
Over the years technology and techniques used for laser vision correction have come a long way, yet there’s still further to go. Artificial intelligence and machine learning are on the near horizon.
As one of the first ophthalmologists to have laser vision correction (LVC) in Australia and specifically do a Fellowship overseas in refractive surgery, I was considered by my peers as somewhat progressive back in 2004. Much has changed for the better. Certainly, the modern-day laser patient can expect increased accuracy and safety due to better screening for suitability and advanced laser technology. A patient in 2020 also has a much more comfortable experience due to faster lasers, reduced suction pressure and better medication. I remember quite vividly the feeling of being almost pinned to the laser table and my vision blacking out from the high suction pressure of the early femtosecond lasers. It was not unusual to have a subconjunctival haemorrhage afterwards that lasted for a few weeks and I routinely would warn patients of this. Nowadays, it is very rare to have patients mention the pressure feeling at all and often they will comment on how much easier the experience was than expected.
SMILE laser eye surgery potentially may improve the effective size of the treatment zone as, unlike excimer lasers used in LASIK and PRK, it does not have the issue of peripheral reflectance of the laser rays
 ADVANCES IN SAFETY: ECTASIA/KERATOCONUS
ADVANCES IN SAFETY: ECTASIA/KERATOCONUS
Ectasia or keratoconus after LVC in the mid to late 2000s was one of the most feared complications of LVC and is therefore a good framework in which to highlight safety advances. A rush of retrospective research followed early cases of what was felt to be a “most surprising complication”.1-5 As the lead author of one of the larger studies, and due to my early involvement in collagen crosslinking, I found myself in quite a bit of demand as a speaker at conferences with concerned eye surgeons eager to learn anything that could help avoid and treat this complication. It became generally agreed that there were a number of risk factors for ectasia: abnormal topography, higher laser corrections, younger age, and a family history of keratoconus. Ectasia can occur early or late, with a median time of around four years. The actual incidence pre-2010 was reported to be anything from 0.04–0.6%, however it was thought to be under-reported.6
Fast forward to 2020, and the presence of risk factors for ectasia is still the number one reason in my practice (and most others) why I would recommend against LVC. However, while there are no large data sets to absolutely confirm this, my perception is that the incidence of ectasia appears to be lower now. Bohac et al’s large retrospective review of 30,000 patients between 2007 and 2015 found an incidence of ectasia of 0.033%.7 The reduced incidence is most likely multi-factorial: more accurate and stronger healing flaps can be achieved with the femtosecond laser as opposed to a microkeratome (blade); we have better topographic screening and we tend to be more conservative in case selection. Crosslinking has also been shown to be an effective treatment to stop further progression of post LASIK ectasia.8,9 Increased adoption of SMILE laser eye surgery may be another factor going forward, which reduces ectasia incidence. Experimental studies show that it has potentially less structural impact on the cornea than LASIK but this has not yet been borne out in any clinical studies.10
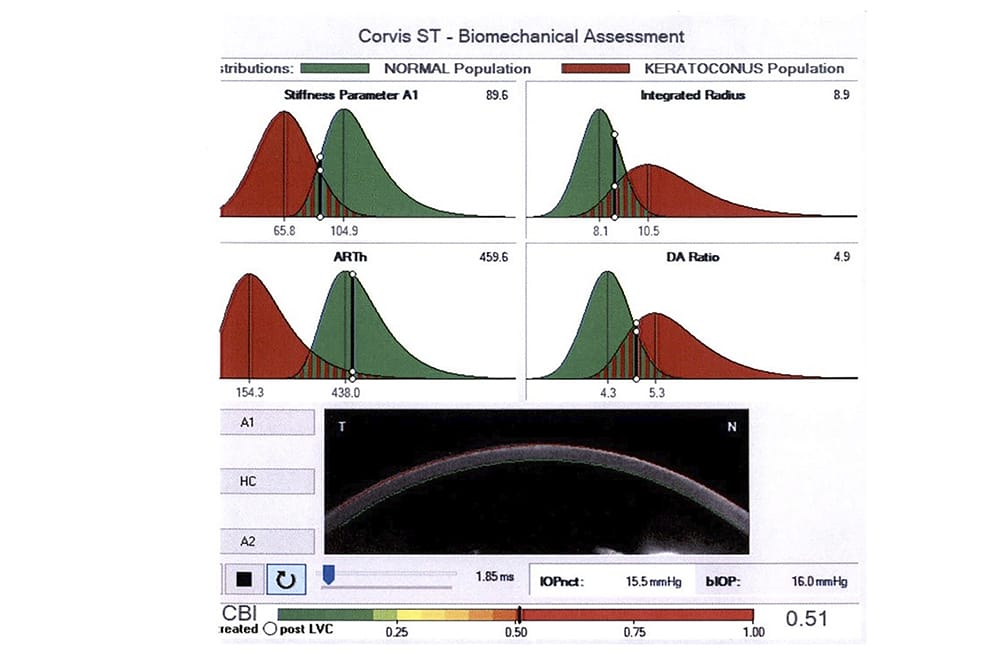
What is really lacking to potentially eliminate ectasia as a complication is an instrument which reliably assesses biomechanical strength of the cornea and big data/registries to map the incidence and risk factors for keratoconus in the population. Currently the assumption in refractive surgery screening is that shape or topography and thickness reflect strength but I tell patients that this is the mental equivalent of assessing a building’s structural integrity, on how straight and wide it is. A number of novel devices to measure corneal biomechanical strength, including the Ocular Response Analyser and CORVIS,11,12 have emerged. These devices do show reasonable repeatability and reliability on measurements with normal eyes and significant differences in indices with keratoconic eyes. However, the refractive surgery candidates where these devices are most needed are in the so-called ‘normal eye’, which shows only very mild or no topographic changes suggestive of keratoconus. To date, these devices do not appear to have the sensitivity to differentiate between normal and slightly abnormal corneas (Figure 1).
Tear osmolarity is a relatively new player in the dry eye screening process… Variability in measurements and inter-eye variability has also been shown to be an indicator of dry eye disease
Artificial intelligence (AI) and machine learning approaches, with big data, may provide another potential way to greater safety and better screening of refractive candidates. Already data-based algorithms are employed in modern topographic screening. At Vision Eye Institute we use the Belin−Ambrósio Enhanced Ectasia Display (BAD-D) index as an additional screening method. This data-based algorithm gives a number of indices which suggest how normal or abnormal a cornea is. In my experience, and based on the studies performed, the BAD-D index is a useful but imperfect additional tool to the surgeon-based clinical decision making process.13 On a small number of occasions, the BAD-D index has failed to identify patients with topographically obvious forme fruste keratoconus.
The next step beyond these instrumentbased algorithms will be multiple input algorithms based on big data. Yoo et al proposed adopting machine learning to automatically identify candidate patients for corneal refractive surgery.14 Using the somewhat cute and aptly named ‘random forest’ machine learning approach, the Korean Eye Centre used a patient database of 18,480 patients and ‘expert’ eye surgeons to train the machine learning model. The random forest approach is based on the premise that one decision ‘tree’ is not as good as multiple decision ‘trees’ which are randomly uncorrelated with each other. If you find that confusing, maybe ‘you can’t see the forest for the trees?’… Think of it this way, it is essentially a decision by committee but the members of the committee have no direct relationship with each other, which means they are more likely to come up with an unbiased and objective answer. Of course, one of the issues with machine learning using big data is validation and the study conducted had a short follow up of less than two years. We know ectasia can take longer to develop than that. It is exciting, however, to think that one day I will be replaced by a machine and therefore, I will be able to stay in my pyjamas all day.
ACCURACY
A recent audit of our data at Vision Eye Institute shows an enhancement rate of 1.8% across all laser surgeries and across all degrees of refractive error, low and high. This is a far cry from what was commonly reported back in the early 2000s. One large study in 2004 reported an enhancement rate of 14%.15 Like the reduction in haloes and improved quality of vision, wavefront customised ablation led a charge to much improved accuracy due to larger treatment zones, which resulted in less regression and better tracking. This in turn achieved better correction of astigmatism in particular. However, larger corrections continued to be the main predictive risk factor for requiring an enhancement. A 10-year prospective audit of LASIK outcomes for myopia in 37,932 eyes at the Singapore National Eye Centre demonstrated this issue very well (Figure 2).16 Larger corrections take longer, and the exposed cornea during laser-assisted in situ keratomileusis (LASIK) or photorefractive keratectomy (PRK) becomes progressively dehydrated, leading to more effective tissue removal and overcorrections.

Figure 1. Corvis printout suggesting lower biomechanical strength in a normal cornea.
While faster excimer lasers compensate for this – quite simply by being faster – SMILE gets around this completely by creating a refractive lenticule in a closed system, so that there is no dehydration or exposure during the ablation. Theoretically this means that it should be as accurate for -1.00 as it is for -10.00. A number of studies demonstrated the increased accuracy of SMILE in higher myopia at the time of its introduction but, as excimer lasers have continued to get faster, this advantage may be diminishing. The primary main advantage of SMILE then becomes less dry eye compared to LASIK.17-25 Dry eye is one of the most common reasons for dissatisfaction after LVC and the higher the correction, the higher the risk of more severe and prolonged dry eye.
To my knowledge there is yet to be a laser centre which can claim a 0% enhancement rate, even with highly experienced surgeons (another predictive factor for accuracy) and after nomogram adjustment and auditing of results (another factor in enhancement rates).26,27,28
I have been impressed with the accuracy of transPRK and most studies show similar accuracy and efficacy to LASIK and SMILE.29-31 With its minimal touch nature, I will suggest it to some of my patients based on so-called soft refractive suitability criteria such as photosensitivity, inability to keep still or keep eyes open, small palpebral apertures and general anxiety about the laser correction process. The reduced surgical component also has the potential to minimise variability in technique and therefore increase accuracy. TransPRK means that the removal of epithelium, which is normally performed by a combination of chemical (alcohol) and manual methods, is instead performed by the excimer laser and in a way that seamlessly transitions to the refractive correction as well. The issue with PRK in the past was discomfort and slower healing time but with modern bandage contact lenses, transPRK and better post-op medication, discomfort is far less of an issue. This means that the healing time is really only the main factor. My colleague, Professor Gerard Sutton’s ifix pen (Figure 3) offers a glimpse at the future as this holds the possibility of speeding up epithelial healing by delivering a 3D printed structure onto the cornea. More rapid healing would not only speed up visual recovery but reduce the incidence of haze as a potential complication.
I know I appear to be a big proponent of AI and machine learning, but I am very confident that it will play a role in further reducing the chance of a patient needing an enhancement in the future. With this in mind, imagine my delight when I was recently leafing through some research and uncovered yet another random forest machine learning study. Achiron et al built a 6000 ‘decision tree forest’ for their study into predictive factors for enhancement using over 17,000 cases.32 Analysis revealed significantly decreased efficacy with increased age, central corneal thickness, mean keratometry and preoperative best corrected visual acuity. However, the most important outcome of the study was the ability to model each individual patient’s unique risk of enhancement based on multiple clinical factors in an incremental way.
HALOES AND NIGHT VISION
Disabling haloes and poor night time vision after laser surgery made not only medical headlines but mainstream media headlines in the early to mid-2000s. It seemed to be an issue with a fairly simple cause: large pupils with large corrections and a small treatment zone along with inferior laser tracking mechanisms were resulting in decentred laser ablations, which did not make for a good outcome. However, for years later, the debate continued to rage.33 The advent of wavefront laser guided surgery in 2005 somewhat inadvertently went a large way to solving the issue. While the primary purpose of wavefront technology was to reduce the induction of higher order aberrations, like spherical aberration and coma, practically it meant a larger treatment zone with better tracking and centration which was applied universally whether you had a small pupil or a large one. Since that era, it has become increasingly rare to hear patients complain of bad haloes after laser eye surgery. One issue with wavefront customised laser though, was the increased amount of tissue removed compared to a standard treatment. Nowadays most treatments are done using a modified version called wavefront optimised, which primarily aims to minimise spherical aberration with a purer and larger treatment zone.34-38 SMILE laser eye surgery potentially may further improve the effective size of the treatment zone as, unlike excimer lasers used in LASIK and PRK, it does not have the issue of peripheral reflectance of the laser rays.39,40
My bold prediction for the future of presbyopia correction is that it will be non-surgical and definitely non-corneal… Presbyopia correcting eye drops hold the most promise at present
Certain patients will still express mild issues with poorer night vision or haloes and, in these patients, there is not necessarily a correlation between the treatment and pupil size. Neural processing no doubt plays a role in patients’ perception of haloes and a more oblate or flattened cornea cannot be expected to have as perfect vision as someone naturally emmetropic.33 Little further research has gone into understanding the small proportion who still experience haloes, maybe somewhat reflecting the lower incidence of haloes as an issue with modern laser vision correction.
DRY EYE
Dry eye after laser eye surgery remains one of my life mysteries. Standardised tear osmolarity, a dry eye questionnaire (OSDI), tear film break time testing and corneal staining with fluorescein are integral parts of screening, in my practice and in modern refractive practices. However, a small but significant cohort of patients still have dry eye to an unexpected degree. Tear osmolarity is a relatively new player in the dry eye screening process and there is still some debate as to its utility, even though it is accepted that hyperosmolarity is a key aspect of dry eye pathogenesis. Currently, 308 mOsm/L is considered to be a widely accepted threshold and the 316 mOsm/L threshold is believed to be able to differentiate between mild and moderate/severe dry eye. Variability in measurements and inter-eye variability has also been shown to be an indicator of dry eye disease and, in an audit of our own data at Vision Eye Institute, we found that to be a relatively good indicator.41-43 Another newer technology, which provides greater accuracy in dry eye screening, is objective non-invasive tear break up time measurements using the Peramis (Schwind platform) and Keratograph (pentacam). Traditional measurement using fluoroscein and slit lamp observation has multiple potential sources of variability, including the method of fluoroscein instillation and concentration of the fluorescein delivered. Established risk factors for dry eye have been published in many studies, including the most recent update of the Dry Eye Workshop DEWS II.44,45 These include higher myopic corrections, autoimmune disease, female gender, Asian ethnicity and older age.

Figure 2. Efficacy indices of LASIK treatment for three myopic categories in dioptres (D) and overall efficacy index from 1998 to 2007.16
SMILE laser eye surgery has been a game changer for my more myopic patients. Many studies and a few meta-analyses have shown that dry eye incidence and severity is less in SMILE compared to LASIK and similar to PRK.23,24 Due to the smaller ‘key-hole’ incision, as opposed to the larger ‘flap’ of LASIK, corneal sensitivity is less affected and recovers more quickly. Use of artificial tears with SMILE has also been shown to be less, at six months post-operatively.
Neuropathic pain most likely plays a significant role in dry eye symptoms after laser. An interesting new study looked at using perioperative pregabalin administration for one day before and 14 days after LASIK to see if dry eye symptoms were reduced compared to placebo.46 Pregabalin is an analgesic which has been found to reduce the incidence and severity of persistent pain after many other surgeries, including mastectomy, thoracotomy, and hernia repair. Unfortunately, this study did not show any effect from the pregabalin, but the approach is novel and deserves further study. Another study looked at using smartphone data to identify risk factors for dry eye in a more complete way.47 Traditional history taking is subject to errors and omissions and given most of us have our phones with us nearly all of the time and usually keep them on, then this may be the most accurate history taker of all. Calcineurin inhibitors, such as cyclosporine, have been shown to aid with neural healing post laser eye surgery and the recent approval of two topical immunomodulators (Xiidra and Cequa) by the TGA gives us further tools to address dry eye.48
PRESBYOPIA: THE LAST FRONTIER
One of my mentor’s mantras is that presbyopia will never be solved by a corneal procedure and one of my colleagues has a similar mantra that nothing should be inserted into the centre of the cornea except cornea. I am a great believer in wisdom based on experience and, for this reason I have watched, as a bystander, as various devices such as corneal inlays and laser ablations such as intracor and presbyLASIK have been implemented by other surgeons. The only laser procedure I have done for presbyopia is monovision due to its safety, reversibility, demonstrability and lesser induction of optical aberrations, which might limit options and increase the difficulty of cataract surgery in the future.

Figure 3. The iFix pen.
Monovision still, after many innovations, remains the dominant preferred method for presbyopia correction among surveyed surgeons. I am always upfront with patients, advising them that monovision does not fix their presbyopia – it’s more like a detour around it. While not the subject of this article, I view presbyopia correcting intraocular lenses (IOLs) as a considerably more successful and popular method for correcting presbyopia than corneal based procedures (though these IOLs have their limitations as well). Part of the success of presbyopia correcting IOLs comes down to presbyopia being a lens-based problem, which means that logically, the correction should occur there.32,49,50
Therefore, my bold prediction for the future of presbyopia correction is that it will be non-surgical and definitely non-corneal. Presbyopia correcting eye drops hold the most promise at present. The early phase of these are mostly miotics which increase depth of focus and again, provide more of an optical trick method of correcting presbyopia rather than a true cure. Lipoic acid choline ester chloride is currently in phase 2 trials (Novartis Pharmaceuticals). This eye drop reduces the disulfide bonds that form between proteins within the crystalline lens and in animal studies was shown to increase lens elasticity by 40%. As a new presbyope, and someone just starting to wear reading glasses, I must say I have a slight personal interest.
CONCLUSIONS
Laser vision correction continues to be one of the stand out leaders as an elective procedure in terms of patient satisfaction, accuracy and safety. However, there is and should be a continuous drive for further improvement. A better understanding of the factors that play a role in the small subset who have variable reactions to laser vision correction is essential, and machine learning with big data may hold the key to unlocking results that we mere human ophthalmologists can only aspire to.
To earn your CPD points from this article visit mieducation.com/laser-vsion-correction-pastpresent- and-future
Associate Professor Colin Chan is an internationally recognised expert in vision correction procedures, including laser eye surgery (LASIK, SMILE and ASLA/PRK), refractive lens exchange and laser cataract surgery. He has more than 18 years’ experience as an eye surgeon and has performed over 7,000 eye surgery procedures. A/Prof Chan also specialises in the treatment of corneal conditions, with a focus on keratoconus and pterygium.
He has expertise in techniques such as corneal ring implants (Intacs and Kerarings), collagen cross-linking and corneal transplants. He is an Adjunct Associate Professor at the University of Canberra (Faculty of Health) and a Senior Clinical Lecturer at the University of Sydney. A/Prof Chan is also a Director of the Refractive Surgery Degree at the University of Sydney (Save Sight Institute).
References
- Rao, S.N. and R.J. Epstein, Early onset ectasia following laser in situ keratomileusus: case report and literature review. J Refract Surg, 2002. 18(2): p. 177-84.
- Piccoli, P.M., A.A. Gomes, and F.V. Piccoli, Corneal ectasia detected 32 months after LASIK for correction of myopia and asymmetric astigmatism. J Cataract Refract Surg, 2003. 29(6): p. 1222-5.
- Argento, C., et al., Corneal ectasia after laser in situ keratomileusis. J Cataract Refract Surg, 2001. 27(9): p. 1440-8.
- Randleman, J.B., et al., Risk factors and prognosis for corneal ectasia after LASIK. Ophthalmology, 2003. 110(2): p. 267-75.
- Chan, C.C., C. Hodge, and G. Sutton, External analysis of the Randleman Ectasia Risk Factor Score System: a review of 36 cases of post LASIK ectasia. Clin Exp Ophthalmol, 2010. 38(4): p. 335-40.
- Wolle, M.A., J.B. Randleman, and M.A. Woodward, Complications of Refractive Surgery: Ectasia After Refractive Surgery. Int Ophthalmol Clin, 2016. 56(2): p. 127-39.
- Bohac, M., et al., Incidence and Clinical Characteristics of Post LASIK Ectasia: A Review of over 30,000 LASIK Cases. Semin Ophthalmol, 2018. 33(7-8): p. 869-877.
- Hirji, N., et al., Corneal collagen crosslinking for keratoconus or corneal ectasia without epithelial debridement. Eye (Lond), 2015. 29(6): p. 764-8.
- Li, G., Z.J. Fan, and X.J. Peng, Corneal collagen crosslinking for corneal ectasia of post-LASIK: one-year results. Int J Ophthalmol, 2012. 5(2): p. 190-5.
- Guo, H., S.M. Hosseini-Moghaddam, and W. Hodge, Corneal biomechanical properties after SMILE versus FLEX, LASIK, LASEK, or PRK: a systematic review and metaanalysis. BMC Ophthalmol, 2019. 19(1): p. 167.
- Serbecic, N., et al., Repeatability and reproducibility of corneal biomechanical parameters derived from Corvis ST. Eur J Ophthalmol, 2019: p. 1120672119864554.
- Terai, N., et al., Identification of biomechanical properties of the cornea: the ocular response analyzer. Curr Eye Res, 2012. 37(7): p. 553-62.
- Ambrosio, R., Jr., et al., Scheimpflug imaging for laser refractive surgery. Curr Opin Ophthalmol, 2013. 24(4): p. 310-20.
- Yoo, T.K., et al., Adopting machine learning to automatically identify candidate patients for corneal refractive surgery. NPJ Digit Med, 2019. 2: p. 59.
- Perlman, E.M. and S.E. Reinert, Factors influencing the need for enhancement after laser in situ keratomileusis. J Refract Surg, 2004. 20(6): p. 783-9.
- Yuen, L.H., et al., A 10-year prospective audit of LASIK outcomes for myopia in 37,932 eyes at a single institution in Asia. Ophthalmology, 2010. 117(6): p. 1236-1244 e1.
- Ganesh, S. and R. Gupta, Comparison of visual and refractive outcomes following femtosecond laser- assisted lasik with smile in patients with myopia or myopic astigmatism. J Refract Surg, 2014. 30(9): p. 590-6.
- Zhang, Y., et al., Clinical Outcomes of SMILE and FS-LASIK Used to Treat Myopia: A Meta-analysis. J Refract Surg, 2016. 32(4): p. 256-65.
- Shen, Z., et al., Dry Eye after Small Incision Lenticule Extraction (SMILE) versus Femtosecond Laser-Assisted in Situ Keratomileusis (FS-LASIK) for Myopia: A Meta-Analysis. PLoS One, 2016. 11(12): p. e0168081.
- Shen, Z., et al., Small Incision Lenticule Extraction (SMILE) versus Femtosecond Laser-Assisted In Situ Keratomileusis (FS-LASIK) for Myopia: A Systematic Review and Meta-Analysis. PLoS One, 2016. 11(7): p. e0158176.
- Taneri, S., et al., [Experience with Introduction of SMILE: Learning Phase of our First 200 Treatments]. Klin Monbl Augenheilkd, 2017. 234(1): p. 70-76.
- Kobashi, H., K. Kamiya, and K. Shimizu, Dry Eye After Small Incision Lenticule Extraction and Femtosecond Laser-Assisted LASIK: Meta-Analysis. Cornea, 2017. 36(1): p. 85-91.
- Wong, A.H.Y., et al., Dry Eyes After SMILE. Asia Pac J Ophthalmol (Phila), 2019. 8(5): p. 397-405.
- Sambhi, R.S., et al., Dry eye after refractive surgery: a meta-analysis. Can J Ophthalmol, 2020. 55(2): p. 99-106.
- Han, T., et al., Refractive outcomes comparing SMILE and FS-LASIK for High Myopia. J Cataract Refract Surg, 2020.
- Artini, W., et al., Predictive Factors for Successful High Myopia Treatment Using High-Frequency Laser-In-Situ Keratomileusis. Open Ophthalmol J, 2018. 12: p. 214-225.
- Mimouni, M., et al., Factors Predicting the Need for Retreatment After Laser Refractive Surgery. Cornea, 2016. 35(5): p. 607-12.
- Gomel, N., et al., Predictive factors for efficacy and safety in refractive surgery for myopia. PLoS One, 2018. 13(12): p. e0208608.
- Xi, L., C. Zhang, and Y. He, Single-step Transepithelial photorefractive keratectomy in the treatment of mild, moderate, and high myopia: six month results. BMC Ophthalmol, 2018. 18(1): p. 209.
- Adib-Moghaddam, S., et al., Efficacy and safety of transepithelial photorefractive keratectomy. J Cataract Refract Surg, 2018. 44(10): p. 1267-1279.
- Jiang, J., et al., Comparison of visual quality after Femto-LASIK and TransPRK in patients with low and moderate myopia. Int Ophthalmol, 2020. 40(6): p. 1419-1428.
- Achiron, A., et al., Predicting Refractive Surgery Outcome: Machine Learning Approach With Big Data. J Refract Surg, 2017. 33(9): p. 592-597.
- Sharma, M., B.S. Wachler, and C.C. Chan, Higher order aberrations and relative risk of symptoms after LASIK. J Refract Surg, 2007. 23(3): p. 252-6.
- Schallhorn, S.C., et al., Pupil size and quality of vision after LASIK. Ophthalmology, 2003. 110(8): p. 1606-14.
- Lee, Y.C., F.R. Hu, and I.J. Wang, Quality of vision after laser in situ keratomileusis: influence of dioptric correction and pupil size on visual function. J Cataract Refract Surg, 2003. 29(4): p. 769-77.
- Villa, C., et al., Night vision disturbances after successful LASIK surgery. Br J Ophthalmol, 2007. 91(8): p. 1031-7.
- Chan, A. and E.E. Manche, Effect of preoperative pupil size on quality of vision after wavefront-guided LASIK. Ophthalmology, 2011. 118(4): p. 736-41.
- Schallhorn, S., et al., The role of the mesopic pupil on patient-reported outcomes in young patients with myopia 1 month after wavefront-guided LASIK. J Refract Surg, 2014. 30(3): p. 159-65.
- Damgaard, I.B., et al., Functional Optical Zone and Centration Following SMILE and LASIK: A Prospective, Randomized, Contralateral Eye Study. J Refract Surg, 2019. 35(4): p. 230-237.
- Liu, Q., et al., Review on Centration, Astigmatic Axis Alignment, Pupil Size and Optical Zone in SMILE. Asia Pac J Ophthalmol (Phila), 2019. 8(5): p. 385-390.
- Wolffsohn, J.S., et al., TFOS DEWS II Diagnostic Methodology report. Ocul Surf, 2017. 15(3): p. 539-574.
- Gupta, P.K., et al., Prevalence of ocular surface dysfunction in patients presenting for cataract surgery evaluation. J Cataract Refract Surg, 2018. 44(9): p. 1090-1096.
- Potvin, R., S. Makari, and C.J. Rapuano, Tear film osmolarity and dry eye disease: a review of the literature. Clin Ophthalmol, 2015. 9: p. 2039-47.
- Craig, J.P., et al., TFOS DEWS II Report Executive Summary. Ocul Surf, 2017. 15(4): p. 802-812.
- Jones, L., et al., TFOS DEWS II Management and Therapy Report. Ocul Surf, 2017. 15(3): p. 575-628.
- Galor, A., et al., Pregabalin Failed to Prevent Dry Eye Symptoms after Laser-Assisted in Situ Keratomileusis (LASIK) in a Randomized Pilot Study. J Clin Med, 2019. 8(9).
- Inomata, T., et al., Characteristics and Risk Factors Associated With Diagnosed and Undiagnosed Symptomatic Dry Eye Using a Smartphone Application. JAMA Ophthalmol, 2019.
- Peyman, G.A., et al., Cyclosporine 0.05% ophthalmic preparation to aid recovery from loss of corneal sensitivity after LASIK. J Refract Surg, 2008. 24(4): p. 337-43.
- Labiris, G., et al., Mini-monovision versus multifocal intraocular lens implantation. J Cataract Refract Surg, 2015. 41(1): p. 53-7.
- Goldberg, D.G., et al., Pseudophakic mini-monovision: high patient satisfaction, reduced spectacle dependence, and low cost. BMC Ophthalmol, 2018. 18(1): p. 293.





