
Laser assisted in situ keratomileusis (LASIK) and orthokeratology (OK) are excellent options to correct myopia in adults. They both provide myopic correction by flattening the central cornea while creating a relative steepening of the peripheral cornea. However some patients who have undergone LASIK refractive surgery to correct for myopia may regress in subsequent years.
There are many options for post- LASIK myopic vision correction, including refractive surgery enhancement or retreatment, or optical correction with spectacles or contact lenses. Another option, which is often used to treat children with myopia, is OK, as the following case study demonstrates.
Marilyn* is a 32 year old Caucasian female, who presented to discuss options for post-LASIK myopic vision correction. She presented with low to moderate myopia, and had been regressing in myopia in both eyes since LASIK refractive surgery nine years prior. Before LASIK, Marilyn reported her spectacle prescription to be about -6.00 to -7.00 in each eye. She had been wearing single vision distance spectacles full-time, and occasionally wore soft contact lenses. She was interested in more independence from wearing spectacles and contact lenses, but was not interested in refractive surgery enhancement or retreatment. After careful consideration and thorough discussion of the vision correction options, she was mostly interested in OK.
Given the complexity of these cases, it is advisable to only offer post-LASIK OK for low to moderate myopia and low corneal astigmatism, and to patients who are highly motivated
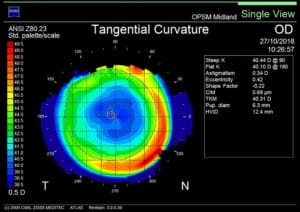
Figure 1. Corneal topography at baseline.
At her first presentation, Marilyn’s spectacle refraction was:
R: -1.75/-0.50×015 (6/4.5)
L: -2.25/-0.25×150 (6/4.5)
A thorough ocular health examination was performed, including a careful examination of the ocular surface, eyelids, ocular adnexa, and thorough posterior segment examination – all of which were healthy and unremarkable in each eye. Corneal examination showed a faint peripheral epithelial ring, consistent with the margins of the previous LASIK corneal flap, but no signs of epithelial ingrowth or corneal haze or scarring. There were no signs of contraindications to OK lens wear.
Baseline corneal topography showed no signs of corneal irregularities, such as post-LASIK ectasia, irregular astigmatism, or epithelial erosions. Multiple baseline topography scans were performed to ensure accuracy, consistency, and repeatable baseline measurements. The baseline corneal topography showed a large central zone of corneal flattening consistent with myopic LASIK correction. This was surrounded by a peripheral ring of relative peripheral corneal steepening. The central LASIK treatment zone diameter appeared to be about 5mm in each eye. At this time it was important to consider the standard optic zone diameter of the chosen OK lens design of 6.0mm, and the total lens diameter of 10.5mm.
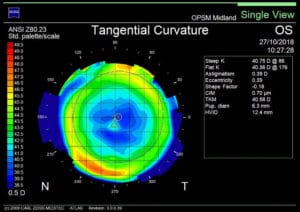
Figure 1. Corneal topography at baseline.
Analysis of the baseline corneal topography, together with manual keratometry measurements, found that the central cornea was largely regular and spherical in each eye. The results from the baseline examination showed that Marilyn was a good candidate for OK. When advised that her OK treatment may require more visits than a conventional OK fitting procedure, she remained highly motivated to proceed.
Simulated Keratometry (Corneal Topography)
R: 40.44/40.10 dioptres
L: 40.75/40.36 dioptres
Manual Keratometry
R: 39.6/39.4 dioptres
L: 39.8/39.5 dioptres
The initial OK lenses, with the following parameters, were selected for Marilyn using the provided lens selector nomogram:
R: 91/500/31
L: 91/500/31

Figure 2. Corneal topography at six month review – showing slightly superior decentred bullseye pattern in each eye.
The OK lenses were inserted, and showed good central fitting with adequate mid-peripheral pooling and edge lift in each eye. The contact lens overrefraction was +0.25 (6/6+2) in each eye. After the tutorial session, Marilyn took the lenses home to wear overnight. She was asked to return the following day for review.
ONE NIGHT REVIEW
Unaided Visual Acuities
R: (6/9-2)
L: (6/12-2)
Binocular: (6/6-2)
Refraction
R: -0.75 (6/6)
L: -0.75 (6/6)
Corneal topography showed a slightly superior decentred bullseye pattern in each eye.

Figure 2. Corneal topography at six month review – showing slightly superior decentred bullseye pattern in each eye.
ONE WEEK REVIEW
Marilyn reported no problems with OK lens wear, but she had noticed some blurred vision at the end of the day.
Unaided Visual Acuities – Morning
R: (6/7.5+)
L: (6/7.5-2)
Binocular: (6/6+2)
Refraction
R: -0.50 (6/6+)
L: plano/-0.50×160 (6/6+)
Corneal topography showed a slightly superior decentred bullseye pattern in each eye.

Figure 3. Corneal topography refractive power difference at six month review.
THREE TO FOUR WEEK REVIEW
Marilyn reported no problems with OK lens wear, with good vison, but had still noticed some blurred but adequate vision at the end of the day.
Unaided Visual Acuities – Morning
R: (6/6+2)
L: (6/6+2)
Binocular: (6/4.5)
Refraction
R: plano
L: plano
Corneal topography showed a slightly superior decentred bullseye pattern in each eye. At this stage, changing the lens parameters was considered by slightly increasing the sagittal depth of the lens to improve centration, but it was decided to continue with the lenses.
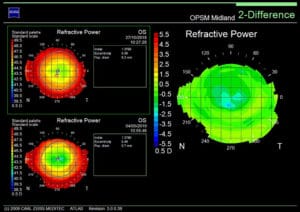
Figure 3. Corneal topography refractive power difference at six month review.
SIX MONTH REVIEW
Marilyn reported that she was very happy and satisfied with her vision and visual comfort, although she experienced some dryness and irritation in the mornings, and still noticed mild blurred vision at the end of the day.
Unaided Visual Acuities – Late Afternoon
R: (6/7.5+)
L: (6/7.5)
Refraction
R: -0.25
L: -0.25
Corneal topography showed a persistently slightly superior decentred bullseye pattern in each eye.
DISCUSSION
Modern LASIK refractive surgery remains an excellent option for myopic vision correction for many patients. It has a long, well-established history of safety with a very low complication rate.1 At the same time, it has been reported that the efficacy and predictability of this treatment option gradually reduces over time due to myopic regression. A number of studies investigating the long-term efficacy of LASIK have found that myopic regression occurs in a number of cases, especially in cases involving moderate to high levels of myopia.2,3,4
The aetiology of myopic regression following LASIK refractive surgery is not well understood, but it is thought to be multifactorial, with some proposed mechanisms involving corneal curvature changes, epithelial hyperplasia, corneal forward shift, stromal thickening, lenticular nuclear sclerosis, and axial elongation.2 A twelve-year post-LASIK follow-up study found that most eyes with moderate to high myopia showed approximately 10% regression of myopia after twelve years post-LASIK.2
Although both LASIK and OK can provide effective myopic correction in adults, there are some key differences. The corneal changes in myopic OK correction involve central epithelial thinning with a midperipheral ring of epithelial thickening.5 This reversible compression and redistribution of corneal epithelial tissue, caused by hydraulic forces of the post-lens tear layer, is the mechanism by which there is central corneal flattening and mid-peripheral corneal steepening. Stromal changes do not contribute significantly in OK. Conversely, LASIK involves the laser ablation and thinning of the central corneal stroma, which leads to relative peripheral corneal steepening. Epithelial changes do not contribute significantly in LASIK. It is also important to note that generally, the central treatment zone in LASIK is larger than with OK. A larger myopic OK refractive correction is also generally associated with a smaller treatment zone.
When considering OK lens fitting, careful patient selection and communication of visual expectations and procedures are very important. Given the complexity of these cases, it is advisable to only offer post-LASIK OK for low to moderate myopia and low corneal astigmatism, and to patients who are highly motivated. It is important to consider that most conventional OK lenses are designed to fit a normal prolate corneal shape (steeper central cornea, flatter peripheral cornea), whereas the post-myopic LASIK cornea is an oblate corneal shape (flatter central cornea, steeper peripheral cornea). This could compromise the fitting and centration of the lens, which will require more adjustments and therefore more visits.
It is unknown whether OK is effective in reducing the rate of myopia regression following LASIK in adults as it is for reducing the rate of myopia progression in children.6 For this reason, this potential benefit of OK was not discussed with the patient and has not been discussed in this article. However this may be an important topic for future study.
PRESENTING THE OPTIONS
It is important for optometrists and ophthalmologists to mutually recognise our expanding scopes of practice, and how we can offer our services to patients. In the case of post-LASIK vision correction, it is in the best interests of our patients to discuss and offer all available options. For optometrists, the options may include referral to a corneal specialist ophthalmologist for enhancement or retreatment of refractive surgery, simple distance correction with spectacles or contact lenses, or OK. This depends on the individual needs and lifestyle of the patient, while taking into consideration the costs, risks, and benefits.
*Patient name changed for anonymity.
Eden Kwok BOptom (Hons) MOptom completed his Bachelor of Optometry at the University of Auckland in 2009 and his Master of Optometry at University of New South Wales in 2014. He practices at OPSM Midland Gate in Western Australia.
References
- Aristeidou A, Taniguchi EV, et al. The evolution of corneal and refractive surgery with the femtosecond laser. Eye Vis (Lond). 2015; 2:12
- Ikeda T, Shimizu K, et al. Twelve-Year Follow-Up of Laser In Situ Keratomileusis for Moderate to High Myopia. Biomed Res Int. 2017; 2017:9391436
- Zalentein WN, Tervo TM, et al. Seven-year follow-up of LASIK for myopia. J Refract Surg. 2009; 25(3):312-8
- Alió JL, Ortiz D, et al. Ten years after photorefractive keratectomy (PRK) and laser in situ keratomileusis (LASIK) for moderate to high myopia (control-matched study). Br J Ophthalmol. 2009; 93(10):1313-8
- Kim WK, Kim BJ, et al. Corneal epithelial and stromal thickness changes in myopic orthokeratology and their relationship with refractive change. PLoS One. 2018; 13(9): e0203652
- Cho P, Cheung SW, et al. The longitudinal orthokeratology research in children (LORIC) in Hong Kong: a pilot study on refractive changes and myopic control. Curr Eye Res. 2005; 30: 71-80





