
No matter how ‘perfect’ a CL is or how well you manage the consults, we can never eliminate the limiting factor; the patient.
JC is a 35 year old female myopic astigmat who has been an avid full time contact lens (CL) wearer since the age of 13. In her mid-late teens, when silicone hydrogel lenses were first released, she wore silicone hydrogel lenses on a monthly extended wear basis however suffered several episodes of infiltrates and suspected ulcers and so reverted back to daily wear. She developed astigmatism in her 20s, and continued to wear monthly disposable CLs on a daily wear basis. She tried various daily disposable toric CLs but found them either uncomfortable and/or unstable until the CooperVision MyDay Toric was launched. She happily wore the MyDay Toric all waking hours until she began to experience end of day dryness a year ago, especially in the left eye.
she complained of extremely foggy vision… and despite advice that wearing the lens during the day could affect the treatment zone, she wore the OK lens all day so she could see
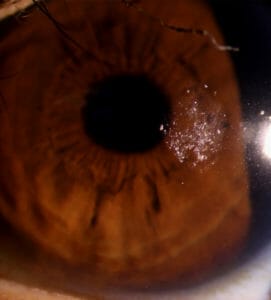
Figure 1. Poor soft contact lens wettability.
JC’s vision with her MyDay Toric CLs of prescription R -2.75/-1.75×180 and L -3.75/-0.75×180 was R 6/4.8, L 6/6+. However she reported it could vary when she was tired, after exercise or towards the end of the day, especially in the left eye.
Examination of her CLs revealed wellfitting lenses with minimal rotation, but poor surface wettability, especially in the left eye (Figure 1). Vision with her CLs was R 6/4.8, L 6/6=.
Anterior eye examination revealed inferior superficial punctuate staining L>R, and meibomian gland dysfunction. Meibography revealed meibomian gland shortening L>R (Figures 2–3). JC was advised to perform hot compresses with a Bruder Eye mask and to take DryEye Forte capsules.
JC returned multiple times, reporting the same issues. Upon questioning, she reported that she’d performed the hot compresses only twice. She had taken DryEye Forte when she remembered, however they did not help significantly. She explained that she already had a reasonable diet and ate plenty of fish.
JC had tried orthokeratology (OK) on three separate occasions years ago and having found the varying vision frustrating, had given up after a few nights each time. She vowed to never try again after she rode her bicycle into a parked car. The problem, she had been told, was that she had limbal to limbal astigmatism (Figure 4). Given the advances in OK design and technology, she was convinced to try once more.
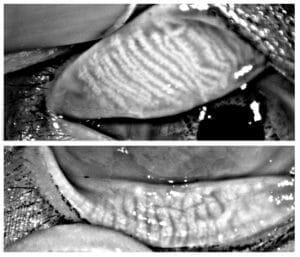
Figure 2. Right eye meibography.
JC was fitted with Innovative Forge toric OK CLs. Upon dispensing, they appeared well-fitting with minimal rotation (Figures 5–6). She only wore the left CL the first night as she wanted clear vision in at least one eye. At day one follow-up she could achieve L 6/12= however, she complained of extremely foggy vision which could not be improved with refraction. She found this very distracting, and despite advice that wearing the lens during the day could affect the treatment zone, she wore the OK lens all day so she could see. She remarked at how clear her vision was with the rigid lens optics compared to soft lenses and said the discomfort didn’t bother her as much as the blur. After day two she removed the lens and was amazed at how clear her vision was – she was able to achieve L 6/6++. Videokeratoscopy revealed a Bull’s eye treatment (Figure 7). She began wearing the right lens and again, reported terrible vision on day one, and decided to wear her lens all day. On day two, her vision was excellent. She was ecstatic and sent a long email exclaiming how grateful she was to have clear, consistent, comfortable vision and declaring that OK was life-changing.
Two days later she broke the right lens.
A new lens was ordered, and while waiting two weeks for its replacement, she wore her OK lens in the left eye and her soft daily in the right. Unfortunately she found this confusing and slept in the daily lens twice during this time; fortunately without complications.

Figure 3. Left eye meibography.
She returned to wearing her right lens as soon as it arrived and remarked at her clarity of vision by day one.
Two days later she reported she had spent ten minutes trying to get the left lens out before realising it was not there. She searched her entire house with no luck, and because she felt as if it were still in her left eye, went back to checking for it. In the process, she discovered a soft lens in her right eye – it had been there since she’d begun wearing her new right eye OK lens two nights prior.
DISCUSSION
I am an advocate for OK and have many patients in this modality. It has been shown to slow the progression of myopia in kids and teenagers,1 and because there is no lens worn during the day, it is an excellent option for patients who suffer dry eyes.2
 OK is perfect for low prescriptions because the effect is fast and lenses can often mould the eyes to the correct prescription for more than one day. This means patients may not need to wear the lenses every night, which is especially beneficial if they forget or simply cannot be bothered.
OK is perfect for low prescriptions because the effect is fast and lenses can often mould the eyes to the correct prescription for more than one day. This means patients may not need to wear the lenses every night, which is especially beneficial if they forget or simply cannot be bothered.
However when it comes to adults with a relatively high prescription and astigmatism I am wary of recommending OK. They require commitment and motivation as the lenses must be worn every night. If they don’t do this, they will not return to their baseline prescription – instead, they will end up at a prescription somewhere in between, often too blurry to manage, but at a level where their spectacles are too strong. While kids and teenagers can be very tolerant to blur, adults hate it and find it frustrating.
Patient Selection
Careful history should be taken before initiating OK with an adult to ascertain their lifestyle and visual demands – their occupation, hobbies, whether they drive long distances, and the type of person they are – are they organised, do they have routine sleep patterns etc. or do they enjoy a more haphazard existence, like JC. Sleep patterns are important to understand because fewer hours sleep means less time for the lenses to mould the cornea. It also means more hours awake so the effect needs to remain in place longer. OK is completely reversible and the effect will start to fade if the lenses are not worn. Ideally the effect will begin to fade after the lenses are reinserted.
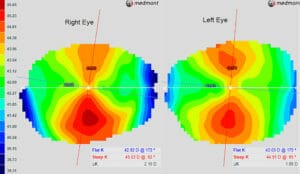
Figure 4. Right and left eye topographies.
Patients need to understand all of these potential complications before they give OK a try. I know this because the patient I write about here – JC – is in fact me.
As an optometrist and a CL patient, I have tried every type of lens I have ever fitted and so I completely understand the patient journey. Patients appreciate this – if it’s good enough for me, it must be good enough for them.
Unfortunately, while that makes me a good CL practitioner, it doesn’t make me a good CL patient – whatever a patient can do, I have done. I am very careful in warning my patients about proper use of peroxide and the need to neutralise it as it hurts. I know because I’ve done it. Three times. It really hurts. Prior to wearing daily disposables, I mixed my lenses up on many occasions. I’ve had lenses fall out of my eyes; I’ve opened my case on several occasions to find no lenses in there; I’ve put two lenses in the same eye; and I’ve walked around with one lens because I’ve had sore eyes and refused to wear my spectacles. My housemate once told me he woke up to two pairs of CLs in his case, the result of a few too many wines, we can argue over whether it was him or whether it was me, but I think we know the answer.

Figure 5. Right eye fit with an OK lens.
Kate Gifford has kindly dubbed me a ‘lovable fool’, which I think is just a euphemism for ‘idiot’. I’m absent minded, clumsy, forgetful, in a rush to do everything and a believer that I am excellent at multitasking (which evidently I am not). On top of that, I enjoy wine probably a little too much. I am also impatient, a myope who demands excellent vision, and a nightmare patient. As my good friend Tim Martin says, “accidents are the price of living life to its fullest” and even during these ‘Corona times’, I’m trying to live my best life.
With all of this in mind, I always carefully explain all the complications of OK, especially at the outset of treatment. After all, patients like me would be the type to ring every day to complain about their vision, despite careful counselling, and I find them really annoying. I do my best to fob off their phone call, hoping that by the time they get through to me their vision will be good. Unfortunately I had no one to ring or annoy.
IS OK FOR ME?
During lockdown, while some people were cooking, others getting fit, learning new hobbies, or binge watching shows, I decide to try OK. I wasn’t driving anywhere, I had nowhere to be, my workload had reduced dramatically, so I had time to devote to something new.
I really enjoyed the days of being CL free and was extremely impressed with the lenses Lachlan Hoy from Innovative Contacts kindly provided – they’re the first to have worked for my eyes. If I ever find my lens, I will persevere until I lose or break another one. However, having everted my eyelid several times in the hope it might be magically stuck somewhere, torn my entire house apart trying to find the damn thing, had many moments of near excitement as I found multiple dried up CLs scattered around my room, and having written this article with just one eye seeing, I’m not sure OK is for me. It’s been a challenging day. This really does highlight the importance of having a spare lens, and for individuals like myself, perhaps a couple of them.

Figure 6. Left eye fit with an OK lens.
Manufacturers have been striving for years to create the perfect CL, however unfortunately, no matter how ‘perfect’ a CL is, the limiting factor can never be eliminated – the patient. For this reason, I remain an avid daily disposable CL prescriber, they are almost idiot proof.
I hope you have enjoyed this true insight into the trials and tribulations of a CL patient, from the perspective of both patient and practitioner… and that by the time this hits your desk we will be able to see each other again at a meeting or conference so you can laugh with (and please not at!) me. Until then, stay safe and sane, and does anyone want to be my optometrist?
Thank you to CooperVision and Innovative Contacts for providing my contacts and sincere apologies for not taking more care, and thank you to Tim Martin and Laura Romeo for taking my images because as I’ve also learnt, it’s difficult to take slit lamp photos and meibography of your own eyes.
Jessica Chi is the director of Eyetech Optometrists, an independent specialty contact lens practice in Melbourne. She is the current Victorian, and a past national president of the Cornea and Contact Lens Society, and an invited speaker at meetings throughout Australia and beyond. She is a clinical supervisor at the University of Melbourne, a member of Optometry Victoria Optometric Sector Advisory Group and a Fellow of the Australian College of Optometry and the British Contact Lens Association.
References
- Sun Y, Xu F, Zhang T, et al. Orthokeratology to control myopia progression: a meta-analysis. PLoS One, 2015 April 9;10:e0124535
- Lipson MJ, Sugar A, Musch DC. Overnight corneal reshaping versus soft disposable contact lenses: visionrelated quality-of-life differences from a randomized clinical trial. Optom Vis Sci. 2005;82:886-91.





