
Diabetic retinopathy is one of the biggest threats to vision in our society. Community education, along with new technologies and treatments, will help stem the rising tide.

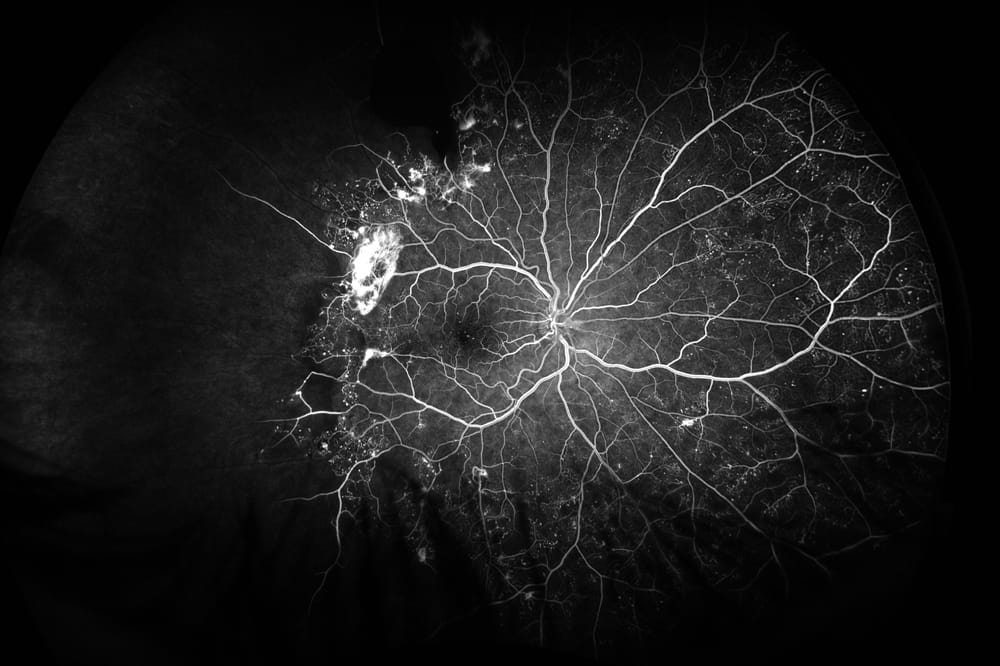
Ultra-wide field fluorescein angiography of a patient with extensive peripheral ischaemia due to diabetes. The temporal capillary non-perfusion and retinal neo-vascularisation are clearly demonstrated.
It is apt that in the year 2020 governments, health care workers and the public turn their sights to one of the biggest threats to vision in our society – diabetic retinopathy (DR). Like Dr James Muecke, I will focus much of the discussion in this article on type 2 diabetes mellitus (T2DM) due to the rapidly rising numbers of the condition and the more readily preventable and treatable nature of the disease. We have all been made aware of the staggering numbers concerning T2DM. Approximately 1.7 million Australians have the disease – and 280 new diagnoses are made in our country every day. If we continue at the current rate of disease incidence, there will be an estimated 2.5–3 million Australians living with the disease by 2025.1 We also know that sadly, Indigenous Australians are three times more likely to be diagnosed with T2DM in their lifetime than non-Indigenous patients – this number may in fact be higher for those living in remote communities. It is the fastest growing chronic condition in Australia and costs the government and the tax payer approximately six billion dollars per annum.2 Due to the rising incidence of the condition, all health care workers are now seeing the long term effects of the disease if poorly controlled. This is all too apparent for optometrists and ophthalmologists charged with the eye health care of these patients.
It is the fastest growing chronic condition in Australia and costs the government and the tax payer approximately six billion dollars per annum
In a report co-published by the Baker IDI and Diabetes Australia in 2012, it was estimated that only half of all Australians living with T2DM had adequate control. Good control means that a patient’s HbA1C is under 7.5. Glycosylated haemoglobin (HbA1C) is a blood test performed every three to six months to give an idea of the patient’s ‘average’ level of control of their blood sugars over the preceding period. Poor control over a long period leads to the end stage complications of the disease we are all familiar with. For the eye, this may mean one of, or a combination of, proliferative diabetic retinopathy and diabetic macular oedema (DME). Sadly in Australia, DME is now the leading cause of blindness in working age adults. As Dr Muecke said in his article, published in this issue of mivision, the time to act is now.
DETECTION AND SCREENING
When a patient is diagnosed with T2DM they require a baseline eye examination. Subsequently, National Health and Medical Research Council (NHMRC) guidelines state that all diabetics must have a detailed eye examination every one to two years. The frequency of review naturally increases with increasing disease severity – meaning that the worse the disease, the more frequent the review. Initial testing and review can be safely done by optometrists. Referral to an ophthalmologist is only necessary if there is treatable disease or some question around the findings at the baseline examination.
When we think of DR, it can be broadly divided into central disease (DME) or peripheral disease (background retinopathy). Fortunately, we have a huge array of imaging modalities that aid in the screening and detection of DR at our disposal. Each optometry and ophthalmology practice is set up slightly differently, but by and large the necessary tools are accessible if required. After a thorough clinical examination, optical coherence tomography (OCT), OCTAngiography (OCT-A) and fluorescein angiogram form the mainstay for diagnosis and tailoring of treatment for DR. Each are performed depending on the patient’s presentation. Here, I provide an update on how each is used and the future of imaging within our practices.
OCT and OCT-A
To say that OCT has transformed the way we practice would be an understatement. We now rely on OCT for not only diagnosis of DME but for treatment planning and prognosis. Like in many ophthalmology practices, all newly referred diabetics referred to my practice have a baseline OCT. This allows me to plan their treatment and prognosticate. There are many papers looking at OCT biomarkers as a way of predicting DME response to treatment with either anti- VEGF or steroid injections. Suggestions for useful biomarkers have included ellipsoid zone (EZ) integrity,3 external limiting membrane structure,4 presence of disruption of the inner retinal layers (DRIL),5 or hyperreflective foci6 among others.
These have all been postulated to predict visual outcomes in DME. However, there is no single OCT biomarker that allows us to accurately predict a patient’s response to treatment or their final visual acuity. Certainly, patients who have an intact EZ tend to have better visual acuity than those patients who have a disrupted EZ line.7 Greater central retinal thickness (CRT) at baseline means patients have greater potential for total reduction in retinal thickness due to the ‘ceiling effect’ of patients who start with a thinner CRT. Certainly, baseline CRT and the presence of subfoveal fluid can be a predictor of a good anatomical response to treatment – meaning that there can be more significant reduction in fluid if there is more to begin with.8 This does not necessarily correlate with better final acuity. Even prior to the use of anti-VEGF agents for the management of DME, the DRCR.net looked at OCT parameters in one of their early studies to see if they could predict final visual acuity after laser treatment.9,10 The purpose was to understand whether developing a 10-step scale for the severity of DME on OCT could predict changes in macular thickness or visual acuity after the laser treatment. No such predictable correlation could be made.11 When anti-VEGF agents became a mainstay of treatment for DME in the mid-nineties, the DRCR Retina Network once again looked to find whether OCT parameters correlate with visual acuity. One study tried to identify factors that predicted treatment success or failure in DME patients receiving ranibizumab for their disease.12 They found baseline retinal thickness was the strongest predictor of anatomical outcomes.
Another study looked at hyper-reflective foci (HRF) in the outer retinal layers as a biomarker on OCT in patients receiving ranibizumab for DME. HRF appear as highly reflective dots on spectral domain (SD) OCT. Some research suggests they represent focal vascular hyper-permeability.12 Depending on their location, they may predict good or bad visual outcomes.13 This study looked at the change in HRF in the outer retinal layers over time with anti-VEGF therapy. They found, in a multivariate analysis of retrospective data, that HRF in the outer retinal layers was correlated with improvement in BCVA at 12 months after pro ne rata anti-VEGF therapy.14
One of the most important recent studies to shape practice for DME management has been the DRCR Retina Network Protocol V study. The results were released at the Association for Research in Vision and Ophthalmology (ARVO) Conference in 2019 and subsequently published in the Journal of the American Medical Association.15 The study took the relatively common clinical scenario of patients with good visual acuity (defined as 6/7.5 or better) and central DME on OCT and randomised them to three different treatment regimens – aflibercept, focal laser or observation. Patients could have ‘rescue’ aflibercept if they worsened from a visual acuity stand point or on OCT. The results were promising – after two years follow up there was no difference in visual acuity outcomes for the 702 participants. The mean visual acuity for all groups was 20/20 and only 25% of laser patients and 30% of observation patients needed rescue aflibercept for worsening vision.15 This has allowed ophthalmologists to take a more conservative approach when dealing with patients with good vision and central DME. Clearly this is an important study and one that relies completely on disease monitoring with OCT – an unthinkable scenario 15 years ago without anti-VEGF and our current imaging modalities.
Irrespective of the nuances of OCT biomarkers, the test certainly allows the ophthalmologist to monitor treatment response and determine the frequency of injections required using guidelines such as those investigated in various randomised control trials undertaken by groups like the DRCR Retina Network – a research group dedicated to the investigation of retinal diseases.
OCT-A in Non-proliferative Diabetic Retinopathy
Traditional grading methodology for DR, using systems such as the modified Airlie House Classification model, requires the trained observer to note the rather indirect signs of microvascular ischaemia such as retinal haemorrhages, cotton wool spots or neovascularisation. With modern imaging modalities it is possible to observe ischaemic complications of diabetes in the eye even before they become clinically apparent. OCT-A allows a detailed study of diabetic microangiopathy which can be useful for both disease monitoring and treatment planning. OCT-A uses multiple OCT images compiled to isolate those areas that consistently produce a back scattering of light, such as the movement of red blood cells through vessels. Therefore, it provides us with a ‘flow’ image and not a ‘leak’ image. This allows a detailed look at capillary non-perfusion and neovascularisation. The imaging is now so sophisticated that we can segment the blood supply of the retina using OCT-A into deep and superficial capillary plexuses, as well as the choriocapillaris and deeper choroid.
The hope is that OCT-A and the quantifiable data it produces may be able to help us predict patients who are at risk of progressing to proliferative disease (and therefore require closer monitoring) and the anticipated response to anti-VEGF therapy
Several studies have looked at OCT-A images in patients without clinical signs of DR and shown that there are still significant microvascular changes present despite absence of the tell-tale signs of the disease on fundus photography or at slit lamp examination. One study showed that the foveal avascular zone was larger in both the superficial and deep capillary plexuses of diabetic patients with no clinical disease compared to non-diabetic controls.16 Another study showed that foveal vessel density was less in diabetic patients, even without clinical disease, than in non-diabetics.17 The utility of these findings may be in assessing the risk of progression in these patients to clinical disease. Certainly, the data lends itself well to potential artificial intelligence algorithms for automated processing of OCT-A imaging as a way of screening in the future. Perhaps patients with high risk changes on OCT-A will be able to be identified and therefore sent for more frequent review to prevent vision loss associated with late presentations.
For patients who have established DR and visible clinical disease, OCT-A provides useful insights to disease severity. Retinal perfusion can be quantified using OCT-A, and groups have looked at the ‘capillary perfusion index’ as a way of doing this. This is defined as the percent coverage of functional retinal capillaries within the traditional early treatment diabetic retinopathy study (ETDRS) zones.18 One study has shown a significantly lower perfusion index in the extra-foveal area of patients with more severe clinical DR compared to those with less severe disease. This suggests a correlation between capillary perfusion and the severity of DR.18
The hope is that OCT-A and the quantifiable data it produces may be able to help us predict patients who are at risk of progressing to proliferative disease (and therefore require closer monitoring) and the anticipated response to anti-VEGF therapy. There are some limitations to the technology. In patients with non-centre involving macular oedema, in whom focal laser may be more appropriate than anti- VEGF therapy, OCT-A may not be as good as a traditional angiogram for management planning. This is primarily because OCT-A may not show all of the microaneurysms present and does not show leakage patterns – both of which are useful parameters when planning focal laser.19
OCT-A in Proliferative Diabetic Retinopathy
The amount of capillary non-perfusion seen on OCT-A is correlated to the risk of conversion to proliferative disease. One study has shown a correlation between the size of the foveal avascular zone, vessel density and the percentage area of non-perfusion by comparing eyes with non proliferative diabetic retinopathy (NPDR) to eyes with PDR.20 Another study looked at the role of widefield OCT-A in disease monitoring and classification for DR.21 They examined 12 x 12mm2 OCT-A segments for large vessels, capillaries and areas of drop out for patients with all stages of the disease. Arguably, peripheral perfusion assessment is more important to monitor for risk of PDR conversion than that of central macular ischaemia. This study found that widefield OCT-A imaging may be useful in detecting capillary nonperfusion in diabetic eyes and thus have some utility in monitoring for disease progression in high risk patients.21
Advances in Fluorescein Angiography
Fluorescein angiography (FA) was once performed on nearly all diabetics to confirm areas of non-perfusion, the presence of proliferative disease and leakage from macular oedema. With the advent of OCT, FA is now less commonly performed. Its usefulness may be on the increase again with ultra-widefield (UWF) FA, which allows angiography to be performed out to 100° or more. This is in contrast to the original ETDRS standardised, seven field, 30° fundus photography concentrating on the posterior pole. UWF-FA has been shown to be more sensitive in detecting PDR than 30° fundus photography.22 In one study, over 10% of diabetic eyes had areas of neovascularisation that were outside the traditional 30° zone.22 In addition, compared to the ETDRS standard FA, UWF-FA has been shown to be able to detect more areas of nonperfusion and more clusters of neovascularisation elsewhere (NVE).
widefield OCT-A imaging may be useful in detecting capillary nonperfusion in diabetic eyes and thus have some utility in monitoring for disease progression in high risk patients
These findings have been successfully used for prognostication. One study showed that eyes that had predominantly peripheral areas of nonperfusion on UWF-FA (defined as outside the standard 30°) had an increased risk of disease progression and conversion to PDR over four years.23
The findings on UWF-FA have also led to the increasing use of image-guided retinal laser photocoagulation. This means that laser is only applied to the areas of nonperfusion seen on UWF-FA, which differs from conventional pan-retinal photocoagulation where all areas of the retina outside the arcades are lasered to induce new vessel regression. There have been various studies to show that like pan-retinal photocoagulation, UWF-FA guided laser is effective in treating PDR but allows only the areas of retina affected to be treated.24,25
The DRCR Retina Network has been pivotal in designing trials that have shaped practice around the management of DR. One current study underway known as Protocol AA is a prospective, observational, longitudinal study that aims to investigate whether UWF imaging, compared to standard ETDRS fields, allows improved assessment of DR and its progression over time. Certainly any positive findings may lead to a change in the way we grade severity in DR.
FUTURE TREATMENT OF DIABETIC RETINOPATHY
For more than 20 years the DRCR Retina Network has undertaken studies that have allowed significant advancement in our understanding of best practice for DR treatment. Protocol S allowed us to compare standard of care panretinal photocoagulation with intravitreal ranibizumab for treatment of PDR. Protocols I, T and V have allowed a thorough examination of management of DME with laser, anti-VEGF or steroid. DRCR Retina Network has defined treatment protocols for DME and given us the tools to best use the imaging modalities available to us all in our everyday practice in order to best manage the disease.
Novel imaging modalities, new pharmacological agents and greater public awareness will ideally allow for improved patient outcomes for all our diabetic patients
DRCR Retina Network now has a number of studies either underway or about to commence to answer further important clinical questions about management of DR. These include Protocol W, which is looking at prevention of vision threatening DR with anti-VEGF therapy in eyes at high risk of progression. They will also report on Protocol TX, which is an extension study of the pivotal Protocol T study that compared head to head aflibercept, ranibizumab and bevacizumab for the treatment of DME.
There have been other recent advances with potential new treatment options for DR in particular for DME. Many of you will have heard of brolucizumab (Beovu) which was recently launched for the treatment of neovascular AMD (nAMD). Beovu is a single-chain antibody fragment and is thought to have better tissue penetration due to its small size compared to other anti- VEFG agents.26,27 It is a potent inhibitor of all VEGF-A isoforms and, given the success of other anti-VEGF agents in crossing over from treatment of nAMD to DME, Novartis instigated the KITE and KESTRAL studies. These are ongoing, prospective, randomised, Phase III clinical studies looking at aflibercept 2mg head to head with brolucizumab 6mg from a functional and morphological perspective over two years for the treatment of DME.
There are other promising novel pharmacological options in the pipeline for treatment of DME. Roche and Genetech recently published results of the phase II BOULEVARD study which compared the novel molecule faricimab to ranibizumab for the treatment of DME. Faricimab is a bispecific antibody that binds to and inhibits both VEGF-A and Angiopoietin-2 (Ang-2). Angiopoietins are an important group of growth factors and their functions are, in part, controlled by the tyrosine kinase receptors Tie 1 and Tie 2. The angiopoietin/Tie signalling pathway is vital for normal angiogenesis. Angiopoietin-1 (Ang-1) is responsible for angiogenesis and signals through Tie2. Ang-2 has antagonistic activity, also through the Tie2 receptor. Deregulation of Ang-2 has been shown to be important in many diseases. Ang-2 expression is induced in endothelial cells by inflammatory mediators such as thrombin28 and conditions such as hypoxia29 and as such is an important factor in the development of vascular related disease such as DR. Given this, targeting of the Ang/Tie pathway is an exciting new therapeutic possibility.
The results from the BOULEVARD study showed that faricimab was superior to ranibizumab in visual acuity gains and anatomic outcomes on OCT. The study met its end point as there was a statistically significant improvement in best corrected visual acuity (BCVA), DR severity scores (DRSS) and extended durability in treatment naïve DME patients treated with faricimab versus ranibizumab. These findings, from the phase 2 studies, indicate there may be a role for inhibition of both Ang-2 and VEGF-A in centre-involving DME. As such, faricimab is currently being studied in two phase III, multi-centre, randomised clinical studies for DME – the YOSEMITE and RHINE studies, which have now completed enrolment.
CONCLUSION
We live in an exciting era for both evolving diagnostic tools and management of DR. Novel imaging modalities, new pharmacological agents and greater public awareness will ideally allow for improved visual outcomes for all our diabetic patients. There does need to be increased acknowledgment by health advocates (such as us) and government as to the contributors to the increasing incidence of T2DM in our community if we are to prevent visual loss from the disease in our patients. I have no doubt that we will be able to achieve this if we continue to work together and put the patient first in the discussion.
Dr Amy Cohn is a Melbourne based ophthalmologist with special interest in medical retina and cataract surgery. She is on the RANZCO Scientific Committee as well as being a Visiting Medical Officer at RVEEH and a Senior Research Fellow at the Centre for Eye Research Australia. Dr Cohn sees patients privately in East Melbourne, Footscray, Glen Waverley and Armadale.
To earn your CPD points from this article answer the assessment available at mieducation.com/ diabetic-retinopathy-stemming-the-rising-tide
References
- Magliano DJ PA, Vos T, et al. Projecting the burden of diabetes in Australia– what is the size of the matter? 2009;Aust N Z J Public Health(33):540-3.
- Colaguiri S CR, Conway B, et al. DiabCo$t Australia: Assessing the burden of Type 2 Diabetes in Australia. 2003.
- Tao LW WZ, Guymer GH, et al. Ellipsoid zone on optical coherance tomography: a review. Clin Exp Ophthalmol 2016;44:422-30.
- Muftuglou IK MN, Gaber R, et al. Integrity of outer retinal layers after resolution of centre involved diabetic macula oedema. Retina 2017;37:2015-24.
- Sun JK LM, Lammer J, et al. Disorganization of the retinal inner layers as a predictor of visual acuity in eyes with center-involved diabetic macular edema. . JAMA Ophthal 2014;132:1309-16.
- Vujosevic S TT, Bini S, et al. Imaging retinal inflammatory biomarkers after intravitreal steroid and anti-VEGF treatment in diabetic macular oedema. Acta Ophthalmol 2017;95:466-71.
- Santos AR CM, Schwartz C, et al. . Optical coherence tomography baseline predictors for initial best-corrected visual acuity response to intravitreal anti-vascular endothelial growth factor treatment in eyes with diabetic macular edema: the CHARTRES study. . Retina 2018;38:1110-9.
- Campos A CE, do Carmo A, et al. . Evaluation of markers of outcome in real-world treatment of diabetic macular edema. Eye and Vision 2018;5.
- Writing Committee for the Diabetic Retinopathy Clinical Research Network. FD, Strauber SF, Aiello LP, et al. Comparison of the modified Early Treatment Diabetic Retinopathy Study and mild macular grid laser photocoagulation strategies for diabetic macular edema. Arch Ophthalmol 2007;125:469-80.
- Network DRCR. Association of the Extent of Diabetic Macular Edema as Assessed by Optical Coherence Tomography with Visual Acuity and Retinal Outcome Variables. Retina 2009;29:300-5.
- Bressler SB QH, Beck RW, et al. Factors Associated with Changes in Visual Acuity and OCT Thickness at 1 Year after Treatment for Diabetic Macular Edema with Ranibizumab. Arch Ophthalmol 2012;130:1153-61.
- Bolz M S-EU, Deak G, et al. Optical coherence tomographic hyperreflective foci: a morphologic sign of lipid extravasation in diabetic macular edema. Ophthalmology 2009;116:914-20.
- Uji A MT, Nishijima K, et al. Association between hyperreflective foci in the outer retina, status of photoreceptor layer, and visual acuity in diabetic macular edema. Am J Ophthalmol 2012;153:710-7.
- Yoshitake T MT, Susuma K, et al. Hyperreflective Foci in the Outer Retinal Layers as a Predictor of the Functional Efficacy of Ranibizumab for Diabetic Macular Edema. Sci Rep 2020.
- Baker CW GA, Beaulieu WT, et al. Effect of initial management with aflibercept vs laser photocoagulation vs observation on vision loss aming patients with diabetic macula oedema involving the centre of the macula and good visual acuity: a randomised clinical trial. JAMA 2019;321:1880-94.
- Takase N NM, Kato A, et al. Enlargement of foveal avascular zone in diabetic eyes evaluated by enface optical coherence tomography angiography. Retina 2015;35:2377-83.
- Dimitrova G CE, Takahashi H, et al. Quantitative retinal optical coherence tomography angiography in patients with diabetes without diabetic retinopathy. Invest Ophthalmol Vis Sci 2017;58:190-6.
- Lin AD LA, Zhang Q, et al. . Association between OCT based microangiography perfusion indices and diabetic retinopathy severity. Br J Ophthalmol 2017;101:960-4.
- Parravano M DGD, Scarinci F, et al. . Diabetic microaneurysms internal reflectivity on spectral-domain optical coherence tomography and optical coherence tomography angiography detection. Am J Ophthalmol 2017;179:90-6.
- Nesper PL RP, Onishi AC, et al. . Quantifying microvascular abnormalities with increasing severity of diabetic retinopathy using optical coherence tomography angiography. . Invest Ophthalmol Vis Sci 2017;58:BIO307- BIO15.
- Tan B CJaLE. Quantitative Microvascular Analysis With Wide-Field Optical Coherence Tomography Angiography in Eyes With Diabetic Retinopathy. JAMA Ophthal 2020(3).
- Talks SJ MV, Steel DH, et al. New vessels detected on wide-field imaging compared to two-field and seven-field imaging: implications for diabetic retinopathy screening image analysis. Br J Ophthalmol 2015;99:1606–9.
- Silva PS CJ, Haddad NM, et al. Peripheral lesions identified on ultrawide field imaging predict increased risk of diabetic retinopathy progression over 4 years. Ophthalmology 2015;122:949–56.
- Muqit MM MG, Henson DB, et al. . Optosguided pattern scan laser (Pascal)-targeted retinal photocoagulation in proliferative diabetic retinopathy. Acta Ophthalmol. Acta Ophthalmol 2013;91:251–8.
- Reddy S HA, Schwartz SD. Ultra wide field fluorescein angiography guided targeted retinal photocoagulation (TRP). . Semin Ophthalmol 2009;24:9-14.
- Nimz EL ea. Intraocular and systemic pharmacokinetics of brolucizumab (RTH258) in nonhuman primates. . The Association for Research in Vision and Ophthalmology (ARVO) annual meeting2016.
- Gaudreault J ea. Preclinical pharmacology and safety of ESBA1008, a single-chain antibody fragment, investigated as potential treatment for age related macular degeneration. . ARVO Annual Meeting2016.
- Huang YQ LJ, Hu L, et al. Thrombin induces increased expression and secretion of angiopoietin-2 from human umbilical vein endothelial cells. Blood 2002;99:1646-50.
- Kelly BD HS, Hirota K, et al. Cell type-specific regulation of angiogenic growth factor gene expression and induction of angiogenesis in nonischemic tissue by a constitutively active form of hypoxia-inducible factor 1. Circ Res 2003;93:1074-81.Ultra-wide field fluorescein





