the primary driver; hyperosmolarity, which serves as the metabolic stressor; or ocular surface staining, which reflects underlying tissue damage.
Tear film osmolarity. Hyperosmolarity serves as a quantitative biomarker of evaporative stress. A reading of ≥308 mOsm/L in either eye, or an interocular difference of >8 mOsm/L, is widely accepted as indicative of a loss of homeostasis.
Ocular surface staining. Corneal fluorescein staining remains the definitive marker of epithelial compromise driven by desiccation and hyperosmolar stress. Fluorescein is useful for identifying corneal damage (>5 punctate spots), while lissamine green assists with visualising bulbar conjunctival compromise (>9 punctate spots), and quantifying lid wiper epitheliopathy (≥2 mm length and ≥25% width).16
Tear break-up time (TBUT). Assessing non-invasive TBUT (NIBUT) or fluorescein TBUT is paramount. A rapid break-up time (<10 seconds for NIBUT and <5 seconds for fluorescein TBUT) is the hallmark of tear film instability.16
Given the primary role of lipid layer instability in these patients, clinical evaluation should include assessment of meibomian gland function and evaporative dynamics.
Meibomian gland expression. Application of gentle pressure to lid margins allows evaluation of meibum expressibility and quality.16 In cases of meibomian gland dysfunction, the clear, oil-like meibum is replaced by cloudy, opaque, or toothpaste-like secretions, or may be absent due to terminal duct obstruction.
Meibography. Utilising infrared imaging to visualise the meibomian gland structure facilitates quantification of glandular dropout and architectural distortion. This provides a tangible metric of disease severity for both the clinician and the patient.16
Management: A Holistic Approach
Managing menopausal DED requires a staged, comprehensive approach that addresses both lifestyle factors and the underlying tear film deficiency.
Lifestyle and behavioural modifications. Lifestyle modifications represent the first line of management.21 This includes counselling on localised environmental control and optimising digital screen habits via conscious blinking exercises to facilitate meibum release. Dietary modifications, particularly high-quality omega-3 fatty acid supplementation, have mixed evidence but plausible benefits for lipid profiles and inflammation.
Advanced lubrication. While lifestyle and behavioural changes are essential, topically applied lubricant drops are the mainstay of DED treatment.21 Historically, the standard of care for patients with dry eye disease was aqueous supplementation. However, in patients whose dry eye disease involves evaporative loss, aqueous supplementation merely addresses the volume deficit while neglecting the evaporative component. Therefore, incorporating lipid replacement constituents is a rational therapeutic strategy that may be considered to supplement the compromised lipid layer.
Systane Complete is a lipid-containing nanoemulsion that has been demonstrated to be beneficial for all DED subtypes.22,23 Its utility lies in its dual-action mechanism, which concurrently addresses aqueous and lipid deficiencies. The formulation uses a proprietary nano-emulsion process that incorporates mineral oil and phospholipids.22 Upon instillation, these droplets form a cohesive barrier that replenishes the lipid layer.23 This stabilisation reduces evaporative loss, addressing the key driver associated with menopausal eye disease. Supporting this lipid layer is hydroxypropyl-guar (HP-Guar). This polymer forms a viscoelastic meshwork that binds to the ocular surface and has a predilection for damaged and hydrophobic regions of the epithelium.24 It acts as a hydration scaffold, retaining moisture and allowing the corneal surface to heal while providing extended retention of the nano-lipid layer above it.
Procedural adjuncts can be considered when foundational therapies and lubrication strategies require further supplementation.21 In the management of advanced MGD, in-office therapies such as intense pulsed light (IPL) therapy, low-level light therapy (LLLT), and vectored thermal pulsation (such as LipiFlow) can emulsify inspissated meibum, reduce lid margin inflammation, and rehabilitate glandular function. Punctal occlusion may also be considered to retain natural tears and artificial lubricants; however, in predominantly evaporative and inflammatory DED, care must be taken to first control the ocular surface inflammation before occluding the puncta, lest inflammatory mediators be trapped against the ocular surface.
Conclusion
Menopause poses a distinct challenge to ocular surface homeostasis, substantially influenced by androgen decline and meibomian gland dysfunction. Recognising that these patients’ underlying dry eye disease has a significant contributory component from evaporative loss, clinical recommendations should consider advanced lipid-replenishing formulations to address the lipid-deficient component of tear film instability. Restoring the lipid barrier provides more than immediate symptomatic relief; it shields the ocular surface from the chronic stress of desiccation and hyperosmolarity, addressing the primary driver of menopausal dry eye.
How Can Systane Complete Lubricant Eyedrops Help? |
|---|
| WRITER: Megan Zabell
As detailed by Assistant Professor Lim, the hormonal shifts of peri- and postmenopause frequently drive tear film instability. This summary evaluates a lubricant formulation designed to address the full clinical spectrum of dry eye, providing sustained relief across aqueous-deficient (ADDE), evaporative (EDE), and mixed DED presentations. Silverstein and coworkers conducted a Phase 4, multicentre clinical trial to evaluate the onset, magnitude, and duration of symptomatic relief following administration of a single drop of Systane Complete (Alcon), a propylene glycol–hydroxypropyl guar (PG‑HPG) nanoemulsion designed to target all three layers of the tear film.25 The study assessed symptom improvement, subjective soothing effect, and tolerability in patients with ADDE, EDE, and mixed subtypes of dry eye disease. The published findings, Symptom relief following a single dose of PG‑HPG nanoemulsion (Systane Complete),25 demonstrated clinically meaningful and statistically significant symptom improvement lasting at least eight hours post‑instillation, with excellent tolerability and broad efficacy across ADDE, EDE, and mixed DED. Role of Artificial TearsArtificial tears are typically formulated to supplement aqueous volume or enhance lipid layer stability. Systane Complete is engineered as a universal formulation to concurrently relieve symptoms of both evaporative and aqueous‑deficient mechanisms through: Propylene glycol (PG). A demulcent providing immediate surface lubrication and osmoprotective effects. Hydroxypropyl guar (HPG). Forms a viscoelastic gel‑like matrix that mimics mucin function and increases retention time. Nano‑sized lipid droplets (1–100 nm). Enhances spreadability on the ocular surface, stabilising the lipid layer, and reducing evaporation. Previous long‑term studies have reported that Systane Complete produces early symptom relief and progressive improvement in ocular surface signs over several months.26 Study PurposeThe objective of the Phase 4 trial was to evaluate real‑world, short‑term efficacy and tolerability of a single dose of Systane Complete administered to adults with symptomatic ADDE, EDE, or mixed DED. Key outcomes included:
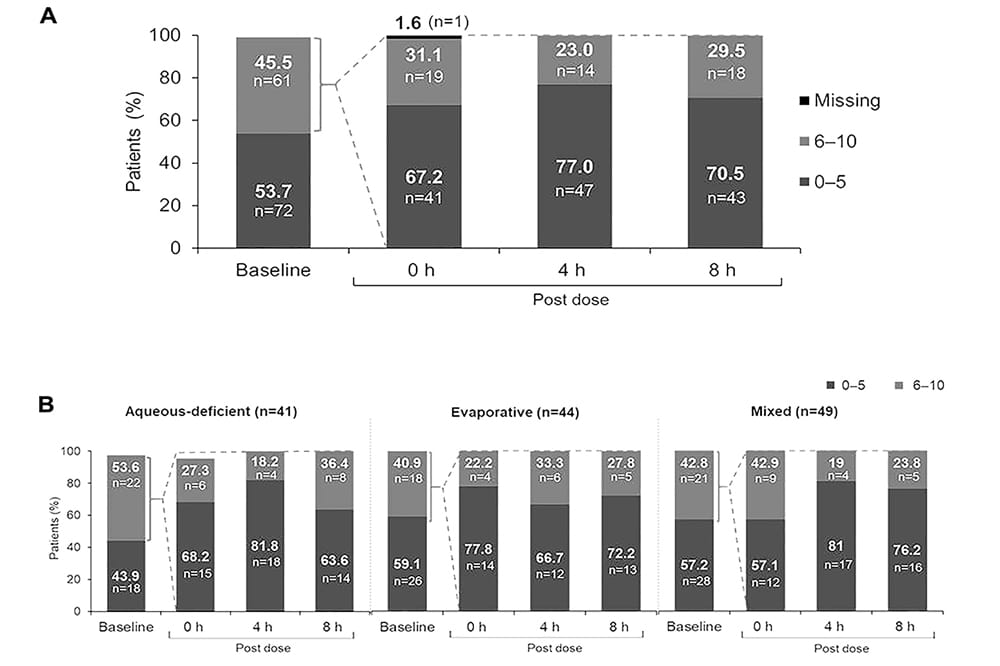
SubjectsA total of 130 subjects completed the study. Each DED subtype was well-represented, comprising approximately one-third of the study population: 30.6% ADDE, 32.8% EDE, and 36.6% mixed. Subtype classification was performed using Schirmer I test and meibum quality scores. ProtocolParticipants were administered a single drop of Systane Complete in the morning and were asked to refrain from using eye drops for eight hours. Patient-reported outcomes assessments regarding dry eye symptom severity, soothing sensation, and eye drop tolerability were performed at baseline (pre-instillation), immediately following drop instillation (0 hours), at 4 ± 1 hours, and 8 ± 1 hours. Dry Eye Symptom ScoresAt instillation (0 hours), four and eight hours, median dry eye symptom scores were reduced by one, two, and two points, respectively. Among participants with severe baseline symptoms (scores 6–10), the majority transitioned to a lower symptom category (0–5) following instillation: 67.2% at zero hours, 77% at four hours, and 70.5% at eight hours. These data suggest a sustained therapeutic effect lasting hours after instillation. Significant score improvements were sustained through eight hours across all DED subtypes, with effects observed as early as zero hours for ADDE and EDE, and by four hours for mixed DED. Soothing Sensation ScoresOver 80% of patients experienced a soothing sensation that lasted over eight hours. Patients reported a consistent soothing sensation following instillation, with median scores of three through four hours. They reported maintaining a high level of relief (3.5) at the eight-hour mark. Median soothing sensation scores for each dry eye sub-type are given in Table 1.  Table 1. Median soothing sensation scores (0 = eyes feeling good, 10 = no soothing feeling at all) at zero, four, and eight hours after drop instillation, categorised by type of dry eye. Tolerability Assessment ScoreTolerability was high across all parameters. Over 92% of participants reported scores of 0–5 for each component (burning sensation, stinging sensation, blur, and foreign body sensation). Median scores were zero across all categories; ranging from 0–8 for burning, stinging and blur and 0–10 for foreign body sensation. These findings remained consistent when participants were stratified by DED subtype. Clinical Implications for Eye‑Care ProfessionalsSystane Complete is designed to address both aqueous and evaporative pathology, simplifying DED management when subtype distinctions are unclear or when mixed mechanisms are present. The study provides evidence that one morning dose delivers up to eight hours of symptomatic relief, and is useful for:
Rapid onset of relief may support use in patients whose symptoms interfere with daily visual tasks, such as computer use, reading, or driving. The sustained benefit suggests improved tear film homeostasis and enhanced surface protection. A low rate of treatment‑related discomfort supports its use even in sensitive or highly symptomatic patients. This study strengthens the scientific foundation for recommending Systane Complete as a versatile first‑line artificial tear for a broad range of DED presentations. ConclusionFindings from Silverstein and coworkers demonstrate that a single drop of Systane Complete provides rapid, meaningful, and sustained symptom relief for at least eight hours across all major subtypes of dry eye disease for many patients. This is particularly relevant given that many patients, including women experiencing perimenopausal or menopausal hormonal shifts, commonly present with evaporative dry eye driven by MGD and increased tear film instability. While this study did not specifically investigate menopausal status, demonstration of symptomatic improvement in evaporative dry eye supports its clinical utility in dry eye patients for whom lipid‑layer compromise plays a central role. Importantly, the formulation was well tolerated, with a reported soothing effect in more than 80% of participants, and over 90% reporting minimal to no discomfort across tolerability metrics. These findings provide eye care professionals with compelling evidence to recommend this broad-spectrum artificial tear option to patients who may require both lipid-layer support and improved tear film stability. This includes those undergoing hormonal transitions that predispose them to evaporative dry eye. |

Figure 1. A) The improvement experienced in dry eye symptom scores at zero, four, and eight hours after instillation of Systane Complete. Lower scores are shown in dark grey and higher values in lighter grey. B). The same data, stratified by type of dry eye.

Figure 2. Tolerability scores at zero, four, and eight hours after drop instillation, stratified by dry eye subtype classification.

This article is sponsored by Alcon.
ANZ-SYX-2600006
 Assistant Professor Prof (Dr) Chris Hong Long Lim BSc (Med) BMed MD PhD MMed (Ophth) FAMS FRANZCO is a consultant ophthalmic surgeon practising in Singapore and Australia. He is a subspecialist in cornea, refractive surgery, and oculoplastics, with clinical interests in comprehensive ocular surface management, complex anterior segment reconstruction, and advanced vision correction surgery.
Assistant Professor Prof (Dr) Chris Hong Long Lim BSc (Med) BMed MD PhD MMed (Ophth) FAMS FRANZCO is a consultant ophthalmic surgeon practising in Singapore and Australia. He is a subspecialist in cornea, refractive surgery, and oculoplastics, with clinical interests in comprehensive ocular surface management, complex anterior segment reconstruction, and advanced vision correction surgery.
 Megan Zabell BSc MOptom has been a member of Alcon Vision Care’s Professional Affairs Team since 2018. She graduated from the University of Melbourne as a therapeutically endorsed optometrist in 2011 and has previously worked in a private optometry practice and also taught preclinical optometry at the University of Melbourne. She has a particular interest in the treatment of dry eye.
Megan Zabell BSc MOptom has been a member of Alcon Vision Care’s Professional Affairs Team since 2018. She graduated from the University of Melbourne as a therapeutically endorsed optometrist in 2011 and has previously worked in a private optometry practice and also taught preclinical optometry at the University of Melbourne. She has a particular interest in the treatment of dry eye.
References
- Matossian C, McDonald M, Gupta PK, et al. Dry eye disease: Consideration for women’s health. J Womens Health (Larchmt). 2019 Apr;28(4):502-514. doi: 10.1089/jwh.2018.7041.
- Schaumberg DA, Sullivan DA, Buring JE, Dana MR. Prevalence of dry eye syndrome among US women. Am J Ophthalmol. 2003 Aug;136(2):318-26. doi: 10.1016/s0002-9394(03)00218-6.
- Gorimanipalli B, Khamar P, Sethu S, Shetty R. Hormones and dry eye disease. Indian J Ophthalmol. 2023 Apr;71(4):1276-1284. doi: 10.4103/IJO.IJO_2887_22.
- Gold EB. The timing of the age at which natural menopause occurs. Obstet Gynecol Clin North Am. 2011 Sep;38(3):425-40. doi: 10.1016/j.ogc.2011.05.002.
- Islam RM, Bond M, Davis SR, et al. Prevalence and severity of symptoms across the menopause transition: cross-sectional findings from the Australian Women’s Midlife Years (AMY) Study. Lancet Diabetes Endocrinol. 2025 Sep;13(9):765-776. doi: 10.1016/S2213-8587(25)00138-X.
- Schaumberg DA, Buring JE, Sullivan DA, Dana MR. Hormone replacement therapy and dry eye syndrome. JAMA. 2001 Nov 7;286(17):2114-9. doi: 10.1001/jama.286.17.2114.
- Paulsen AJ, Cruickshanks KJ, Dalton DS, et al. Dry eye in the Beaver Dam Offspring Study: prevalence, risk factors, and health-related quality of life. Am J Ophthalmol. 2014 Apr;157(4):799-806. doi: 10.1016/j.ajo.2013.12.023.
- Garcia-Alfaro P, Bergamaschi L, Rodríguez I, et al. Prevalence of ocular surface disease symptoms in peri- and postmenopausal women. Menopause. 2020 Sep;27(9):993-998. doi: 10.1097/GME.0000000000001565.
- Peck T, Olsakovsky L, Aggarwal S. Dry eye syndrome in menopause and perimenopausal age group. J Midlife Health. 2017 Apr-Jun;8(2):51-54. doi: 10.4103/jmh.JMH_41_17.
- Garcia-Alfaro P, Garcia S, Rodriguez I, Vergés C. Dry eye disease symptoms and quality of life in perimenopausal and postmenopausal women. Climacteric. 2021 Jun;24(3):261-266. doi: 10.1080/13697137.2020.1849087.
- Wang LX, Deng YP. Androgen and meibomian gland dysfunction: from basic molecular biology to clinical applications. Int J Ophthalmol. 2021 Jun 18;14(6):915-922. doi: 10.18240/ijo.2021.06.18.
- Khandelwal P, Liu S, Sullivan DA. Androgen regulation of gene expression in human meibomian gland and conjunctival epithelial cells. Mol Vis. 2012;18:1055-67. Epub 2012 Apr 27. PMID: 22605918.
- Marangoz D, Oner C, Sahin A, et al. The effect of androgens on proinflammatory cytokine secretion from human ocular surface epithelial cells. Ocul Immunol Inflamm. 2021 Apr 3;29(3):546-554. doi: 10.1080/09273948.2019.1686155.
- Krenzer KL, Dana MR, Sullivan DA, et al. Effect of androgen deficiency on the human meibomian gland and ocular surface. J Clin Endocrinol Metab. 2000 Dec;85(12):4874-82. doi: 10.1210/jcem.85.12.7072.
- Sullivan DA, Rocha EM, Willcox MDP, et al. TFOS DEWS II sex, gender, and hormones report. Ocul Surf. 2017 Jul;15(3):284-333. doi: 10.1016/j.jtos.2017.04.001.
- Wolffsohn JS, Benítez-Del-Castillo JM, Jones L, et al; TFOS collaborator group. TFOS DEWS III: Diagnostic methodology. Am J Ophthalmol. 2025 Nov;279:387-450. doi: 10.1016/j.ajo.2025.05.033.
- Perez VL, Chen W, Sullivan DA, et al. TFOS DEWS III: Executive summary. Am J Ophthalmol. 2026 Feb;282:135-145. doi: 10.1016/j.ajo.2025.09.035.
- Pult H, Wolffsohn JS. The development and evaluation of the new ocular surface disease index-6. Ocul Surf. 2019 Oct;17(4):817-821. doi: 10.1016/j.jtos.2019.08.008.
- Ngo W, Situ P, Simpson T, et al. Psychometric properties and validation of the standard patient evaluation of eye dryness questionnaire. Cornea. 2013 Sep;32(9):1204-10. doi: 10.1097/ICO.0b013e318294b0c0.
- Chalmers RL, Begley CG, Caffery B. Validation of the 5-item dry eye questionnaire (DEQ-5): Discrimination across self-assessed severity and aqueous tear deficient dry eye diagnoses. Cont Lens Anterior Eye. 2010 Apr;33(2):55-60. doi: 10.1016/j.clae.2009.12.010.
- Jones L, Craig JP, Wolffsohn JS, et al; TFOS Collaborator Group. TFOS DEWS III: Management and Therapy. Am J Ophthalmol. 2025 Nov;279:289-386. doi: 10.1016/j.ajo.2025.05.039.
- Sharma N, Bari A, Dasgupta A, et al. To assess the effectiveness of Systane Complete in improving meibomian gland score and in reducing symptoms of ocular dryness. Front Ophthalmol (Lausanne). 2025 Nov 6;5:1577836. doi: 10.3389/fopht.2025.
- Yeu E, Silverstein S, Manoj V, et al. Efficacy and safety of phospholipid nanoemulsion-based ocular lubricant for the management of various subtypes of dry eye disease: A phase IV, multicenter trial. Clin Ophthalmol. 2020 Sep 1;14:2561-2570. doi: 10.2147/OPTH.S261318.
- Rangarajan R, Kraybill B, Ogundele A, Ketelson HA. Effects of a hyaluronic acid/hydroxypropyl guar artificial tear solution on protection, recovery, and lubricity in models of corneal epithelium. J Ocul Pharmacol Ther. 2015 Oct;31(8):491-7. doi: 10.1089/jop.2014.0164.
- Silverstein S, Yeu E, Manoj V, et al. Symptom relief following a single dose of propylene glycol-hydroxypropyl guar nanoemulsion in patients with dry eye disease: A phase IV, multicenter trial. Clin Ophthalmol. 2020 Oct 9;14:3167-3177. doi: 10.2147/OPTH.S263362.
- Craig JP, Muntz A, Wolffsohn JS, et al. Developing evidence-based guidance for the treatment of dry eye disease with artificial tear supplements: A six-month multicentre, double-masked randomised controlled trial. Ocul Surf. 2021 Apr;20:62-69. doi: 10.1016/j.jtos.2020.12.006.





